
Located within the Robert W. Franz Cancer Center in Portland, Ore., the Earle A. Chiles Research Institute is a leader in immuno-oncology, and home to a team of world-renowned scientists and physicians. With expertise in cancer immunotherapy, clinical and translational research, and training programs spanning the continuum of higher education, it provides a rich environment for immuno-oncology fellowship.
-

Manual Scalp Cooling in Early Stage Breast Cancer: Value of Caretaker Training and Patient-Reported Experience to Optimize Efficacy and Patient Selection
Manaz Rezayee, Nikki Moxon, Staci Mellinger, Amanda Y Seino, Nicole E. Fredich, Tracy L. Kelly, Susan Mulligan, Patrick Rossi, Ijeoma Uche, Walter Urba, Alison Conlin, Janet Ruzich, and David B Page
Title:
Manual scalp cooling in early stage breast cancer: value of caretaker training and patient-reported experience to optimize efficacy and patient selection
Authors:
Manaz Rezayee1, BS Nicole Moxon1, RN Staci Mellinger1, RN Amanda Y. Seino1 Nicole E. Fredrich1 Tracy L. Kelly1 Susan Mulligan2, MA Patrick Rossi3, MD Ijeoma Uche1, MD Walter J. Urba1, MD PHD Alison K. Conlin1, MD MPH Janet Ruzich1, DO David B. Page1, MD
Background:
Alopecia is an emotionally distressing common adverse effect of curative-intent chemotherapy in early stage breast cancer.1–6 Although machine-based scalp cooling is effective for reduction of chemotherapy-associated alopecia in early stage breast cancer, availability is geographically limited.7–11 Manual cold-cap systems may also be effective and are available regardless of geographic location.12–14 We evaluated the feasibility of caretaker-administered cold-cap efficacy following structured standardized training, and utilized patient-reported subjective outcomes to develop a clinical tool to facilitate patient selection.
Patients and Methods:
A small pilot study (n=10) was conducted to evaluate the feasibility and efficacy of manual cold capping. Key eligibility criteria included: 1) no hair loss at baseline; 2) no pre-existing scalp condition; 3) planned curative-intent chemotherapy for early stage breast cancer and 4) availability of caretaker(s). Participants received standardized training and then performed the cold-cap procedure without assistance. The primary endpoint was post-treatment hair retention using Dean’s alopecia scale, with success defined as
Results:
Of the evaluable patients, 80% (n=8/10) met the primary efficacy endpoint (Dean’s scale 0-2) with 20% (n=2/10) trial failures due to pre-mature discontinuation. Manual cold-capping was worthwhile to 90% of patients (Was it Worth It? Questionnaire) and associated with favorable PROs. Patient interviews identified a number of themes shared by almost all patients, which were subsequently used to develop a questionnaire to aid patient-directed decision-making on whether to pursue manual cold-capping.
Conclusion:
This study affirms the safety and efficacy of manual cold-capping to reduce alopecia and demonstrates the importance of proper training and education to maximize efficacy. It also highlights the considerable costs and effort associated with cold-capping. Selected patients with early stage breast cancer may benefit subjectively from cold capping while the proposed clinical instrument can be used to facilitate an informed discussion between patient and provider.
-
 Experience by Sarah Tu and Shuntao Cai")
PD-1 and PD-L1 Inhibitors: A Single Center Medication Assistance Program (MAP) Experience
Sarah Tu and Shuntao Cai
PD-1 and PD-L1 Inhibitors: A Single Center Medication Assistance Program (MAP) Experience
Sarah Tu, PharmD and Shuntao Cai, PharmD, BCOP
Robert W. Franz Cancer Center, Providence Cancer Institute, Portland, OR, USA
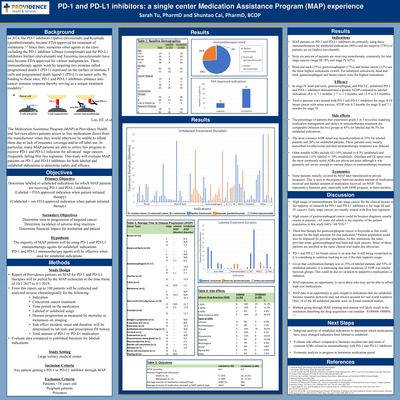
Background: PD-1 and PD-LI inhibitors are a large component of the growing immuno-oncology field and every year there are increasing studies investigating potential indications for these agents. This IRB approved retrospective chart review examines patients in the Medication Assistance Program (MAP) within a large tertiary medical center who are on PD-1 and PD-L1 medications due to financial barriers and/or non-FDA approved regimens (unlabeled indications). This study seeks to evaluate efficacy and safety of PD-1 and PD-L1 for unlabeled vs labeled indications within this population.
Methods: One hundred MAP patients treated with the PD-1 and PD-L1 inhibitors Opdivo (nivolumab), Keytruda (pembrolizumab) and Imfinzi (durvalumab) from October 2017- August 2019 will be analyzed in a reverse chronological order. The following data will be collected from the EMR: patient age, gender, medication, indication, duration of therapy, duration of therapy, labeled or unlabeled usage, if patient had a response, time to disease progression, concurrent therapies, total amount of drug administered, noted side effects, and if the FDA indication has changed since initiation. Labeled indications will be defined as medications that are FDA approved for the patient’s cancer type at time of medication initiation. Unlabeled medications are those not FDA approved for a patient’s cancer type at time of medication initiation. Evaluation of provider notes, lab tests and medication history records will be the primary data source for information collected. Primary objectives include evaluation of labeled vs unlabeled indications for PD-1 and PD-L1 inhibitors. Secondary objectives include determining time to disease progression, incidence of adverse drug reactions, and financial impact for institution and patient.
Results: Out of one hundred patients analyzed, 20% were on PD-1 and PD-L1 inhibitors for labeled indications and 80% patients were treated for unlabeled indications. The top three indications for PD-1 and PD-L1 inhibitors overall were head and neck (35%), gastroesophageal (17%), and breast cancer (12%) which was primarily driven by unlabeled patients. In stage IV head and neck, gastroesophageal, and NSCLC, unlabeled PD-1 and PD-L1 inhibitors demonstrated a greater average time to disease state progression compared to labeled indications (8.6 vs 7.3 months, 2.7 vs 1.1 months and 12.9 vs 0.5 months). The percentage of patients with grade 2 and 3 toxicities were comparable between the unlabeled and labeled indications with total incidence of ADR at 45% for labeled indications and 46.3% for unlabeled indications. The most common ADR requiring medications or delay of therapy was hypothyroidism (25% in labeled and 20% in unlabeled).
Conclusions: The majority of MAP patients are on PD-1 and PD-L1 inhibitors for unlabeled indications with the highest usage of Opdivo (nivolumab) at 74%. From our small sample size, there is promising data that PD-1 and PD-L1 inhibitors may prolong survival for several months longer for various indications including breast cancer, stage IV head and neck, gastroesophageal and NSCLC. These indications may later be incorporated into clinical trials as these agents seek new drug approvals.




{kind=link}
{kind=link}