
-

Increasing HPV Vaccination Rates at PMG Milwaukie Family Medicine
Sean Brachvogel, Justin Ferley, Jessica Hu, Lauren Moore, Sebastian Reeve, Tyler Reimann, John Yates, and Daniel Ruegg
Background
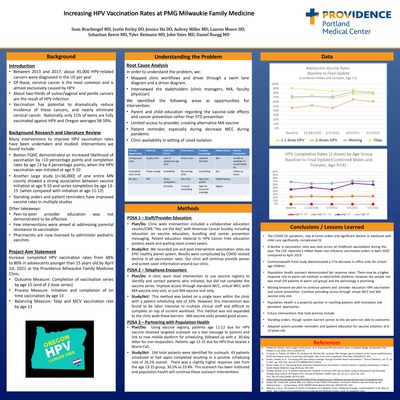
Introduction • Between 2013 and 2017 about 45 000 HPV related cancers were diagnosed in the US per year • Of these, cervical cancer is the most common and is almost exclusively caused by HPV • About two thirds of vulvar/vaginal and penile cancers are the result of HPV infection • Vaccination has potential to dramatically reduce incidence of these cancers, and nearly eliminate cervical cancer Nationally, only 51 of teens are fully vaccinated against HPV and Oregon averages 58 59 Background Research and Literature Review Many interventions to improve HPV vaccination rates have been undertaken and studied Interventions we found include • Boston FQHC demonstrated an increased likelihood of vaccination by 10 percentage points and completion rates by age 13 by 4 percentage points, when the HPV vaccination was initiated at age 9 10 • Another large study ( 36 000 of one entire MN county showed a strong association between vaccine initiation at age 9 10 and series completion by age 13 15 (when compared with initiation at age 11 12 • Standing orders and patient reminders have improved vaccine rates in multiple studies Other takeaways • Peer to peer provider education was not demonstrated to be effective • Few interventions were aimed at addressing parental resistance to vaccination • Pharmacists are now licensed to administer pediatric vaccines Project Aim Statement Increase completed HPV vaccination rates from 68 to 80 in adolescents younger than 15 years old by April 1 st, 2021 at the Providence Milwaukie Family Medicine Clinic • Outcome Measure Completion of vaccination series by age 15 (end of 2 dose series) • Process Measure initiation and completion of on time vaccination by age 13 • Balancing Measure Tdap and MCV vaccination rate by age 13
Understanding the Problem
Root Cause Analysis In order to understand the problem, we • Mapped clinic workflows and driver through a swim lane diagram and a driver diagram • Interviewed the stakeholders (clinic managers, MA, faculty physician) We identified the following areas as opportunities for intervention • Parent and child education regarding the vaccine side effects and cancer prevention rather than STD prevention • Limited access to provider, creating alternative MA vaccine • Patient reminder, especially during decrease WCC during pandemic • Clinic availability in setting of covid isolation
Methods
PDSA 1 Staff/Provider Education • Plan/Do Clinic wide intervention included a collaborative education session/CME "You are the Key" with American Cancer Society, including education on vaccine education, bundling and cancer prevention messaging Patient education material in HPV Cancer Free education posters, exam and waiting room screen savers • Study/Act We recorded pre and post intervention vaccination rates via EPIC healthy planet system Results were complicated by COVID related decline in all vaccination rates Our clinic will continue provide poster and screen saver information around our clinic PDSA 2 Telephone Encounters • Plan/Do A clinic team level intervention to use vaccine registry to identify and contact patients who initiated, but did not complete the vaccine series Improve access through standard WCC, virtual WCC with MA vaccine only visit, or just MA vaccine visit only • Study/Act This method was tested on a single team within the clinic with a patient scheduling rate of 33 However, this intervention was found to be labor intensive to multiple clinical staff and difficult to complete on top of current workload This method was not expanded to the clinic wide these barriers MA vaccine visits proved good access PDSA 3 Partnering with Population Health • Plan/Do Using vaccine registry, patients age 11 12 due for HPV vaccine received targeted outreach via a text message to parents and link to new mobile platform for scheduling, followed up with a 30 day letter for non responders Patients age 13 15 due for HPV that receive a Warm Call • Study/Act 164 total patients were identified for outreach 43 patients scheduled or had appts completed resulting in a positive scheduling rate of 26 2 overall There was a slightly higher response rate from the age 13 15 group, 30 5 vs 23 8 This outreach has been instituted and population health will continue these outreach interventions
Conclusions/Lessons Learned
The COVID 19 pandemic, stay at home orders and significant decline in adolscent well child care significantly complicated QI • A decline in vaccination rates was seen across all childhood vaccinations during this year. The CDC reported 3 million fewer non influenza vaccination orders in April 2020 compared to April 2019 • Commonwealth Fund study demonstrated a 71% decrease in office visits for school age children. • Population Health outreach demonstrated fair response rates. There may be a higher response rate to warm call methods vs text/mobile platform, however the sample size was small (59 patients in warm call group) and the technology is promising. • Moving forward we plan to continue patient and provider education HPV vaccination and cancer prevention. Continue providing access through virtual WCC and MA vaccine only visit. • Population Health is a powerful partner in reaching patients with innovative and persistent approaches. • Future interventions that hold promise include: • Standing orders, though system barriers persist to this we were not able to overcome. • Adopted system provider reminders and [ patient education for vaccine initiation at 9 10 years old.
-

Critical Conversations: Improving Goals of Care Conversations at Southeast Family Medicine
Elizabeth Deyo, Michael Dirks, Tyler Nelson, Katherine Cobb, Nicholas Wolfgang, Hannah Kadavy, and Ben Pederson
Quality Improvement Project - Background
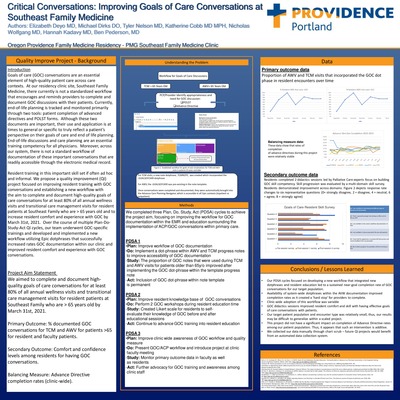
Introduction Goals of care (GOC) conversations are an essential element of high quality patient care across care contexts. At our residency clinic site, Southeast Family Medicine, there currently is not a standardized workflow that encourages and reminds providers to complete and document GOC discussions with their patients. Currently, end of life planning is tracked and monitored primarily through two tools: patient completion of advanced directives and POLST forms. Although these two documents are important, their use and application is at times to general or specific to truly reflect a patient’s perspective on their goals of care and end of life planning. End of life discussions and care planning are an essential training competency for all physicians. Moreover, across our system, there is not a standard workflow of documentation of these important conversations that are readily accessible through the electronic medical record. Resident training in this important skill set if often ad hoc and informal. We propose a quality improvement (QI) project focused on improving resident training with GOC conversations and establishing a new workflow with the aim to complete and document high quality goals of care conversations for at least 80% of all annual wellness visits and transitional care management visits for resident patients at Southeast Family who are > 65 years old and to increase resident comfort and experience with GOC by March 31st, 2021. Over the course of multiple Plan Do Study Act QI cycles, our team underwent GOC specific trainings and developed and implemented a new workflow utilizing Epic dotphrases that successfully increased rates GOC documentation within our clinic and improved resident comfort and experience with GOC conversations. Project Aim Statement We aimed to complete and document high quality goals of care conversations for at least 80% of all annual wellness visits and transitional care management visits for resident patients at Southeast Family who are > 65 years old by March 31st, 2021. Primary Outcome: % documented GOC conversations for TCM and AWV for patients >65 for resident and faculty patients. Secondary Outcome: Comfort and confidence levels among residents for having GOC conversations. Balancing Measure: Advance Directive completion rates (clinic wide).
Methods
We completed three Plan, Do, Study, Act (PDSA) cycles to achieve the project aim, focusing on improving the workflow for GOC documentation within the EMR and education surrounding the implementation of ACP/GOC conversations within primary care. PDSA 1 • Plan: Improve workflow of GOC documentation • Do: Implement a dot phrase within AWV and TCM progress notes to improve accessibility of GOC documentation - Study: The proportion of GOC notes that were used during TCM and AWV visits for patients older than 65y/o improved after implementing the GOC dot phrase within the template progress note - Act: Inclusion of GOC dot phrase within note template is permanent PDSA 2 • Plan: Improve resident knowledge base of GOC conversations • Do: Perform 2 GOC workshops during resident education time - Study: Created Likert scale for residents to self evaluate their knowledge of GOC before and after educational sessions - Act: Continue to advance GOC training into resident education PDSA 3 • Plan: Improve clinic wide awareness of GOC workflow and quality measure • Do: Present GOC/ACP workflow and introduce project at clinic faculty meeting - Study: Monitor primary outcome data in faculty as well as residents - Act: Further advocacy for GOC training and awareness among clinic staff
Conclusions/Lessons Learned
• Our PDSA cycles focused on developing a new workflow that integrated new dotphrases and resident education led to a sustained near goal completion rate of GOC conversations for our target population. • Availability of system wide dotphrases within the AVW documentation improved completion rates as it created a 'hard stop' for providers to complete. • Clinic wide adoption of this workflow was variable • GOC didactics sessions improved resident comfort and skill with having effective goals of care conversations with patients. • Our target patient population and encounter type was relatively small, thus, our results may be difficult to generalize within a scaled project. • This project did not have a significant impact on completion of Advance Directive rates among our patient population. Thus, it appears that such an intervention is additive. • We collected our data manually through chart scrub future QI projects would benefit from an automated data collection system.
Providence Oregon Family Medicine Residency is a 21-resident program under the direction of Justin Osborn, M.D. This community hospital program has been accredited by the Accreditation Council for Graduate Medical Education (ACGME) since 2000 and is the sole residency at Providence Milwaukie. Our program is located just six miles from the center of downtown Portland, Ore.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}