
-
, and Cerebrovascular Accident (CVA). by Jonathan Aguilar Roa and Evon Anukam")
Health Disparities in Black, Latinx, and Native Populations Compared to Caucasians: A Retrospective Descriptive-Analysis of Care Focused on Hypertensive Emergency, Non-ST Segment Elevation Myocardial Infarction (NSTEMI), and Cerebrovascular Accident (CVA).
Jonathan Aguilar Roa and Evon Anukam
Background
• Health disparity is a sum of differences in healthcare seen in underserved populations of the United States. 1 • Differences include incidence, prevalence, mortality, burden of disease, and other adverse health conditions • According to ASHP, health disparities continue to be a major public health problem confronting the U.S. health care systems. 2 • Evidence suggests that health disparities can be in part due to differences in the quality of care for different racial and ethnic groups. 2 • All the different disparity factors have been shown to lead to different health outcomes that do not favor Black, Latinx, and Native American populations. • ASHP believes health-system pharmacists have both a professional and moral obligation to take part in initiatives that work towards erasing any racial and ethnic disparities in healthcare. 2 • Examples of ways pharmacists can make an impact are: • Increase awareness among fellow caregivers • Ensure effective communication by volunteering for leadership roles • Enforce consistency of using evidence-based therapy for all patients • Analyze data for outcomes sorted by racial minorities • Per ASHP there are three general principles that serve as guides for pharmacist to help erase healthcare disparities: 2 1. All patients have the right to high-quality care, by taking leadership roles pharmacists can partake in initiatives to increase access to care. 2. Medication-use practices should reflect knowledge of, sensitivity to, and respect for the race and culture of the patient. 3. Health-system pharmacists have a vital role to play in eliminating racial and ethnic disparities in health care.
Purpose
Evaluate and compare how two large tertiary hospitals have provided prompt evidence based medical therapy to Blacks, Latinx, and Natives, in comparison to Caucasians pertaining to hypertensive emergency, non- ST segment elevation myocardial infarction (NSTEMI), and cerebrovascular accident (CVA)
Objective
Determine what differences there may be in providing various non-medication/medication interventions and time-to-intervention order placement after arrival to the emergency department (ED)
Methodology
• Institutional Review Board (IRB) – approved • Double center, observational, descriptive-analysis, retrospective review, spanning 51 months (January 1st, 2017, to March 31st, 2021), of adults presenting to ED at either of the two large tertiary hospitals. • Inclusion criteria • Black, Latinx, Native American, and Caucasian adults (> 18 years old) presenting to the ED with primary diagnosis of NSTEMI, hypertensive emergency, or CVA. • Exclusion criteria • < 18 years old; patients not meeting the pre-specified race/ethnicity criteria; primary diagnosis outside of hypertensive emergency, NSTEMI, or CVA
Discussion
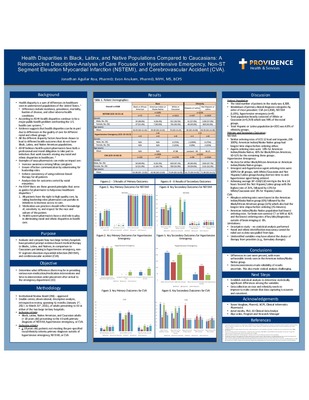
Patient Population • The total number of patients in the study was 4,308. • Breakdown of primary clinical diagnosis categories by order of most prevalent: CVA (n=1,858), NSTEMI (1,695), hypertensive emergency (n=8) • Total population heavily consisted of White or Caucasian (n=3,359) which was 94% of the racial groups. • Total Hispanic or Latino population (n=207) was 4.8% of ethnicity groups. Primary and Secondary Outcomes: NSTEMI: • Similar ordering rates of ECG 12 lead and troponin, (98- 100%). American Indian/Alaska Native group had longest time elapse before ordering either. • Aspirin ordering rates were 18% for American Indian/Alaska Native, 43% for Black/African American, 50-51% for the remaining three groups . Hypertensive Emergency: • No data for either Black/African American or American Indian/Alaska Native groups. • Emergent anti-hypertensive agent ordering rates were 100% for all groups, with White/Caucasian and Not Hispanic/Latino groups having shortest time-to antihypertensive agent being ordered. • Achieving average BP <160/110 mmHg in the first 24 hours favored the Not Hispanic/Latino group with the highest rate of 25%, followed by 13% for White/Caucasian and 0% for Hispanic/Latino. CVA: • Alteplase ordering rates were lowest in the American Indian/Alaska Native group (6%) followed by the Black/African American group (11%) which also had the longest time elapse before ordering (76 minutes). • American Indian/Alaska Native population had lowest ordering rates for brain non-contrast CT or MRI at 41% and the lowest ordering rates of key labs/diagnostics outside of brain imaging at 6%. Limitations: • Descriptive study – no statistical analysis performed • Racial and ethnic identification inaccuracy cannot be ruled out as data was pulled from Epic. • Unidentified variables may have altered the choice of therapy from providers (e.g., formulary changes)
Conclusions
• Differences in care were present, with more unfavorable trends seen in the American Indian/Alaska Native group. • Data inconsistencies made reliability of results uncertain. This also made statical analysis challenging.
-

Pharmacist Pilot Project to Reduce Hypoglycemic Events on Internal Medicine Unit
Carly Barnes and Pamela Levine
-
 Project by Hyesoo Chae, Sharon Leigh, and Colleen M Casey")
Medication and Pharmacy-Related Outcomes As Part Of The Seniors At Risk For Falls after Emergency Room Visit (SAFER) Project
Hyesoo Chae, Sharon Leigh, and Colleen M Casey
Background
The United States is comprised of an aging population; adults over the age of 85 are the fastest-growing age group in the United States and will reach approximately 9 million in 2030.1 25% of patients ≥ 65 years old in the United States report falling each year.1 There are over 3 million emergency department visits related to falls in the United States, totaling approximately 50 billion dollars in total medical expenditures.2 Falls are a major threat for older adults as they can lead to increased risk of further injury, loss of independence, decreased mobility, and premature death.1,2 Despite numerous studies showing evidence that multifactorial fall risk interventions are effective in decreasing fall risk, older adults who have an injurious fall often do not receive meaningful interventions to mitigate their fall risk. 3,4,5 Polypharmacy and high-risk medication (HRM) use is one such modifiable fall risk factor. In 2015, it was estimated that 29% of older adults in the United States had filled at least one medication listed in the Beers Criteria. Studies have demonstrated that primary care pharmacists can help bridge that gap and play an important role in the interdisciplinary healthcare team by identifying and intervening to reduce HRMs use in older adults.7 The Seniors At risk for Falls after Emergency Room visits (SAFER) project was created in 2018 to better serve seniors greater than 75 years of age who go to the Emergency Room for a fall, increase coordinated services, improve various outcome measures, and appreciate cost savings for delivery side and health plan with less costly services. SAFER provides a structured pathway to help teams provide tailored care to at-risk seniors.
Purpose
Falls continue to be a significant cause of morbidity and mortality in older adults, with falls accounting for 70% of accidental deaths in patients who are 75 years of age or older.1 This project is a sub-analysis of a larger multi-clinic study examining multifactorial fall-risk interventions in the primary care setting. The purpose of this project is to describe medication and pharmacy-related variables for both an intervention and matched control group of patients 75 years of age and older admitted to the Emergency Department (ED) for a fall and quantitively assess the outcome of interventions.
Methods
This project was a retrospective comparative cohort analysis of patients in the SAFER project in four Providence Medical Group (PMG) primary care clinics from December 2018 to June 2019 in the Portland metro area. Inclusion criteria included patients who were active PMG patients at a SAFER pilot clinic, ≥75 years, prescribed ≥1 highrisk medication associated with increased falls, and went to the ED for a fall. Exclusion criteria included no clinic visits in the previous two years, enrollment in hospice or hospitalization, skilled nursing facility discharge, and death within two weeks of ED visit. For purposes of analysis, patients were matched by age, gender, Stopping Elderly Accidents, Deaths, and Injuries (STEADI) fall risk score and geographic location: eastside, westside, and southern Oregon and stratified by the STEADI score. A comparator group of patients who met inclusion criteria but were not enrolled in the SAFER project were used as a matched control group. Descriptive statistics include: patient demographics across control and intervention groups; occurrence of pharmacy (PharmD) consults during and after the formal intervention period; whether patients were on Vitamin D3; and changes in HRMs.
Discussion
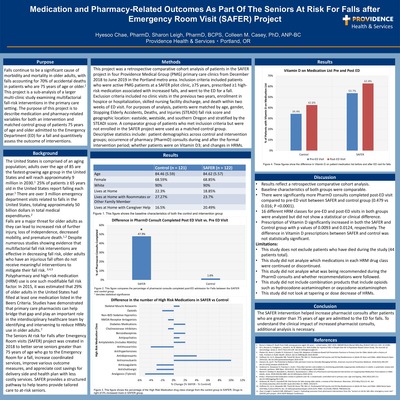
• Results reflect a retrospective comparative cohort analysis. • Baseline characteristics of both groups were comparable. • There were significantly more PharmD consults completed post-ED visit compared to pre-ED visit between SAFER and control group (0.479 vs 0.016; P <0.0001). • 16 different HRM classes for pre-ED and post-ED visits in both groups were analyzed but did not show a statistical or clinical difference. • Prescription of Vitamin D significantly increased in both the SAFER and Control group with p values of 0.0093 and 0.0124, respectively. The difference in Vitamin D prescriptions between SAFER and control was not statistically significant. Limitations: • This study does not exclude patients who have died during the study (44 patients total). • This study did not analyze which medications in each HRM drug class were continued or discontinued. • This study did not analyze what was being recommended during the PharmD consults and whether recommendations were followed. • This study did not include combination products that include opioids such as hydrocodone-acetaminophen or oxycodone-acetaminophen • This study did not look at tapering or dose decrease of HRMs.
Conclusion
The SAFER intervention helped increase pharmacist consults after patients who are greater than 75 years of age are admitted to the ED for falls. To understand the clinical impact of increased pharmacist consults, additional analysis is necessary.
-
 by Jacqueline Figueras, Loann Wong, and Sharon Leigh")
Evaluate opioid prescribing trends for ElderPlace, a Program for All-inclusive Care for the Elderly (PACE)
Jacqueline Figueras, Loann Wong, and Sharon Leigh
Background
• Providence ElderPlace in Oregon is the fifth-largest PACE program in the country that offers wraparound nursing home-eligible medical and social services to over 1600 community-dwelling seniors who are medically frail with complex medication regimens. • Many elderly patients suffer from chronic nonmalignant pain which may affect their function and quality of life. • The Centers for Disease Control and Prevention (CDC) reports a 7.7% increase in drug overdoses and opioid deaths in the aging population from 2013 to 2014. • In 2015-2016 elderly adults obtained an annual average of 774 Morphine Milligram Equivalents (MME) of outpatient prescriptions for chronic & acute pain. • Multiple comorbidities and age-related changes may affect distribution, metabolism, and elimination, older adults are at increased risk of adverse drug events and reactions. • Physician prescribing practices has been shown to play an important role in high rates of prescription opioid use and misuse.
Purpose
To determine trends in opioid prescribing for chronic pain in geriatric patients enrolled with Providence ElderPlace in Oregon
Objectives
Discuss trends in opioid prescribing for chronic pain in geriatric patients at Providence ElderPlace • Determine if opioids are being safely prescribed at Providence ElderPlace • Identify potential gaps that can be addressed to improve opioid prescribing safety
Methodology
• Institutional Review Board (IRB) exempt • Retrospective electronic health record (EHR) based study of multiple ElderPlace clinic sites in Oregon. • All patients meeting inclusion criteria were included • Study population: • Providence ElderPlace participants on routine opioids for chronic pain only (>6 months). • Study period: • March 1, 2020 – October 1, 2020 • Exclusion criteria: • Palliative care Stage 2 and Stage 3 • Outcomes: • Primary: Trends in opioid prescribing using surrogate markers such as: • Average MEDD • Functional goals of therapy • Alternative therapy offered/provided • Informed consent • ElderPlace protocol use • Safety: Falls and opioid-related hospitalizations
Discussion
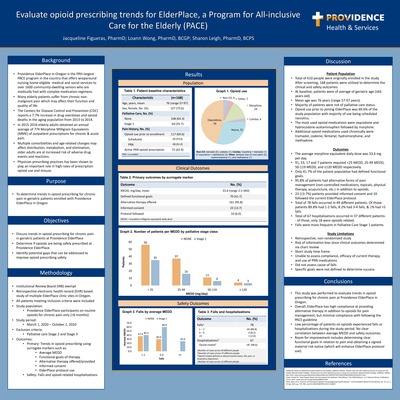
Patient Population • Total of 610 people were originally enrolled in the study. After screening, 168 patients were utilized to determine the clinical and safety outcomes. • At baseline, patients were of average of geriatric age (≥65 years old) • Mean age was 76 years (range 57-97 years). • Majority of patients were not of palliative care status. • Opioid use prior to joining ElderPlace was 69.6% of the study population with majority of use being scheduled narcotics. • The most used opioid medications were oxycodone and hydrocodone-acetaminophen followed by morphine. • Additional opioid medications used chronically were tramadol, codeine, fentanyl, hydromorphone, and methadone. Outcomes • The average morphine equivalent daily dose was 33.6 mg per day. • 91, 53, 17 and 7 patients required <25 >MEDD, 25-49 MEDD, 50-119 MEDD, and ≥120 MEDD respectively. • Only 41.7% of the patient population had defined functional goals. • 95.8% of patients had alternative forms of pain management (non-controlled medications, topicals, physical therapy, acupuncture, etc.) in addition to opioids. • 23 (13.7%) patients provided informed consent and 10 followed the current ElderPlace protocol. • Total of 78 falls occurred in 49 different patients. Of those patients 89.8% had 1-2 falls, 8.2% had 3-4 falls, & 2% had >5 falls. • Total of 67 hospitalizations occurred in 37 different patients- - of those, only 18 were opioids related. • Falls were more frequent in Palliative Care Stage 1 patients. Study Limitations • Retrospective, non-randomized study • Risk of information bias since clinical outcomes determined via chart review • Short study time frame • Unable to assess compliance, efficacy of current therapy, and use of PRN medications • Did not assess cause of falls • Specific goals were not defined to determine success
Conclusions
This study was performed to evaluate trends in opioid prescribing for chronic pain at Providence ElderPlace in Oregon. • Overall, ElderPlace has high compliance at providing alternative therapy in addition to opioids for pain management, but minimal compliance with following the PACE guideline • Low percentage of patients on opioids experienced falls or hospitalizations during the study period. No clear correlation between average MEDD and safety outcomes. • Room for improvement includes determining clear functional goals in relation to pain and obtaining a signed material risk notice (which will enhance ElderPlace protocol use).
-
 by Caleb Galindo, Pamela Levine, and Melanie Geer")
Review of Prophylactic Anticoagulation Strategies and Outcomes for COVID-19 Patients (Research in Progress)
Caleb Galindo, Pamela Levine, and Melanie Geer
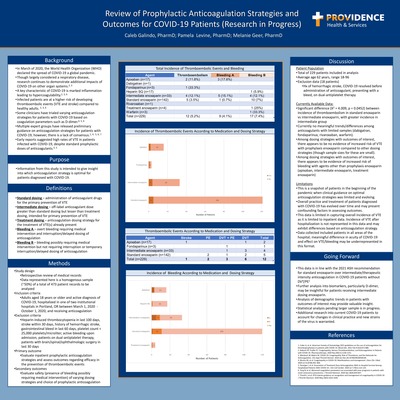
Background
In March of 2020, the World Health Organization (WHO) declared the spread of COVID-19 a global pandemic. •Though largely considered a respiratory disease, research continues to demonstrate additional impacts of COVID-19 on other organ systems.2, 3 •A key characteristic of COVID-19 is marked inflammation leading to hypercoagulability.2, 3, 6 •Infected patients are at a higher risk of developing thromboembolic events (VTE and stroke) compared to healthy adults. 2, 3, 6 •Some clinicians have trialed varying anticoagulation strategies for patients with COVID-19 based on coagulation parameters such as D-dimer.4, 5, 6 •Multiple expert groups have released preliminary guidance on anticoagulation strategies for patients with COVID-19; however, there is a lack of consensus.1, 4, 5, 6, 7 •Early reports suggested high rates of VTE in patients infected with COVID-19, despite standard prophylactic doses of anticoagulants.3, 5
Purpose Information from this study is intended to give insight into which anticoagulation strategy is optimal for patients diagnosed with COVID-19.
Definitions
• Standard dosing –administration of anticoagulant drugs for the primary prevention of VTE •Intermediate dosing –off-label anticoagulant dose greater than standard dosing but lesser than treatment dosing, intended for primary prevention of VTE •Treatment dosing –anticoagulation dosing strategy for the treatment of VTE(s) already present •Bleeding A –overt bleeding requiring medical intervention and interruption/delayed dosing of anticoagulation •Bleeding B –bleeding possibly requiring medical intervention but not requiring interruption or temporary interruption/delayed dosing of anticoagulation
Methods
• Study design •Retrospective review of medical records •Data represented here is a homogenous sample (~50%) of a total of 473 patient records to be analyzed •Inclusion criteria •Adults aged 18 years or older and active diagnosis of COVID-19, hospitalized in one of two institutional hospitals in Portland, OR between March 1, 2020 -October 1, 2020, and receiving anticoagulation •Exclusion criteria •Heparin-induced thrombocytopenia in last 100 days, stroke within 30 days, history of hemorrhagic stroke, gastrointestinal bleed in last 60 days, platelet count < 25,000 platelets/microliter, active bleeding upon admission, patients on dual-antiplatelet therapy, patients with brain/spinal/ophthalmologic surgery in last 30 days •Primary outcome •Evaluate inpatient prophylactic anticoagulation strategies and assess outcomes regarding efficacy in the prevention of thromboembolic events •Secondary outcomes •Evaluate safety (presence of bleeding possibly requiring medical intervention) of varying dosing strategies and choice of prophylactic anticoagulation
Discussion
Patient Population •Total of 229patients included in analysis •Average age 62 years, range 18-96 •Exclusion data (18 patients) •Hx of hemorrhagic stroke, COVID-19 resolved before administration of anticoagulant, presenting with a bleed, on dual-antiplatelet therapy Currently Available Data: •Significant difference (X2= 4.009, p = 0.0452) between incidence of thromboembolism in standard enoxaparin vs intermediate enoxaparin, with greater incidence in intermediate group •Currently no meaningful trends/differences among anticoagulants with limited samples (dabigatran, fondaparinux, rivaroxaban, warfarin). •Among dosing strategies with outcomes of interest, there appears to be no evidence of increased risk of VTE with prophylaxis enoxaparin compared to other dosing strategies (though sample sizes for these are small). •Among dosing strategies with outcomes of interest, there appears to be evidence of increased risk of bleeding with agents other than prophylaxis enoxaparin (apixaban, intermediate enoxaparin, treatment enoxaparin) Limitations •This is a snapshot of patients in the beginning of the pandemic when clinical guidance on optimal anticoagulation strategies was limited and evolving. •Overall practice and treatment of patients diagnosed with COVID-19 has evolved over time and may present confounding factors in assessing outcomes. •This data is limited in capturing overall incidence of VTE as it is limited to inpatient data. Incidence of VTE after hospitalization is not represented in this data and may exhibit differences based on anticoagulation strategy. •Data collected included patients in all areas of the hospital; meaningful difference in acuity of COVID-19 and effect on VTE/bleeding may be underrepresented in this format.
Going Forward
• This data is in line with the 2021 ASH recommendation for standard enoxaparin over intermediate/therapeutic intensity anticoagulation in COVID-19 patients without DVT/PE1 •Further analysis into biomarkers, particularly D-dimer, may be insightful for patients receiving intermediate dosing enoxaparin. •Analysis of demographic trends in patients with outcomes of interest may provide valuable insight. •Statistical analysis pending larger sample is in progress. •Additional research into current COVID-19 patients to account for changes in clinical practice and new strains of the virus is warranted.
-

Evaluation of Surgical Antibiotic Prophylaxis Compliance at a Large, Tertiary Medical Center
Meagan Greckel and Brent Footer
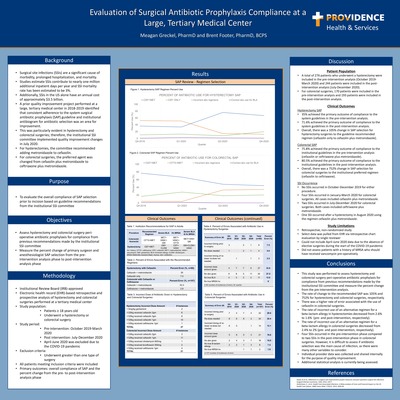
Background
• Surgical site infections (SSIs) are a significant cause of morbidity, prolonged hospitalization, and mortality. •Studies estimate SSIs contribute to nearly one million additional inpatient days per year and SSI mortality rate has been estimated to be 3%. •Additionally, SSIs in the US alone have an annual cost of approximately $3.5 billion. •A prior quality improvement project performed at a large, tertiary medical center in 2018-2019 identified that consistent adherence to the system surgical antibiotic prophylaxis (SAP) guideline and institutional antibiogram for antibiotic selection was an area for improvement. •This was particularly evident in hysterectomy and colorectal surgeries; therefore, the institutional SSI committee implemented quality improvement changes in July 2020. •For hysterectomies, the committee recommended adding metronidazole to cefazolin. •For colorectal surgeries, the preferred agent was changed from cefazolin plus metronidazole to ceftriaxone plus metronidazole.
Purpose To evaluate the overall compliance of SAP selection prior to incision based on guideline recommendations from the institutional SSI committee
Objectives
• Assess hysterectomy and colorectal surgery peri-operative antibiotic prophylaxis for compliance from previous recommendations made by the institutional SSI committee •Measure the percent change of primary surgeon and anesthesiologist SAP selection from the pre-intervention analysis phase to post-intervention analysis phase
Methodology
Institutional Review Board (IRB)-approved •Electronic health record (EHR)-based retrospective and prospective analysis of hysterectomy and colorectal surgeries performed at a tertiary medical center •Study population: •Patients ≥ 18 years old •Underwent a hysterectomy or colorectal surgery •Study period: •Pre-intervention: October 2019-March 2020 •Post intervention: July-December 2020 •April-June 2020 was excluded due to the COVID-19 pandemic •Exclusion criteria: •Underwent greater than one type of surgery •All patients meeting inclusion criteria were included •Primary outcomes: overall compliance of SAP and the percent change from the pre-to post-intervention analysis phase
Discussion
Patient Population •A total of 276 patients who underwent a hysterectomy were included in the pre-intervention analysis (October 2019-March 2020) and 244 patients were included in the post-intervention analysis (July-December 2020). •For colorectal surgeries, 170 patients were included in the pre-intervention analysis and 193 patients were included in the post-intervention analysis. Clinical Outcomes Hysterectomy SAP •35% achieved the primary outcome of compliance to the system guidelines in the pre-intervention analysis. •71.6% achieved the primary outcome of compliance to the system guidelines in the post-intervention analysis. •Overall, there was a 105% change in SAP selection for hysterectomy surgeries to the guideline recommended regimen (cefazolin only to cefazolin plus metronidazole). Colorectal SAP •75.8% achieved the primary outcome of compliance to the institutional guidelines in the pre-intervention analysis (cefazolin or ceftriaxone plus metronidazole). •80.5% achieved the primary outcome of compliance to the institutional guidelines in the post-intervention analysis. •Overall, there was a 752% change in SAP selection for colorectal surgeries to the institutional preferred regimen (cefazolin to ceftriaxone). SSI Occurrence •No SSIs occurred in October-December 2019 for either procedure. •Four SSIs occurred in January-March 2020 for colorectal surgeries. All cases included cefazolin plus metronidazole. •Two SSIs occurred in July-December 2020 for colorectal surgeries. Both cases included ceftriaxone plus metronidazole. •One SSI occurred after a hysterectomy in August 2020 using the regimen cefazolin plus metronidazole. Study Limitations •Retrospective, non-randomized study •Select data was pulled from EHR via retrospective chart evaluation by single reviewer •Could not include April-June 2020 data due to the absence of elective surgeries during the start of the COVID-19 pandemic •Did not assess patients with a history of MRSA who should have received vancomycin pre-operatively
Conclusions
This study was performed to assess hysterectomy and colorectal surgery peri-operative antibiotic prophylaxis for compliance from previous recommendations made by the institutional SSI committee and measure the percent change from the pre-intervention analysis. •The rate of change to the recommended SAP was 105% and 752% for hysterectomy and colorectal surgeries, respectively. •There was a higher rate of error associated with the use of cefazolin in colorectal surgeries. •The rate of incorrect use of an alternative regimen for a beta-lactam allergy in hysterectomies decreased from 2.6% to 1.6% (pre-and post-intervention, respectively). •The rate of incorrect use of an alternative regimen for a beta-lactam allergy in colorectal surgeries decreased from 2.4% to 2% (pre-and post-intervention, respectively). •Four SSIs occurred in the pre-intervention phase compared to two SSIs in the post-intervention phase in colorectal surgeries. However, it is difficult to assess if antibiotic selection was the main cause of infection, as there were many other variables to consider. •Individual provider data was collected and shared internally for the purpose of quality improvement. •Additional statistical analysis is currently being assessed.
-

Evaluation of specialty pharmacy productivity metrics to create an updated standardized productivity tool
Linda Huynh, Adam Saulles, and Amber Franck
Background
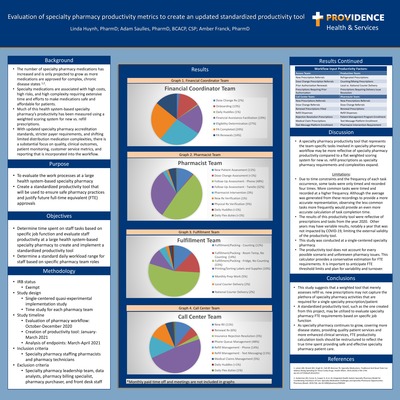
• The number of specialty pharmacy medications has increased and is only projected to grow as more medications are approved for complex, chronic disease states 1,2 • Specialty medications are associated with high costs, high risks, and high complexity requiring extensive time and efforts to make medications safe and affordable for patients. • Much of this health system based specialty pharmacy’s productivity has been measured using a weighted scoring system for new vs. refill prescriptions. • With updated specialty pharmacy accreditation standards, stricter payer requirements, and shifting limited distribution medication complexities, there is a substantial focus on quality, clinical outcomes, patient monitoring, customer service metrics, and reporting that is incorporated into the workflow.
Purpose
To evaluate the work processes at a large health system based specialty pharmacy • Create a standardized productivity tool that will be used to ensure safe pharmacy practices and justify future full time equivalent (FTE) approvals
Objectives
Determine time spent on staff tasks based on specific job function and evaluate staff productivity at a large health system based specialty pharmacy to create and implement a standardized productivity tool • Determine a standard daily workload range for staff based on specific pharmacy team roles
Methodology
• IRB status • Exempt • Study design • Single centered quasi experimental implementation study • Time study for each pharmacy team • Study timeline • Evaluation of pharmacy workflow: October December 2020 • Creation of productivity tool: January March 2021 • Analysis of endpoints: March April 2021 • Inclusion criteria • Specialty pharmacy staffing pharmacists and pharmacy technicians • Exclusion criteria • Specialty pharmacy leadership team, data analysts, pharmacy billing specialist, pharmacy purchaser, and front desk staff
Discussion
• A specialty pharmacy productivity tool that represents the team specific tasks involved in specialty pharmacy workflow may be more reflective of specialty pharmacy productivity compared to a flat weighted scoring system for new vs. refill prescriptions as specialty pharmacy requirements and complexities expand. Limitations • Due to time constraints and the frequency of each task occurrence, some tasks were only timed and recorded four times. More common tasks were timed and recorded at a higher frequency. Although the average was generated from these recordings to provide a more accurate representation, observing the less common tasks more frequently would provide an even more accurate calculation of task completion time. • The results of this productivity tool were reflective of prescriptions and tasks from the year 2020. Other years may have variable results, notably a year that was not impacted by COVID 19, limiting the external validity of the productivity tool. • This study was conducted at a single centered specialty pharmacy. • The productivity tool does not account for every possible scenario and unforeseen pharmacy issues. This calculator provides a conservative estimation for FTE requirements. It is important to anticipate FTE threshold limits and plan for variability and turnover.
Conclusions
• This study suggests that a weighted tool that merely assesses refill vs. new prescriptions may not capture the plethora of specialty pharmacy activities that are required for a single specialty prescription/patient • A standardized productivity tool, such as the one created from this project, may be utilized to evaluate specialty pharmacy FTE requirements based on specific job function • As specialty pharmacy continues to grow, covering more disease states, providing quality patient services and more enhanced clinical services, FTE productivity calculation tools should be restructured to reflect the true time spent providing safe and effective specialty pharmacy patient care.
-

Appropriateness of Sugammadex usage within the OR
Kevin Johansen and Bryce Winn
Background
Sugammadex is a unique neuromuscular reversal drug used to counteract the effects of the aminosteroidnon-depolarizing muscle relaxing drugs; rocuronium and vecuronium •Neuromuscular blocking agents (NMBs) are frequently used in surgical procedures to assist with intubation, patient immobilization, etc. •Sugammadex, a synthetic cyclodextrin molecule, encapsulates rocuronium (and vecuronium, pancuronium) rendering it inactive •Onset of action of rocuronium is within 1-2 minutes, duration of action is about 30 minutes, though t1/2elimination is between 1.4-2.4 hours and true duration varies greatly patient to patient •Sugammadex pharmacokinetic/dynamic profile: non-protein bound, unchanged renal elimination, onset of action < 3 min, t1/2 : 2 hours •Sugammadex is an expensive medication, and so far, there are no guidelines or criteria in place to ensure its use is optimized and that overuse and waste are minimized •The medication comes in 2 vial sizes: 200 mg/2 mL, and 500 mg/5 mL •Providence Oregon P&T committee has put forth suggested appropriate use criteria for the use of Sugammadex within the OR •The purpose of this project is to evaluate the impact of these criteria, and to assess the current cost and potential cost savings obtainable through criteria justifying the use of sugammadex •Goals include: •Ensuring appropriate vial sizes are used to minimize waste and reduce hospital costs •Interpreting whether the use, and dose of sugammadex is justified •Evaluate the impact of the P&T committee’s proposed appropriate use criteria
Objectives
Primary outcomes •Evaluate appropriateness of sugammadex use •Identify methods of reducing waste and achieve cost savings through implementation of appropriate use criteria •Secondary outcomes •Assess impact of appropriate use criteria as put forth by system P&T committee
Methods
Study design •Retrospective •Utilization review of OR cases from March,2020 through October 2020 •Cases randomly selected •Inclusion criteria •All OR cases within the time frame during which sugammadex was administered •Exclusion criteria •N/A
Discussion
Results •Proposed appropriate use criteria encourages restriction of sugammadex dosing to max of 200 mg for patients weighing•Doses greater than 200 mg should be reserved for more complex scenarios, requiring justification for increased dose and subsequent larger vial (5 mL) size use •Use criteria evaluated include: •Age > 70 •Overall poor health (ASA >3) •Surgical cases < 1 hour Findings: •Currently, dosing varies drastically, ranging from as low as 1.11 mg/kg, to 5.71 mg/kg •Literature states that NMB reversal can be seen by 2 mg/kg, though new literature suggests this threshold may be lower than previously thought •In addition to this, appropriate vial selection reaches only 29% of administered sugammadex doses, indicating much room for improvement and potential cost savings of upwards of $3,475 •Furthermore, of the 58 cases studied, only 21 (36%) of them had sugammadex administered within 2 hours of last rocuronium administration. Considering rocuronium’s short half life, cases lasting longer than this are less likely to require sugammadex as time goes on •Selected appropriate use criteria (age > 70, ASA >3, case time <1>hour) indicate that implementation of these criteria would drastically reduce sugammadex use Exceptional finding: •One patient received 400 mg sugammadex (5.71 mg/kg) though zeroNMB agent was used during the case Data Limitations •Not all proposed appropriate use criteria put forth by P&T committee were able to be evaluated in this study
Conclusions & Next Steps
• Improved justification of sugammadex dosage selection would result in drastic reduction of medication waste, and subsequent cost savings • Primary focus should be placed on maintaining a max of 200 mg of sugammadex, unless other criteria are met in certain circumstances • In addition to that, adhering to a strict 2 mL vial selection for doses of <200>mg, would have saved $3,474 dollars for a sample size of 58 alone, without factoring in additional savings with appropriate dose selection • It is important to note that sugammadex does have benefits and is associated with reduced PACU/post-op recovery time compared to neostigmine/glycopyrrolate • Further approval of the proposed appropriate use criteria and buy in from anesthesia to adhere to these criteria would reduce patient exposure to unnecessarily high doses of sugammadex, and result in minimization of waste and increased cost savings
-

Evaluation and Implementation of a New Phenobarbital Protocol for Alcohol Withdrawal Management in the Emergency Department
Sarah J. Kim, Sara Clark, and Joshua L. Floyd
Background
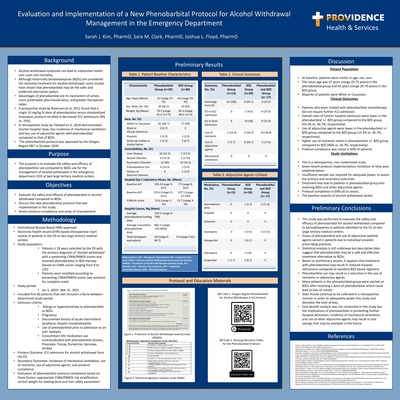
• Alcohol withdrawal syndrome can lead to substantial health care costs and mortality. • Although historically benzodiazepines (BZDs) are considered the mainstay treatment for alcohol withdrawal, some studies have shown that phenobarbital may be the safer and preferred alternative option. • Advantages of phenobarbital are its mechanism of action, more predictable pharmacokinetics, and greater therapeutic index. • A prospective study by Rosenson et al. 2012 found that a single 10 mg/kg IV dose of phenobarbital versus standardized lorazepam protocol resulted in decreased ICU admissions (8% vs. 25%). • A retrospective study by Tidewell et al. 2018 demonstrated shorter hospital stays, less incidence of mechanical ventilation and less use of adjunctive agents with phenobarbital compared to that of BZDs. • The phenobarbital protocol was approved by the Oregon Region P&T in October 2020.
Purpose
• The purpose is to evaluate the safety and efficacy of phenobarbital use compared to BZDs use for the management of alcohol withdrawal in the emergency department (ED) at two large tertiary medical centers.
Objectives
• Evaluate the safety and efficacy of phenobarbital in alcohol withdrawal compared to BZDs. • Discuss the new phenobarbital protocol that was implemented in this study. • Assess protocol compliance and areas of improvement.
Methodology
• Institutional Review Board (IRB)-approved • Electronic health record (EHR)-based retrospective chart review of patients in the ED at two large tertiary medical centers • Study population: • Patients ≥ 18 years admitted to the ED with the primary diagnosis of ‘alcohol withdrawal’ with a presenting CIWA/PAWSS scores and received phenobarbital or BZD therapy (based on CIWA scores ranging from 9 to >25) • Patients were stratified according to presenting CIWA/PAWSS scores (see protocol for complete scale) • Study period: • Jan 1, 2020– Mar 31, 2021 • Included first 60 patients that met inclusion criteria between determined study period • Exclusion criteria: • Allergy or hypersensitivity to phenobarbital or BZDs • Pregnancy • Documented history of acute intermittent porphyria, hepatic encephalopathy • Use of phenobarbital prior to admission as an anti- epileptic • Concomitant HIV medication use contraindicated with phenobarbital (Evotaz, Prezcobix, Tivicay, Doravirine, Genvoya, Stribild • Primary Outcome: ICU admission for alcohol withdrawal from the ED • Secondary Outcomes: Incidence of mechanical ventilation, use of restraints, use of adjunctive agents, and protocol compliance • Evaluation of phenobarbital protocol compliance based on three factors: appropriate CIWA/PAWSS risk stratification, correct weight for loading dose and met safety parameters
Discussion
Patient Population • At baseline, patients were similar in age, sex, race. • The mean age was 47 years (range 25-75 years) in the phenobarbital group and 45 years (range 29-70 years) in the BZD group. • Majority of patients were White or Caucasian. Clinical Outcomes • Patients who were treated with phenobarbital monotherapy did not require further ICU admission. • Overall rates of further hospital admission were lower in the phenobarbital +/- BZD group compared to the BZD group (43.3% vs. 56.7%, respectively). • Use of adjunctive agents were lower in the phenobarbital +/- BZD group compared to the BZD group (13.3% vs. 26.7%, respectively). • Higher use of restraints noted in phenobarbital +/- BZD group compared to BZD (40% vs. 16.7%, respectively). • Protocol compliance was noted in 60% of patients. Study Limitations • This is a retrospective, non-randomized study. • Given recent protocol implementation, limitation of time post implementation • Insufficient sample size required for adequate power to assess the primary and secondary outcomes • Treatment bias due to patients in phenobarbital group also receiving BZDs and other adjunctive agents. • Protocol compliance is difficult to assess. • The baseline severity of alcohol withdrawal varied.
Preliminary Conclusions
• This study was performed to evaluate the safety and efficacy of phenobarbital for alcohol withdrawal compared to benzodiazepines in patients admitted to the ED at two large tertiary medical centers. • Doses of phenobarbital and use of adjunctive sedative agents varied in patients due to individual provider prescribing practices. • Statistical analysis is still underway but descriptive data suggest that phenobarbital may be a safe and effective treatment alternative to BZDs. • Based on preliminary results, it appears that treatment with phenobarbital may result in reduced hospital admissions compared to standard BZD based regimens. • Phenobarbital use may result in a reduction in the use of restraints or adjunctive agents. • Many patients in the phenobarbital group were started on BZDs after receiving a dose of phenobarbital, which could lead to bias of results. • Data should continue to be collected in a retrospective manner in order to adequately power this study and decrease the level of bias. • Cost benefit analysis was not conducted in this study but the implications of phenobarbital in preventing further hospital admission, incidence of mechanical ventilation, and use of other adjunctive agents may result in cost savings that may be analyzed in the future.
-

Fixed Dose Prothrombin Complex Concentrate Versus Weight-Based Dose for Warfarin Reversal
Peter Martsin and Bryce Winn
Background
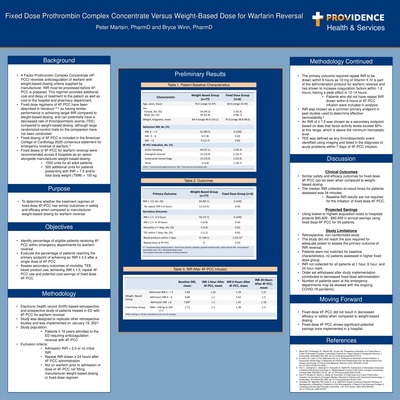
•4 Factor Prothrombin Complex Concentrate (4F-PCC) reverses anticoagulation of warfarin with weight-based dosing criteria supplied by manufacturer. INR must be processed before 4F-PCC is prepared. This regimen provides additional cost and delay of treatment to the patient as well as cost to the hospital and pharmacy department. •Fixed dose regimens of 4F-PCC have been described in literature1,2-4as having similar performance in achieving target INR compared to weight-based dosing, and can potentially have a decreased rate of thromboembolic events (TEE) compared to weight-based dosing, although large randomized-control trials on the comparison have not been conducted. •Fixed dosing of 4F-PCC is included in the American College of Cardiology 2020 consensus statement for emergency reversal of warfarin.5 •Fixed doses of 4F-PCC for warfarin reversal were recommended across 8 hospitals as an option alongside manufacturer weight-based dosing: •1500 units for all adult patients •500 additional units for patients presenting with INR > 7.5 and/or total body weight (TBW) > 100 kg
Purpose •To determine whether the treatment regimen of fixed dose 4F-PCC has similar outcomes in safety and efficacy when compared to manufacturer weight-based dosing for warfarin reversal
Objectives
•Identify percentage of eligible patients receiving 4F-PCC within emergency departments for warfarin reversal •Evaluate the percentage of patients reaching the primary endpoint of achieving an INR ≤ 2.0 after a single dose of 4F-PCC •Assess secondary outcomes of mortality, TEE, blood product use, achieving INR ≤ 1.5, repeat 4F-PCC use and potential cost-savings of fixed dose 4F-PCC
Methodology
Table 2. Outcomes •Electronic health record (EHR)-based retrospective and prospective study of patients treated in ED with 4F-PCC for warfarin reversal •Study was designed to replicate other retrospective studies and was implemented on January 19, 2021 •Study population: •Patients ≥ 18 years admitted to the ED requiring anticoagulation reversal with 4F-PCC •Exclusion criteria: •Admission INR < 2.0 or no initial INR •Repeat INR drawn ≥ 24 hours after 4F-PCC administration •Not on warfarin prior to admission or dose of 4F-PCC not fitting manufacturer weight-based dosing or fixed dose regimen
The primary outcome required repeat INR to be drawn within 6 hours as 10 mg of Vitamin K IV is part of the administration protocol for warfarin reversal and has shown to increase coagulation factors within 1-2 hours, having a peak effect in 12-14 hours. •Patients who did not have repeat INR drawn within 6 hours of 4F-PCC infusion were included in analysis. •INR was chosen as a common primary endpoint in past studies used to determine effective hemostability.2 •An INR of ≤ 1.5 was chosen as a secondary endpoint based on data that factor activity levels exceed 80% at this range, which is above the minimum hemostatic level. •TEE was defined as any thromboembolic event identified using imaging and listed in the diagnosis of acute problems within 7 days of 4F-PCC infusion.
Discussion
Clinical Outcomes •Similar safety and efficacy outcomes for fixed dose 4F-PCC can be seen when compared to weight-based dosing. •The median INR collection-to-result times for patients assessed was 34 minutes. •Baseline INR results are not required for the initiation of fixed dose 4F-PCC. Projected Savings •Using lowest to highest acquisition costs to hospitals projects $45,600 -$80,400 in annual savings using fixed dose 4F-PCC for 55 patients. Study Limitations •Retrospective, non-randomized study •The study did not reach the size required for adequate power to assess the primary outcome of INR reversal. •Patients were not matched for baseline characteristics, no patients assessed in higher fixed dose group. •INR not collected for all patients at 1 hour, 6 hour, and 24 hour mark. •Order set withdrawal after study implementation contributed to decreased fixed dose administration. •Number of patients seen at the emergency departments may be skewed with the ongoing COVID-19 pandemic.
Moving Forward
•Fixed dose 4F-PCC did not result in decreased efficacy or safety when compared to weight-based dosing. •Fixed dose 4F-PCC shows significant potential savings once implemented in a hospital.
-

Financial impact of a regional antimicrobial stewardship cost saving initiative in a large integrated health care system
Van Nguyen, Colton Taylor, Alyssa B Christensen, and Brent Footer
Background
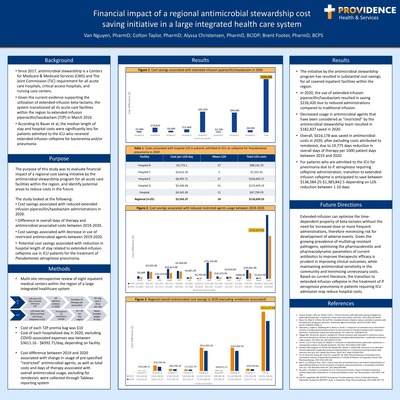
• Since 2017, antimicrobial stewardship is a Centers for Medicare & Medicaid Services (CMS) and The Joint Commission (TJC) requirement for all acute care hospitals, critical access hospitals, and nursing care centers. •Given the current evidence supporting the utilization of extended-infusion beta-lactams, the system transitioned all its acute care facilities within the region to extended-infusion piperacillin/tazobactam (TZP) in March 2016 •According to Bauer et al, the median length of stay and hospital costs were significantly less for patients admitted to the ICU who received extended-infusion cefepime for bacteremia and/or pneumonia
Purpose
The purpose of this study was to evaluate financial impact of a regional cost saving initiative by the antimicrobial stewardship program for all acute care facilities within the region, andidentify potential areas to reduce costs in the future. The study looked at the following: •Cost savings associated with reduced extended-infusion piperacillin/tazobactam administrations in 2020. •Difference in overall days of therapy and antimicrobial-associated costs between 2019-2020. •Cost savings associated with decrease in use of restricted antimicrobial agents between 2019-2020. •Potential cost savings associated with reduction in hospital length of stay related to extended-infusion cefepime use in ICU patients for the treatment of Pseudomonas aeruginosa pneumonia.
Methods
• Multi-site retrospective review of eight inpatient medical centers within the region of a large integrated healthcare system •Cost of each TZP premix bag was $10 •Cost of each hospitalized day in 2020, excluding COVID-associated expenses was between $3611.16 -$8392.71/day, depending on facility •Cost difference between 2019 and 2020 associated with change in usage of pre-specified “restricted” antimicrobial agents, as well as total costs and days of therapy associated with overall antimicrobial usage, excluding for remdesivir, were collected through Tableau reporting system
Results
• The initiative by the antimicrobial stewardship program has resulted in substantial cost savings for all covered inpatient facilities within the region. •In 2020, the use of extended-infusion piperacillin/tazobactamresulted in saving $226,420 due to reduced administrations compared to traditional infusion. •Decreased usage in antimicrobial agents that have been considered as “restricted” by the antimicrobial stewardship team resulted in $182,837 saved in 2020. •Overall, $616,178 was saved in antimicrobial costs in 2020, after excluding costs attributed to remdesivir, due to 19,775 days reduction in overall days of therapy per 1000 patient days between 2019 and 2020. •For patients who are admitted to the ICU for pneumonia due to P. aeruginosarequiring cefepime administration, transition to extended-infusion cefepime is anticipated to save between $138,584.25-$1,385,842.5 depending on LOS reduction between 1-10 days
Future Directions Extended-infusion can optimize the time-dependent property of beta-lactams without the need for increased dose or more frequent administrations, therefore minimizing risk for development of adverse events. Given the growing prevalence of multidrug-resistant pathogens, optimizing the pharmacokinetic and pharmacodynamic parameters of current antibiotics to improve therapeutic efficacy is prudent in improving clinical outcomes, while maintaining antimicrobial sensitivity in the community and minimizing unnecessary costs. Based on current literature, the transition to extended-infusion cefepime in the treatment of P. aeruginosa pneumonia in patients requiring ICU admission may reduce hospital costs.
-

Evaluation of Provider Adherence to Antibiotic Selection Following the Implementation of Antimicrobial Stewardship Committee Recommendations for the Empiric Treatment of Hospitalized Adults with Urinary Tract Infections
James E. Watkins, Alyssa B Christensen, and Brent Footer
Background
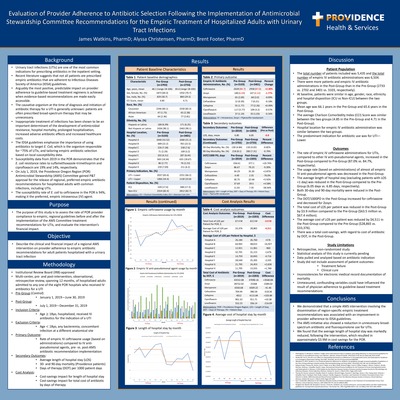
• Urinary tract infections (UTIs) are one of the most common indications for prescribing antibiotics in the inpatient setting. • Recent literature suggests that not all patients are prescribed empiric antibiotics that are adherent to Infectious Diseases Society of America (IDSA) guidelines. • Arguably the most positive, predictable impact on provider adherence to guideline-based treatment regimens is achieved when evidence-based recommendations are made easily accessible. • The causative organism at the time of diagnosis and initiation of antibiotic therapy for a UTI is generally unknown: patients are often prescribed broad-spectrum therapy that may be unnecessary. • Inappropriate treatment of infections has been shown to be an important determinant of the development of antimicrobial resistance, hospital mortality, prolonged hospitalization, increased adverse antibiotic effects and increased healthcare costs. • The IDSA guidelines emphasize the importance of using antibiotics to target E. Coli, which is the organism responsible for ~75% of UTIs, and tailoring empiric antibiotic selection based on local susceptibility data. • Susceptibility data from 2019 in the POR demonstrates that the E. coli resistance rates to sulfamethoxazole-trimethoprim and ciprofloxacin are 19% and 14%, respectively. • On July 1, 2019, the Providence Oregon Region (POR) Antimicrobial Stewardship (AMS) Committee gained P&T approval for the release of regional, preferred empiric antibiotic recommendations for hospitalized adults with common infections, including UTIs. • The susceptibility rate of E. coli to ceftriaxone in the POR is 94%, making it the preferred, empiric intravenous (IV) agent.
Purpose
• The purpose of this study is to assess the rate of POR provider compliance to empiric, regional guidelines before and after the implementation of the AMS Committee treatment recommendations for UTIs, and evaluate the intervention’s financial impact.
Objective
Describe the clinical and financial impact of a regional AMS intervention on provider adherence to empiric antibiotic recommendations for adult patients hospitalized with a urinary tract infection
Methodology
Institutional Review Board (IRB)-approved • Multi-center, pre- and post-intervention, observational, retrospective review, spanning 12 months, of hospitalized adults admitted to any one of the eight POR hospitals who received IV antibiotics for a UTI • Pre-Group (Control): • January 1, 2019—June 30, 2019 • Post-Group: • July 1, 2019—December 31, 2019 • Inclusion Criteria: • Age ≥ 18yo, hospitalized, received IV antibiotics for the indication of a UTI • Exclusion Criteria: • Age < 18yo, any bacteremia, concomitant infection at a different anatomical site • Primary Outcome: • Rate of empiric IV ceftriaxone usage (based on administrations) compared to IV antipseudomonal agents, pre- vs. post-AMS antibiotic recommendation implementation • Secondary Outcomes: • Average length of hospital stay (LOS) • 30- and 90-day mortality (Providence patients) • Days of therapy (DOT) per 1000 patient days • Cost Analysis: • Cost-savings impact for length of hospital stay • Cost-savings impact for total cost of antibiotic by days of therapy
Discussion
Patient Population • The total number of patients included was 5,435 and the total number of empiric IV antibiotic administrations was 6,504. • There were more patients and empiric IV antibiotic administrations in the Post-Group than in the Pre-Group (2733 vs. 2702 and 3401 vs. 3103, respectively). • At baseline, patients were similar in age, gender, race, ethnicity and hospital disposition (ICU vs Non-ICU) between the two groups. • Mean age was 66.1 years in the Pre-Group and 65.6 years in the Post-Group. • The average Charlson Comorbidity Index (CCI) Score was similar between the two groups (4.85 in the Pre-Group and 4.71 in the Post-Group). • Hospital location for empiric IV antibiotic administration was similar between the two groups. • The predominant indication for antibiotic use was for UTI— Lower. Outcomes • The rate of empiric IV ceftriaxone administrations for UTIs, compared to other IV anti-pseudomonal agents, increased in the Post-Group compared to Pre-Group (87.0% vs. 84.7%, respectively). • The usage rate (based on administrations) of almost all empiric IV anti-pseudomonal agents was decreased in the Post-Group. • The average length of hospital stay (excluding patients with LOS <1 >day) was reduced in the Post-Group compared to the Pre- Group (6.05 days vs. 6.85 days, respectively). • Both 30-day and 90-day mortality were reduced in the Post- Group. • The DOT/1000PD in the Post-Group increased for ceftriaxone and decreased for Zosyn. • The total cost of LOS per patient was reduced in the Post-Group by $3.9 million compared to the Pre-Group ($63.5 million vs. $67.4 million). • The average cost of LOS per patient was reduced by $4,511 in the Post-Group compared to the Pre-Group ($28,865 vs. $33,376). • There was a total cost-savings, with regard to cost of antibiotic by DOT, in the Post-Group. Study Limitations • Retrospective, non-randomized study • Statistical analysis of this study is currently pending • Data pulled and analyzed based on antibiotic indication • Study did not include assessment of patient outcomes: • Treatment failure • Clinical cure • Inconsistencies for electronic medical record documentation of mortality • Unmeasured, confounding variables could have influenced the result of physician adherence to guideline-based treatment recommendations
Conclusions
• We demonstrated that a simple AMS intervention involving the dissemination of region-specific empiric treatment recommendations was associated with an improvement in provider adherence to IDSA guidelines. • The AMS initiative also showed a reduction in unnecessary broadspectrum antibiotic and fluoroquinolone use for UTIs. • We found that the average length of hospital stay was markedly reduced, following the intervention, which resulted in approximately $3.9M in cost savings for the POR.
Providence residency programs are built on a tradition of excellence. We offer diverse training in a variety of practice settings, and our award-winning programs are recognized for high-quality patient care.
The PGY1 Pharmacy Residency program has been accredited by ASHP since 1994, offering residents the opportunity to participate in collaborative, integrated care in health system pharmacy practice. Residents apply advanced practice-based skills, expand leadership skills, participate in professional organizations, and participate in innovative approaches to delivery of care.
The PGY1 Pharmacy Residency is one program with two sites: Providence Portland Medical Center and Providence St. Vincent Medical Center. Both Providence Portland Medical Center and Providence St. Vincent Medical Center have implemented a layered learning model, with pharmacy student/resident/attending pharmacist teams on each of the core clinical services, modeled after the medical education model. The teams work collaboratively with health care practitioners to provide patient care and improve medication management across transitions in care. The PGY1 Pharmacy Residency program provides broad experience and confidence in practice-based skills across diverse practice settings while offering the opportunity to obtain focused experience in areas of interest.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}