
-

Overloadipine–Emerging Therapies to Treat Refractory Shock
Stephanie Barayuga and Irene Hendrickson
Introduction
Refractory vasodilatory shock develops from uncontrolled vasodilation and hyporesponsivenessto vasopressors. •Management of calcium channel blockers (CCB) toxicity can be difficult because it can result in refractory vasodilatory
Case Presentation
•21-year-old male with history of depression and prior suicide attempts presented after intentional ingestion of amlodipine (300 mg) and metformin (150 tablets of 1000 mg). •Presented with slightly altered mentation and hypotension, then quickly deteriorated and required intubation and high vasopressor requirements. •Transferred to PSVMC for consideration of venoarterialextracorporeal membrane oxygenation (VA-ECMO). Since he was hyperdynamic on echocardiogram, our team did not feel he would benefit from VA-ECMO. •His vasopressor requirements surpassed the normal recommended doses •Due to no improvement, methylene blue and hydroxycobalamine(vitamin B12) were initiated for his refractory shock. •He responded favorably to this therapy. Norepinephrine dose was halved and Epinephrine down to 10 mcg/min almost immediately. •It took several days to wean him off the vasopressors and he was able to transfer to the medical floor in stable condition.
Discussion
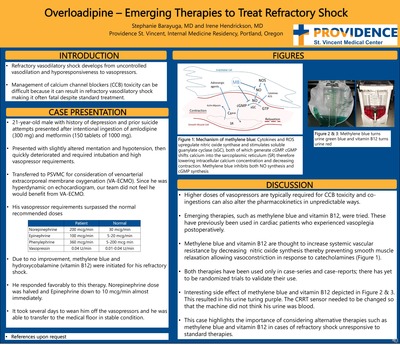
•Higher doses of vasopressors are typically required for CCB toxicity and co-ingestions can also alter the pharmacokinetics in unpredictable ways. •Emerging therapies, such as methylene blue and vitamin B12, were tried. These have previously been used in cardiac patients who experienced vasoplegiapostoperatively. •Methylene blue and vitamin B12 are thought to increase systemic vascular resistance by decreasing nitric oxide synthesis thereby preventing smooth muscle relaxation allowing vasoconstriction in response to catecholamines (Figure 1). •Both therapies have been used only in case-series and case-reports; there has yet to be randomized trials to validate their use. •Interesting side effect of methylene blue and vitamin B12 depicted in Figure 2 & 3. This resulted in his urine turingpurple. The CRRT sensor needed to be changed so that the machine did not think his urine was blood. •This case highlights the importance of considering alternative therapies such as methylene blue and vitamin B12 in cases of refractory shock unresponsive to standard therapies.
-

Are elevated inflammatory markers and acute phase reactants associated with more severe disease in COVID 19 patients?
Joanna Bove, Robert Kim, and Shelley Sanders
Introduction Inflammatory markers and acute phase reactants (from here referred to as “markers”) are associated with COVID-19 infection and may be able to predict disease severity.1,2We collected markers including d-dimer (ug/mL), ferritin (ng/mL), CRP (mg/dL), and creatinine kinase (CK) (IU/L) on admission and periodically throughout the hospital stay for 50 patients admitted with COVID-19 infection. We hypothesized that higher levels of markers at admission and during hospitalization are associated increased severity of disease, such as ICU admission and placement on mechanical ventilation.
Methods From March to May 2020, we identified 50 patients admitted to Providence St. Vincent Medical Center with PCR-confirmed COVID-19 infection. Demographic and laboratory data were obtained through chart review. Statistical analysis including linear regression, t-tests, and chi2 tests were performed to look at the association between markers and severe outcomes including ICU admission, mechanical ventilation, and inpatient mortality. Regression models were adjusted for patients’ age, gender, DM2 status, reported onset of symptoms, and whether the patient was hypoxic at admission. All the statistical analyses were carried out by STATA software (Version 16.1; STATA Corporation, College Station, TX, USA).
Results
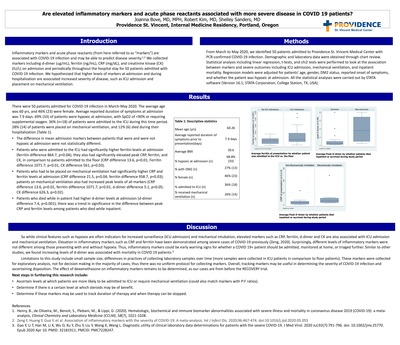
There were 50 patients admitted for COVID-19 infection in March-May 2020. The average age was 60 yrs, and 46% (23) were female. Average reported duration of symptoms at admission was 7.9 days. 69% (33) of patients were hypoxic at admission, with SpO2 of <90% or requiring supplemental oxygen. 36% (n=18) of patients were admitted to the ICU during this time period. 28% (14) of patients were placed on mechanical ventilation, and 12% (6) died during their hospitalization (Table 1). •The difference in mean admission markers between patients that were and were not hypoxic at admission were not statistically different. •Patients who were admitted to the ICU had significantly higher ferritin levels at admission (ferritin difference 864.7, p=0.04); they also had significantly elevated peak CRP, ferritin, and CK, in comparison to patients admitted to the floor (CRP difference 13.6, p=0.01; Ferritin difference 1071.7; p=0.01, CK difference 561, p=0.03). •Patients who had to be placed on mechanical ventilation had significantly higher CRP and ferritin levels at admission (CRP difference 21.5, p=0.04; ferritin difference 958.7, p=0.03); patients on mechanical ventilation also had increased peak levels of all markers (CRP difference 13.6, p=0.01, ferritin difference 1071.7, p=0.01; d-dimer difference 5.1, p=0.05; CK difference 626.3, p=0.02). •Patients who died while in patient had higher d-dimer levels at admission (d-dimer difference 7.4, p=0.001); there was a trend in significance in the difference between peak CRP and ferritin levels among patients who died while inpatient.
Discussion
So while clinical features such as hypoxia are often indicators for increased surveillance (ICU admission) and mechanical intubation, elevated markers such as CRP, ferritin, d-dimer and CK are also associated with ICU admission and mechanical ventilation. Elevation in inflammatory markers such as CRP and ferritin have been demonstrated among severe casesof COVID-19 previously (Zeng, 2020). Surprisingly, different levels of inflammatory markers were not different among those presenting with and without hypoxia. Thus, inflammatory markers could be early warning signs for whether a COVID 19+ patient should be admitted, monitored at home, or triaged further. Similar to other studies, we found increasing levels of d-dimer was associated with mortality in COVID 19 patients.3 Limitations to this study include small sample size, differences in practices of collecting laboratory samples over time (more samples were collected in ICU patients in comparison to floor patients). These markers were collected for exploratory analysis, not for decision making in the majority of cases, thus there was no uniform protocol for collectingmarkers. Overall, tracking markers may be useful in determining the severity of COVID-19 infection and ascertaining disposition. The effect of dexamethasone on inflammatory markers remains to be determined, as our cases are frombefore the RECOVERY trial. Next steps in furthering this research include: •Ascertain levels at which patients are more likely to be admitted to ICU or require mechanical ventilation (could also match markers with P:F ratios). •Determine if there is a certain level at which steroids may be of benefit. •Determine if these markers may be used to track duration of therapy and when therapy can be stopped.
-

When Two Isn’t Better Than One: A Case of Severe Hyponatremia from Combination Thiazide Diuretic and ARB Therapy
Jillian Catral and Emily Hitchcock
Introduction
Thiazide diuretics and angiotensin II receptor blockers (ARB) are common medications for hypertension and are widely used together to counteract thiazide-induced hypokalemia •Thiazide-associated hyponatremia (TAH) is fairly common. There are also multiple case series in the literature of severe hyponatremia in elderly pts attributed to initiation of a thiazide-ARB combination, even when the thiazide dose was low. This is a unique case of hyponatremia in which ARB on thiazide therapy seems to have precipitated severe hyponatremia.
Case Report This is a 74-year-old female with a history of essential hypertension with intolerance to several antihypertensive medications, post-operative hyponatremia after laminectomy for cervical stenosis, mild peripheral edema, and chronic intermittent cough, who was being followed in clinic for refractory hypertension
Discussion
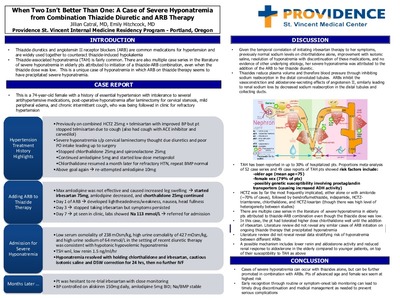
Given the temporal correlation of initiating irbesartantherapy to her symptoms, previously normal sodium levels on chlorthalidonealone, improvement with isotonic saline, resolution of hyponatremia with discontinuation of these medications, and no evidence of other underlying etiology, her severe hyponatremia was attributed to the addition of the ARB to her thiazide diuretic. •Thiazides reduce plasma volume and therefore blood pressure through inhibiting sodium reabsorption in the distal convoluted tubules. ARBs inhibit the vasoconstriction and aldosterone-secreting effects of angiotensin II, similarly leading to renal sodium loss by decreased sodium reabsorption in the distal tubules and collecting ducts.
TAH has been reported in up to 30% of hospitalized pts. Proportions meta-analysis of 52 case series and 49 case reports of TAH pts showed risk factors include: -older age (mean age=75) -female sex (79% of pts) -possibly genetic susceptibility involving prostaglandin transporters (causing increased ADH activity) •HCTZ was by far the most frequently implicated, either alone or with amiloride(~70% of cases), followed by bendroflumethiazide, indapamide, HCTZ-triamterene, chlorthalidone, and HCTZ-losartan (though there was high level of heterogeneity between studies) •There are multiple case series in the literature of severe hyponatremia in elderly pts attributed to thiazide-ARB combination even though the thiazide dose was low. •In this case, the pthad tolerated higher dose chlorthalidonewell until the addition of irbesartan. Literature review did not reveal any similar cases of ARB initiation on ongoing thiazide therapy that precipitated hyponatremia •Literature review did not reveal revealdata stratifying risk of hyponatremia between different ARBs •A possible mechanism includes lower renin and aldosterone activity and reduced renal response to aldosterone in the elderly compared to younger patients, on top of their susceptibility to TAH as above
Conclusion
Cases of severe hyponatremia can occur with thiazides alone, but can be further promoted in combination with ARBs. Pts of advanced age and female sex seem at highest risk •Early recognition through routine or symptom-onset lab monitoring can lead to timely drug discontinuation and medical management as needed to prevent serious complications
-

A case of succinylcholine-induced postoperative myalgia
Nancy Ha and Stephanie Griffith
Introduction
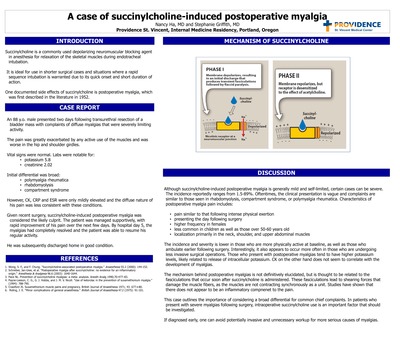
Succinylcholine is a commonly used depolarizing neuromuscular blocking agent in anesthesia for relaxation of the skeletal muscles during endotracheal intubation. It is ideal for use in shorter surgical cases and situations where a rapid sequence intubation is warranted due to its quick onset and short duration of action. One documented side effects of succinylcholine is postoperative myalgia, which was first described in the literature in 1952.
Case Report
An 88 y.o. male presented two days following transurethral resection of a bladder mass with complaints of diffuse myalgias that were severely limiting activity. The pain was greatly exacerbated by any active use of the muscles and was worse in the hip and shoulder girdles. Vital signs were normal. Labs were notable for: •potassium 5.8 •creatinine 2.02 Initial differential was broad: •polymyalgia rheumatica •rhabdomyolysis •compartment syndrome However, CK, CRP and ESR were only mildly elevated and the diffuse nature of his pain was less consistent with these conditions. Given recent surgery, succinylcholine-induced postoperative myalgia was considered the likely culprit. The patient was managed supportively, with rapid improvement of his pain over the next few days. By hospital day 5, the myalgias had completely resolved and the patient was able to resume his regular activity. He was subsequently discharged home in good condition.
Discussion
Although succinylcholine-induced postoperative myalgia is generally mild and self-limited, certain cases can be severe. The incidence reportedly ranges from 1.5-89%. Oftentimes, the clinical presentation is vague and complaints are similar to those seen in rhabdomyolysis, compartment syndrome, or polymyalgia rheumatica. Characteristics of postoperative myalgia pain includes: •pain similar to that following intense physical exertion •presenting the day following surgery •higher frequency in females •less common in children as well as those over 50-60 years old •localization primarily in the neck, shoulder, and upper abdominal muscles The incidence and severity is lower in those who are more physically active at baseline, as well as those who ambulate earlier following surgery. Interestingly, it also appears to occur more often in those who are undergoing less invasive surgical operations. Those who present with postoperative myalgias tend to have higher potassium levels, likely related to release of intracellular potassium. CK on the other hand does not seem to correlate with the development of myalgias. The mechanism behind postoperative myalgias is not definitively elucidated, but is thought to be related to the fasciculations that occur soon after succinylcholine is administered. These fasciculations lead to shearing forces that damage the muscle fibers, as the muscles are not contracting synchronously as a unit. Studies have shown that there does not appear to be an inflammatory compnenet to the pain. This case outlines the importance of considering a broad differential for common chief complaints. In patients who present with severe myalgias following surgery, intraoperative succinylcholine use is an important factor that should be investigated. If diagnosed early, one can avoid potentially invasive and unnecessary workup for more serious causes of myalgias.
-

When your patient DOES know best: A lesson in geriatrics
Daphne Sy and Jeff Youker
Introduction
An athletic elderly woman presented to the emergency department (ED) with subjective leg weakness, most notably while climbing stairs. The patient’s insistence that we acknowledge her change in functional status prompted a workup that exposed an active pauci-immune crescentic glomerulonephritis. She was diagnosed with an unusual presentation of granulomatosis with polyangiitis (GPA) which was discovered in time to initiate treatment and prevent renal failure.
Case Report
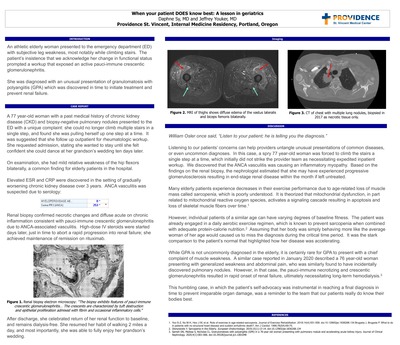
A 77 year-old woman with a past medical history of chronic kidney disease (CKD) and biopsy-negative pulmonary nodules presented to the ED with a unique complaint: she could no longer climb multiple stairs in a single step, and found she was pulling herself up one step at a time. It was suggested that she follow up outpatient for rheumatologic workup. She requested admission, stating she wanted to stay until she felt confident she could dance at her grandson’s wedding ten days later. On examination, she had mild relative weakness of the hip flexors bilaterally, a common finding for elderly patients in the hospital. Elevated ESR and CRP were discovered in the setting of gradually worsening chronic kidney disease over 3 years. ANCA vasculitis was suspected due to serology: Renal biopsy confirmed necrotic changes and diffuse acute on chronic inflammation consistent with pauci-immune crescentic glomerulonephritis due to ANCA-associated vasculitis. High-dose IV steroids were started days later, just in time to abort a rapid progression into renal failure; she achieved maintenance of remission on rituximab. After discharge, she celebrated return of her renal function to baseline, and remains dialysis-free. She resumed her habit of walking 2 miles a day, and most importantly, she was able to fully enjoy her grandson’s wedding.
Discussion
William Osler once said, “Listen to your patient; he is telling you the diagnosis.” Listening to our patients’ concerns can help providers untangle unusual presentations of common diseases, or even uncommon diagnoses. In this case, a spry 77 year-old woman was forced to climb the stairs a single step at a time, which initially did not strike the provider team as necessitating expedited inpatient workup. We discovered that the ANCA vasculitis was causing an inflammatory myopathy. Based on the findings on the renal biopsy, the nephrologist estimated that she may have experienced progressive glomerulosclerosis resulting in end-stage renal disease within the month if left untreated. Many elderly patients experience decreases in their exercise performance due to age-related loss ofmuscle mass called sarcopenia, which is poorly understood. It is theorized that mitochondrial dysfunction, in part related to mitochondrial reactive oxygen species, activates a signaling cascade resulting in apoptosis and loss of skeletal muscle fibers over time.1 However, individual patients of a similar age can have varying degrees of baseline fitness. The patient was already engaged in a daily aerobic exercise regimen, which is known to prevent sarcopenia when combined with adequate protein-calorie nutrition.2Assuming that her body was simply behaving more like the average woman of her age would caused us to miss the diagnosis during the critical time period. It was the stark comparison to the patient’s normal that highlighted how her disease was accelerating. While GPA is not uncommonly diagnosed in the elderly, it is certainly rare for GPA to present with a chief complaint of muscle weakness. A similar case reported in January 2020 described a 76 year-old woman presenting with generalized weakness and abdominal pain, who was similarly found to have incidentally discovered pulmonary nodules. However, in that case, the pauci-immune necrotizing and crescentic glomerulonephritis resulted in rapid onset of renal failure, ultimately necessitating long-term hemodialysis.3 This humbling case, in which the patient’s self-advocacy was instrumental in reaching a final diagnosis in time to prevent irreparable organ damage, was a reminder to the team that our patients really do know their bodies best.
Providence St. Vincent Internal Medicine Residency in Portland, Oregon, stands out for its superior internal medicine training, allowing our graduates to excel in outpatient, inpatient and/or subspecialty settings. This is a collaborative, supportive and academically rigorous environment with physicians committed to patient-focused compassionate care. Our curriculum and philosophy strive to create leaders with the tools to improve the lives of their patients, as well as shaping the healthcare system of the future, their practice and their communities.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}