
Providence Pharmacy PGY1 Program at Providence Milwaukie and Providence Newberg Medical Centers 2020
The Newberg/Milwaukie PGY1 Pharmacy Residency Program is dedicated to providing the resident with the knowledge, skills and confidence needed to pursue a pharmacy career focused on optimal drug therapy outcomes.
-

Evaluation of Transitional Care Interventions from a Decentralized Clinical Pharmacist in a Small Inpatient Geriatric Psychiatry Unit
Nathan Wong and Michael Brown
Evaluation of Transitional Care Interventions from a Decentralized Clinical Pharmacist in a Small Inpatient Geriatric Psychiatry Unit
Nathan Wong, PharmD; Michael Brown, RPh, BCPS, BCPP
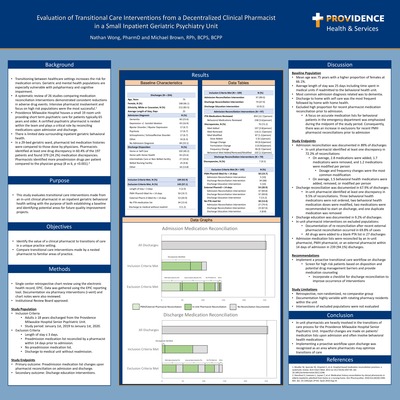
Background: Transitioning between healthcare settings increases the risk for medication errors. A systematic review of 26 studies comparing various medication reconciliation interventions demonstrated consistent reductions in adverse drug events. Intensive pharmacist involvement and focus on high risk populations were the most successful. 1 Geriatric and behavioral health populations are especially vulnerable with polypharmacy and cognitive impairment often complicating the picture. Providence Milwaukie Hospital (PMH) houses a small unit tailored to provide mental health care for seniors. A certified psychiatric pharmacist is nested within the team and plays a critical role in transitional care by reconciling medications upon admission and discharge. This study quantifies these interventions with the purpose of both establishing a baseline and identifying potential areas for future quality improvement projects.
Methods: This is a single center retrospective chart review of all patients discharged from the Providence Milwaukie Hospital Senior Psychiatric Unit from January 1st, 2019 to January 1st, 2020. The unit contains 19 private rooms for patients typically 65 years and older. Short term psychiatric care is provided by a diverse set of mental health professionals. The primary outcome evaluates in-unit changes made upon pharmacist reconciliation of admission and discharge medication lists. The secondary outcome evaluates the occurrence of pharmacist medication counseling upon discharge. Patients with no existing prior to admission medication list or whose list was recently reconciled by a pharmacist prior to admission were excluded. This study has been approved by the Institutional Review Board.
Results: A total of 254 discharges occurred from January 1st, 2019 to January 1st, 2020. Baseline characteristics included an average age of 75 years with a higher proportion of females at 66.1%. The average length of stay was 25 days and the most frequent discharge disposition was to home or self-care. Admission medication lists were reconciled either by a PMH pharmacist or an external pharmacist within 14 days of admission in 239 (94.1%) discharges. Inclusion criteria was met in 109 (42.9%) discharges. In unit pharmacist medication reconciliation on admission totaled to 97 (89.0%). On admission, at least one discrepancy was identified upon 70 (72.2%) reconciliations. A pharmacist on average added 2.8 drugs, removed 1.7 drugs, and modified 1.2 drugs per reconciliation. Of the drugs that were modified, dosing and frequency changes were the most common. Each admission reconciliation included on average an addition, removal, or modification of 1.5 behavioral health medications. Upon discharge, reconciliation was documented in 74 (67.9%) cases and education was documented in 10 (9.2%). Implementing a proactive education and reconciliation workflow upon discharge was recognized as an area where pharmacists may improve the effectiveness of transitions of care.
Conclusions: Pharmacists are heavily involved in the transitions of care process for the Providence Milwaukie Hospital Senior Psychiatric Unit. An embedded clinical pharmacist is making impactful changes to patients’ medication lists upon admission which often involve a behavioral health drug. Ensuring accurate medication lists enables providers to make informed decisions and reduces adverse events.
1. Mueller SK, Sponsler KC, Kripalani S, et al. Hospital-based medication reconciliation practices: a systematic review. Arch Intern Med. 2012 Jul 23;172(14):1057-69. doi: 10.1001/archinternmed.2012.2246.
-

Incorporating a clinical pharmacist in an outpatient palliative care team
Crystal Rim, Sharon Leigh, Linda DeSitter, Mary Grant, and Dana Nguyen
Title: Incorporating a clinical pharmacist in an outpatient palliative care team
Crystal Rim, PharmD; Sharon Leigh, PharmD, BCPS; Linda De Sitter MD, MPH; Mary Grant, ANP; Dana Nguyen, PharmD
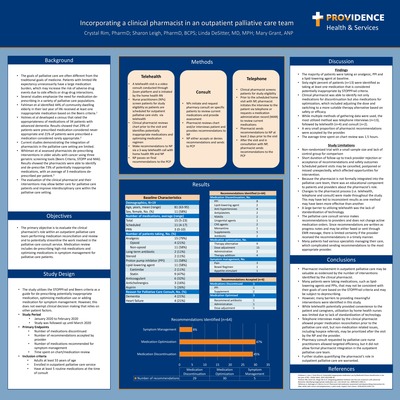
Palliative care is a growing field in medicine that focuses on delivering care that improves quality of life for patients with serious illnesses. Often, the goals of palliative care differ from traditional goals of medicine. Currently, there is limited data demonstrating the integration of pharmacists in the palliative care setting. The purpose of this quality improvement is to evaluate the clinical pharmacist’s role within an outpatient palliative care team when performing medication reconciliation and review. Medication review includes de-prescribing high-risk medications and optimizing medications in symptom management. Between January and February 2020, the clinical pharmacist interviewed patients referred to the outpatient palliative care service through three different methods: telehealth, pharmacy consult and telephone. The clinical pharmacist provided recommendations to the outpatient palliative care nurse practitioner and primary care provider for medication optimization, symptom management and de-prescribing based on STOPPFrail and Beers Criteria. Data from 19 patients were analyzed. One patient was excluded from analysis due to death. Five patients were interviewed through telehealth. Two patients were directly consulted for pharmacist review by the outpatient palliative care nurse practitioner. Seven patients were interviewed through telephone, of which 4 patients were referred to hospice following palliative care consult. Of 19 patients, 64 total recommendations (29 medication discontinuation, 30 medication optimization, 5 symptom management) were made. Six recommendations were accepted by the provider (3 medication discontinuation, 3 medication optimization). The average time spent on chart review for each patient was 1.5 hours. Pharmacist involvement in outpatient palliative care may be valuable. However, many barriers to providing meaningful interventions were identified in this study. While telehealth provided the convenience to the patient and caregivers, utilization was limited due to lack of standardization of technology. Telephone interviews allowed proper medication reconciliation prior to the palliative care visit, but non-medication related issues may be prioritized after the visit. Finally, pharmacy consult from palliative care nurse practitioners allowed more efficiency, but it did not allow formal pharmacist integration in the outpatient palliative care team. Further studies quantifying the pharmacist role in outpatient palliative care are warranted.




{kind=link}
{kind=link}