
-

A Case Of Gluten-Induced Delirium: Using Capsule Endoscopy To Diagnose Occult GI Bleeding
Rachael Starcher and Lisa Sanders
A Case Of Gluten-Induced Delirium:
Using Capsule Endoscopy To Diagnose Occult GI Bleeding
Rachael Starcher, MD
Providence Portland Medical Center – Portland, OR
Additional Authors: Lisa Sanders, MD
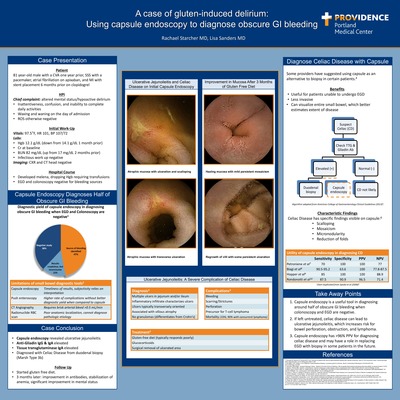
Introduction: Despite an increasing prevalence of celiac disease worldwide, many patients remain undiagnosed, putting them at risk for late stage complications of unidentified and untreated celiac disease. Ulcerative jejunoileitis is a rare cause of occult GI bleeding seen only in refractory celiac disease or in atypical celiac disease at the time of diagnosis. When left untreated, ulcerative jejunoileitis can lead to bowel perforation, blood loss anemia, and T-cell lymphoma.
Case Presentation: An 81-year-old male presented with hypoactive delirium of a few hours duration. His partner noticed inattentiveness, confusion, and inability to complete his daily activities the day of admission. Review of systems was otherwise negative. He had a previous stroke a year prior, sick sinus syndrome with a pacemaker, and myocardial infarction with stent placement just over 6 months before admission. On admission, he was tachycardic to 101, with normal blood pressure and mild anemia (hemoglobin 12.1 g/dL, from 14.1 g/dL a month prior). Infectious work up including viral panel, white count, procalcitonin, and urinalysis was negative. Creatinine was near the patient’s baseline (1.2 mg/dL), but BUN was up to 82 mg/dL from 17 mg/dL a month prior. Head CT was negative for any new process. Initial work up revealed positive fecal occult blood, but subsequent evaluation with upper endoscopy and colonoscopy found no cause. Hemoglobin trended downward and the patient received blood transfusions. Small bowel capsule endoscopy, however, showed evidence of ulcerative jejunoileitis, with subsequent duodenal pathology significant for gluten sensitive enteropathy (celiac disease), Marsh type 3 (destructive type). Serum studies showed elevated tissue transglutaminase IgA, anti-gliadin antibody IgG and IgA. He was started on a gluten free diet and has shown improvement in antibodies, stabilization of anemia, and significant improvement in mental status. Repeat capsule endoscopy has also shown improvement in jejunal ulceration.
Discussion: Capsule endoscopy is an excellent diagnostic tool when the source of a GI bleed cannot be found with EGD or colonoscopy. Not only does it have greater than 96% positive predictive value for diagnosing celiac disease, it can also identify other small bowel disorders including Crohn’s disease. This case highlights the importance of diagnosing celiac disease as when left untreated, complications such as ulcerative jejunoileitis can lead to bowel perforation, blood loss anemia, and T-cell lymphoma; however it can be effectively treated with a gluten free diet.
-

A Case Of Multifactorial Orthostatic Hypotension Complicated By Chemotherapy Associated Autonomic Toxicity
Christopher Bender and Amy Dechet
A Case Of Multifactorial Orthostatic Hypotension Complicated By Chemotherapy Associated Autonomic Toxicity
Christopher Bender, MD
Providence Portland Medical Center – Portland, OR
Additional Authors: Amy Dechet, MD
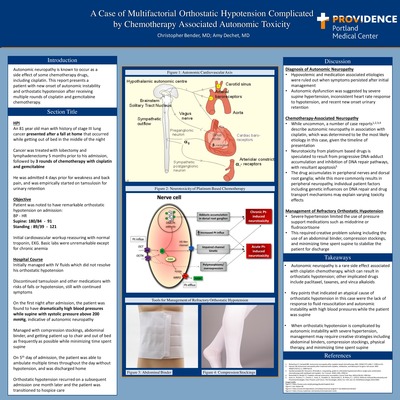
Introduction: Autonomic neuropathy is known to occur as a side effect of some chemotherapy drugs, including cisplatin. This reports presents a patient with new onset of autonomic instability and orthostatic hypotension after receiving multiple rounds of cisplatin and gemcitabine chemotherapy.
Case Presentation: An 81-year-old man with history of stage III lung cancer presented after a fall at home that occurred while getting out of bed in the middle of the night in the setting of recent malaise and poor oral fluid intake. His cancer was treated with surgical lobectomy and thoracic lymphadenectomy five months prior to his admission, and three rounds of chemotherapy with cisplatin and gemcitiabine. He had been admitted to the same hospital three days prior for weakness and back pain and was empirically started on tamsulosin for urinary retention and was discharged with a foley catheter in place.
On presentation he was noted to have marked orthostatic hypotension, and during the first night of admission he had high blood pressures while sleeping, with systolic blood pressure greater than two hundred mmHg. Postural hypotension did not improve over the first twenty-four hours after multiple intravenous fluid boluses. He was managed by discontinuing exacerbating medications including tamsulosin and benadryl, as well as treatment with physical therapy, an abdominal binder, and minimizing the amount of time spent supine. He was discharged on the fifth day of hospitalization after clearance by physical therapy.
Discussion: Although this case initially appeared to be a straightforward case of orthostatic hypotension related to hypovolemia, it became more complicated when the patient continued to display orthostatic hypotension after initial fluid resuscitation and discontinuation of associated medications. Further suggesting autonomic dysfunction was an inconsistent response of heart rate in relation to hypotension, as well as markedly elevated systolic blood pressure readings at night while the patient was supine. While not a common side effect, there are prior documented cases of autonomic neuropathy in association with cisplatin, which was determined to be the most likely etiology in this case, given the timeline of presentation. An additional factor complicating this case was the issue of addressing orthostatic hypotension in a patient with autonomic instability causing intermittent severe hypertension such that the use of midodrine was not an option. This required creative problem solving including the use of an abdominal binder and compression stockings in order to get the patient stable for discharge from the hospital.
-

A Case Of Spontaneous Intercostal Artery Hemorrhage
Chang Min Lee, Veronica Schims, and Craig Riley
A Case Of Spontaneous Intercostal Artery Hemorrhage
Chang Lee, MD
Providence Portland Medical Center – Portland, OR
Additional Authors: Veronica Schims, MD; Craig Riley, MD
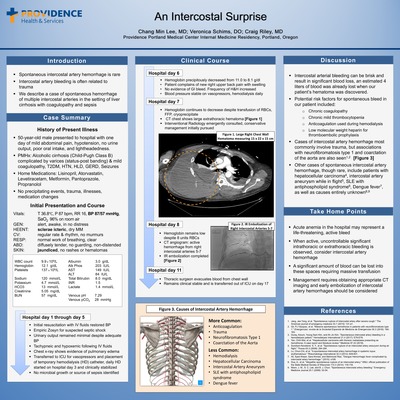
Introduction: Spontaneous intercostal arterial bleeding is rare and usually related to trauma. We describe a patient with a history of cirrhosis and coagulopathy admitted with sepsis who spontaneously developed an expanding extrathoracic hematoma and subsequent hypovolemic shock requiring arterial embolization.
Case Presentation: 50-year-old male with a past medical history of alcoholic liver disease, esophageal varices, chronic coagulopathy, type 2 diabetes and hypertension on lisinopril was admitted to hospital with decreased urine output, dizziness, poor PO intake and lower abdominal discomfort. On exam, blood pressure was 80/50 mmHg and he was encephalopathic with otherwise unremarkable physical exam. Labs showed a normal lactate, sodium 117, hemoglobin 11 g/dL, INR 1.5, elevated creatinine and severe metabolic acidosis. CT abdomen and pelvis showed nonspecific diffuse colitis but no source of infection. His decompensated cirrhosis and acute kidney injury was thought due to poor oral intake and Lisinopril use. He developed worsening renal function and acidosis. His urinary output diminished leading to volume overload. He was then transferred to the intensive care unit for placement of right-sided internal jugular temporary dialysis catheter for initiation of hemodialysis, which was without complications. On hospital day five, he developed a precipitous drop in hemoglobin from 8.7 to 6.0 g/dL and a new right back pain with swelling. A CT chest/abdomen/pelvis revealed a large hematoma along the posterior right hemithorax involving the latissimus dorsi extending from the level of the 1st to 10th rib measuring 30 cm x 5 cm. No reports of trauma and no invasive procedures occurred to explain the hematoma. The patient required multiple transfusions of red blood cells, platelets and fresh frozen plasma and the bleeding, expected to tamponade itself, continued. He underwent emergent arterial embolization with coiling of three intercostal arteries and then successful ultrasound-guided evacuation of the remaining large extrathoracic hematoma.
Discussion: This is a rare case of spontaneous intercostal arterial bleeding. Literature review shows spontaneous intercostal artery hemorrhage is rare. Cases of intercostal artery hemorrhage more commonly involve trauma, and rarer still, associations with neurofibromatosis type 1 and coarctation of the aorta. There is one case report of an incident occurring after hemodialysis, which is the case in this patient. Other case reports include patients with hepatocellular carcinoma, intercostal artery aneurysm while in flight, SLE with antiphospholipid syndrome, Dengue fever, as well as causes entirely unknown. Our patient had underlying liver disease with chronic coagulopathy and mild thrombocytopenia as risk factors for spontaneous bleeding, other considerations included use of low molecular weight heparin or heparin use with hemodialysis, but no inciting factor such as trauma or surgical intervention. When active, uncontrollable bleeding is observed from intercostal arteries, early arterial embolization should be considered.
-

A Perplexing Case Of Episodic Abdominal Pain And The Role Of Mast Cells Gastroenteritis
Hayden Smith and Mari Kai
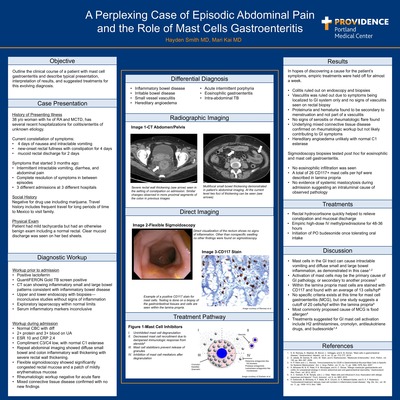
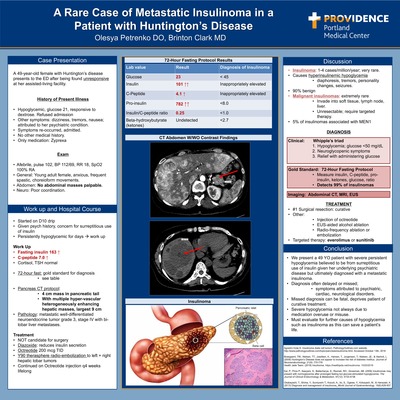
Here we present a case of chronic intractable vomiting and diarrhea of unknown cause, and introduce the relatively new entity of mast cell gastroenteritis.
Our patient is a 38-year old female with PMH of seronegative rheumatoid arthritis, mixed connective tissue disorder, and several recent hospitalizations over the past 4 months at outside hospitals for suspected colitis with associated vomiting and diarrhea. Current symptoms include 4 days of nausea with intractable vomiting, and 2 days of rectal fullness with mucoid rectal discharge. Previous workup at outside hospitals included multiple abdominal CT scans, flexible sigmoidoscopy, colonoscopy, and exploratory laparotomy. Prior to admission no definitive diagnosis were identified for her symptoms, despite extensive workup. Possible causes considered include inflammatory bowel disease, irritable bowel disease, hereditary angioedema, and small vessel vasculitis.
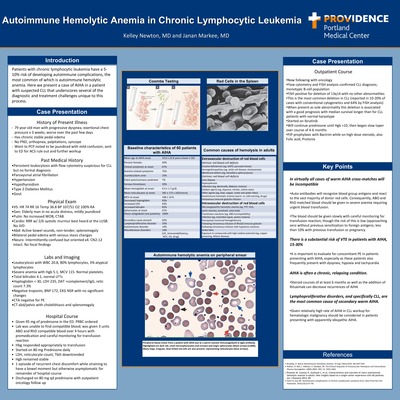
On admission, our physical exam showed no abnormalities including normal rectal exam. CT scan showed inflammation in the colon particularly in the rectum. A flexible sigmoidoscopy showed only edematous appearance of the colon without bleeding, ulcerations, or erythema. Biopsies were obtained, and initial pathology was non-specific. Special stains of the rectal tissue showed increased CD117+ cells at the lamina propria suggesting mast cell gastroenteritis (MCG) as the cause of her symptoms. She was treated with IV steroids until she could tolerate oral budesonide on discharge.
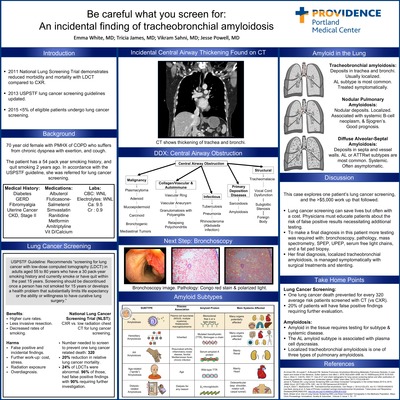
MCG is defined as the abundance of mast cells at the lamina propria along the GI tract. Release of inflammatory mediators by these cells cause gastrointestinal mucosal inflammation leading to symptoms of nausea, vomiting, diarrhea, and abdominal pain. The relatively new and evolving diagnosis of MCG can be part of a larger systemic process or as the patient’s primary problem. Treatments include antihistamines, cromolyn, and steroids. Knowing when to test for MCG and how to interpret the results given a clinical scenario can be helpful in understanding the cause of a patient’s symptoms. In the setting of this case we can better understand this clinical reasoning behind MCG and more effectively treat our patient and her underlying GI mastocytosis.
-

A Rare Case Of Metastatic Insulinoma In A Patient With Huntington’s Disease
Olesya Petrenko and Brinton C. Clark
A Rare Case Of Metastatic Insulinoma
In A Patient With Huntington’s Disease
Olesya Petrenko, DO
Providence Portland Medical Center – Portland, OR
Additional Authors: Brinton Clark, MD, FACP
A 49-year-old female with past medical history of Huntington’s disease presents to the ED after being found unresponsive at her assisted-living facility. She was noted to be hypoglycemic with a glucose of 21 and responded to dextrose. For the past several months, patient had symptoms of dizziness, tremors. She has no history of diabetes, and only home medication is Zyprexa. Patient required D10 drip to maintain glucose levels. Given patient’s psychiatric history, there was concern for surreptitious use of diabetic medications. Labwork showed an insulin level of 163 and an elevated C-peptide of 7.0 consistent with endogenous insulin secretion. Patient underwent a 72-hour fasting protocol which revealed a glucose of 23, C-peptide of 4.1 and insulin of 101, undetectable beta-hydroxybutyrate levels and pro-insulin level of 782 (normal <8), which are consistent with a diagnosis of insulinoma. She was started on diazoxide, which diminishes insulin secretion, to treat the hypoglycemia. Patient underwent a pancreas CT protocol which showed multiple hypervascular hepatic masses up to 9 cm and one 4 cm mass in pancreatic tail concerning for metastasis. Pathology revealed metastatic well-differentiated neuroendocrine tumor grade 3. She was not a candidate for surgical resection of tumors and she was started on Octreotide 200 mcg TID. Patient underwent two Y90 therasphere radioembolization treatments, 2 months apart with improvement of hypoglycemia and discontinuation of diazoxide. Patient remains on Octreotide LAR injection every 4 weeks with frequent glucose monitoring.
Insulinoma, although rare, occurs in 1-4% of the population and is the most common type of functional neuroendocrine tumor of the pancreas. It secretes insulin which results in hyperinsulinemic hypoglycemia. Diagnosis involves persistent hypoglycemia with glucose <50 mg>/dL, neuroglycopenic symptoms and prompt relief after glucose administration. Gold standard diagnosis is a 72-hour fast and measurement of plasma insulin, C-peptide and pro-insulin, which detects 99% of insulinomas. After lab confirmation, imaging is necessary to localize the tumor with either CT, MRI or EUS. Surgical resection is curative in most patients. Other treatment modalities include injection of octreotide, EUS-aided alcohol ablation, radio-frequency ablation or embolization of insulinoma, as well as targeted therapy with everolimus or sunitinib.
Malignant insulinomas are extremely rare and often invade into surrounding soft tissue or have lymph node or liver metastasis. They are usually unresectable and require targeted therapy.
We present the case of a 49-YO patient with Huntington’s disease who presented with severe persistent hypoglycemia secondary to metastatic insulinoma. Diagnosis of insulinoma is often delayed or missed as symptoms may be attributed to psychiatric, cardiac or neurological disorders or medication misuse. Clinicians should be aware of insulinoma as a cause of life-threatening hypoglycemia.
-

Autoimmune Hemolytic Anemia In Chronic Lymphocytic Leukemia
Kelley Newton and Janan Markee
Autoimmune Hemolytic Anemia In Chronic Lymphocytic Leukemia
Kelley Newton, MD
Providence Portland Medical Center – Portland, OR
Additional Authors: Janan Markee, MD
Patients with chronic lymphocytic leukemia have a 5-10% risk of developing autoimmune complications, the most common of which is autoimmune hemolytic anemia. Here we present a case of AIHA in a patient with suspected CLL that underscores several of the diagnostic and treatment challenges unique to this process. A 79-year old man with a history of hypertension, atrial fibrillation, type 2 diabetes and hypothyroidism was undergoing workup for suspected CLL due to a persistent leukocytosis. He then presented to his primary care physician after several weeks of worsening exertional chest pain and dyspnea. On exam, he was noted to be confused as well as mildly jaundiced and was sent to the Emergency Department for work up with a specific concern for ACS given his presenting symptoms. Cardiac workup was unremarkable with a negative troponin, normal BNP and no changes on EKG. Pulmonary CTA was negative for pulmonary embolism. However, his lab work revealed an acute macrocytic anemia with a Hgb of 5.1 as well as a Total bilirubin of 4.1. Additional lab work revealed a significantly decreased haptoglobin, elevated reticulocyte count and IgG/complement positive DAT. CT abd/pelvis showed splenomegaly. The patient was admitted, placed on high dose steroids and 2 units of packed red blood cells were ordered. After some delay due to an inability to find compatible blood, he received several ABO and RhD matched units. After several days, his hemoglobin stabilized and reticulocyte count and Tbili down trended. He was discharged on high dose steroids to be tapered down once his Hgb>10 over the course of 4-6 months, with outpatient oncology follow up. This case highlights several important points in the diagnosis and treatment of AIHA in CLL. Firstly, it is important to note that in virtually all cases of warm AIHA cross-matches will be incompatible as auto-antibodies will recognize blood group antigens and react to the vast majority of donor red cells. Consequently, ABO and RhD matched blood should be given in severe anemia requiring urgent blood transfusion. The blood should be given slowly with careful monitoring for transfusion reaction, though the risk of this is low. Another important consideration in the workup and treatment of AIHA is the substantial risk of VTE in these patients. Given the presentation of dyspnea in this patient, ruling out concomitant PE is especially crucial. Lastly, the relatively high rate of AIHA in CLL workup for hematologic malignancy should be considered in patients presenting with apparently idiopathic AIHA.
-

Be Careful What You Screen For: An Incidental Finding Of Tracheobronchial Amyloidosis
Emma White, Tricia James, Vikram Sahni, and Jesse Powell
Introduction: The 2011 National Lung Screening Trial (NLST) demonstrated a reduction in morbidity and mortality with LDCT compared to CXR. In 2013 the USPSTF began recommending CT scan for lung cancer screening in appropriate patients but, the 2015 National Health Interview Survey (NHIS) demonstrated that less than 5% of eligible patients received screening. The NLST also demonstrated a high rate of false positives, incidental findings, and the need for further invasive testing. When deciding to screen, patients and providers are tasked with reconciling these risks and benefits. In this case, we explore one patient’s incidental findings, and the work-up that ensued.
Our Case: Our patient is a 70-year old female with PMHX of COPD (GOLD 1) who suffers from dyspnea with exertion, and cough. The patient did not tolerate LAMA therapy but her symptoms improved with the addition of an ICS/LABA inhaler. She has had 1-2 COPD exacerbations per year. She has a 54-pack year smoking history and quit smoking 2 years ago. In accordance with USPSTF guidelines and with shared decision making, the patient was referred for lung cancer screening with LDCT. LDCT revealed thickening of the patient’s right and mainstem bronchi, and trachea. In light of this, the patient was referred to pulmonology for bronchoscopy. Bronchoscopy demonstrated irregular thickening and heaped pink mucosa. Biopsies were examined by a pathologist who determined the tissue to be amyloid. Upon follow up in primary care clinic, the tissue samples were located and again sent for amyloid sub-typing which identified AL amyloid. With this finding, the patient required subsequent testing with free light chains, SPEP, and UPEP to rule out a plasma cell dyscrasia. Finally, a fat pad biopsy was ordered to evaluate for systemic amyloidosis. With all of these tests negative, the patient could be diagnosed with localized pulmonary AL amyloidosis & specifically tracheobronchial amyloidosis. This condition is managed symptomatically and does not require systemic chemotherapy.
Discussion: In this case, we explored the diagnosis of a patient with central airway obstruction due to amyloidosis found incidentally during lung cancer screening. In our patient, the incidental finding of central airway obstruction required further testing with bronchoscopy, pathology, mass spectrometry, SPEP, UPEP, serum free light chains, and a fat pad biopsy which were ultimately negative. The high rate of false positive screens and the need for subsequent testing are concerns physicians must address with their patients when recommending lung cancer screening CT. This should be balanced with the potential for reduced mortality and morbidity with CT screening, through higher cure rates, less invasive lung resection, and increased rates of smoking cessation.
-

Beck’s Tetrad? Adding POCUS To The Clinical Exam For Pericardial Tamponade Improves Diagnostic Accuracy In Obstructive Shock
Cody Wiench and Benjamin Pedroja
Beck’s Tetrad?
Adding POCUS To The Clinical Exam For Pericardial Tamponade Improves Diagnostic Accuracy In Obstructive Shock
Cody Wiench, MD
Providence Portland Medical Center – Portland, OR
Additional Authors: Benjamin Pedroja, MD
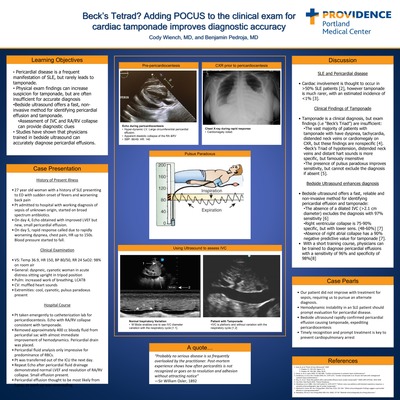
Introduction: Obstructive shock due to tamponade is an important, but rare, cause for sudden cardiovascular collapse. Accurate treatment requires prompt (and correct) diagnosis. Bedside echocardiogram can provide rapid and accurate diagnosis, however the physical exam can provide important clues to consider tamponade. In patients with conditions that predispose them to pericardial disease, such as SLE, one must have a high index of suspicion for tamponade when patients suddenly de-compensate.
Case Presentation: A 27-year old woman with a history of SLE on chronic immunosuppression, pulmonary hypertension and chronic pain presents to the Emergency Department with subjective fevers to 40C, diaphoresis and sudden onset back pain. Vitals in the ED were impressive for heart rate of 106, blood pressure of 92/67, respiration rate of 10. Labs and imaging were unremarkable. Pt admitted to hospital for potential sepsis of unclear cause in an immunosuppressed patient and was started on vancomycin and piperacillin-tazobactam. On day 5 of hospitalization, a rapid response was called due to sudden onset of heart rate to 150, respiration rate to 24, blood pressures of 80s/50s and severe chest pain. Physical exam at that time was notable for muffled heart sounds and pulsus paradoxus. Bedside ultrasound demonstrated a large pericardial effusion resulting in cardiac tamponade. Emergent pericardial fluid drainage was preformed, draining 70 cc of fibrinous, bloody fluid. After procedure, the patient had rapid normalization of hemodynamics. Pericardial fluid analysis was performed, but nonspecific. It is thought that the effusion was secondary to SLE, and the patient was discharged to home in stable condition.
Discussion: Cardiac involvement in SLE is thought to occur in more than 50% of SLE patients, however tamponade is much rarer with an estimated incidence of <1% in a review series. Tamponade portends a poor prognosis in SLE patients. During acute cardiovascular collapse in SLE, one much have a rapid approach to evaluating for tamponade. Pulsus paradoxus is one of those maneuvers; in one prospective study, it was found in 2/3 of patients with tamponade. Unfortunately, patients presenting with the classical “Beck’s Triad” (hypotension, distended neck veins and distant heart sounds) is uncommon; in once study of ultrasound-confirmed tamponade, Beck’s Triad was present in 0% of patients. Fortunately, there are key findings on POCUS exam that, in conjunction with the physical exam, can lead to rapid and accurate diagnosis of tamponade, for instance the absence of a dilated IVC can exclude tamponade with 97% sensitivity.
-

Chronic Hepatitis B Reactivation: Deadly, But Preventable
Sarah Xie, Jesse Powell, and Andrea Roast
Chronic Hepatitis B Reactivation:
Deadly, But Preventable
Sarah Xie, DO
Providence Portland Medical Center – Portland, OR
Additional Authors: Andrea Roast, MD, FACP; Jesse Powell, MD
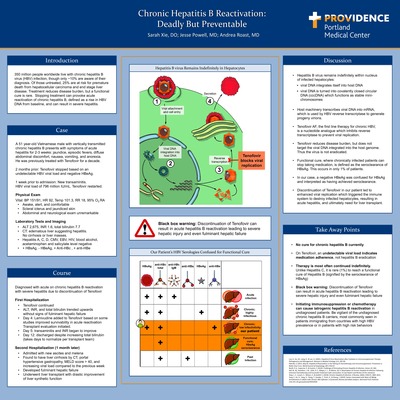
A 51-year-old Vietnamese male with chronic hepatitis B presents with symptoms of acute hepatitis. 2 months prior, his PCP had discontinued Tenofovir, for which he had been taking for the past decade, based on an undetectable viral load and a negative HBeAg. 1 month later, his viral load soared to 796 million so Tenofovir was restarted. On admission a few days later, the patient had scleral icterus and jaundiced skin. He had severe transaminitis, coagulopathy, and a total bilirubin of 7.7. His CT showed hepatitis, but no cirrhosis. With other etiologies ruled out, he was diagnosed with acute on chronic hepatitis B reactivation due to discontinuation of Tenofovir.
He was discharged once his LFTs improved though his total bilirubin continued to rise. The liver transplant team followed the patient post discharge and one month later, he represented with decompensated liver cirrhosis which progressed to fulminant hepatic failure requiring a liver transplant.
An estimated 350 million people in the US live with chronic hepatitis B, though only a third are aware of their diagnosis. Untreated hep B accounts for over 600,000 deaths per year from HCC and end stage liver disease. There is no cure because hep B virus remains in hepatocytes by integrating its DNA into our own and by turning its DNA into stable mini-chromosomes. Tenofovir AF, the 1st line treatment, works only by inhibiting viral replication outside the nucleus, but does not eradicate viral DNA (point). A negative viral load, as seen in our patient, indicates only medication adherence and not a cure. Only 1% of patients achieve “seroclearance of HBsAg,” constituting a functional cure and can discontinue medications at that point, but 99% of patient require indefinite treatment. Our patient did not have labs consistent with a functional cure. Tenofovir has a black box warning that if discontinued, can cause hepatitis B reactivation leading to severe hepatic injury and even fulminant hepatic failure. It took only one month of discontinued Tenofovir to set in motion our patient’s path for a liver transplant. Fortunately, he is doing well now.
The take home points are that, unlike Hepatitis C, 99% of hep B patients require indefinite treatment to minimize the risk of premature death. Physicians should recognize that only seroclearance of HBsAg suggests a functional cure. Undetectable viral loads indicate successful treatment adherence.
Discontinuation of treatment can result in hepatitis B reactivation and even fulminant hepatic failure. From a broader perspective, clinicians need to be vigilant of undiagnosed chronic hepatitis B carriers, especially in patients immigrating from countries with high prevalence or patient with high risk behaviors. These patients are at risk for reactivation with any immunosuppressive therapy such as steroids or cancer therapies.
-
 by Hiromichi Park, Shirin Ferdosian Najafabadi, Lian Wang, and David Gilbert")
Comparative Detection Of Airway MRSA In Patients With Community-Acquired Pneumonia (CAP)
Hiromichi Park, Shirin Ferdosian Najafabadi, Lian Wang, and David Gilbert
Comparative Detection Of Airway MRSA In Patients With Community-Acquired Pneumonia (CAP)
Hiromichi Park, DO
Providence Portland Medical Center
Portland, OR
Additional Authors: Shirin Ferdosian Najafabadi; Lian Wang, PhD; David Gilbert, MD, MACP
Introduction: Vancomycin is often included in the empiric therapy of CAP to ensure activity against MRSA. The current gold standard for detection of MRSA in the airway is a nasal swab PCR. The FilmArray sputum pneumonia panel includes PCR probes for MRSA. This study compares the detection performance of the nasal swab versus the sputum PCR detection of MRSA. Clinically, the absence of airway-detectable MRSA allows cessation of empiric Vancomycin.
Methods: 585 patients with Community Acquired Pneumonia (CAP) were enrolled to compare pathogen detection with a “bundle” of tests versus the new 33 target FilmArray sputum pneumonia panel. Of the 585 patients, 112 patients were evaluable for comparative detection of S. aureus via blood and sputum culture, sputum FilmArray pneumonia panel and nasal swab PCR.
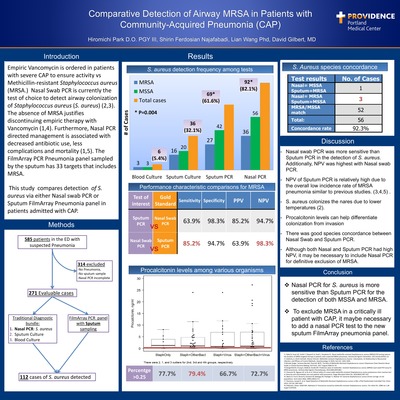
Results: The FilmArray pneumonia panel sampled from sputum detected 69 cases representing 62.2% of total evaluable cases. Nasal swab PCR detected 92 cases representing 82% of total cases. P value was 0.004 between tests. Sputum PCR had a sensitivity rate of 63.9% with a negative predictive value of 94.7% when nasal PCR was considered as the gold standard for MRSA detection. Conversely the nasal PCR had a sensitivity of 85.2% with negative predictive value of 98.3% when sputum PCR is gold standard. Among cases that were simultaneously detected by nasal and sputum PCR, species (MSSA and MRSA) match rate was 52/56 (92.3%).
Discussion: Nasal swab PCR testing had significantly higher sensitivity than sputum PCR in detection of S. aureus (both MSSA and MRSA). Of clinical import, a negative nasal PCR for MRSA supports discontinuation of empiric Vancomycin Therapy. Conversely, the 20% lower frequency of MRSA detection with the sputum PCR creates uncertainty in decisions to discontinue Vancomycin therapy.
Conclusions: Nasal PCR for S. aureus is more sensitive than sputum PCR for both MSSA and MRSA. In a critically ill patient with influenza and elevated serum Procalcitonin level, the most sensitive method to detect the presence of MRSA is a nasal swab PCR.
-

Drugging Chemokine Receptors: Biased CXCR3 Agonists Differentially Regulate Chemotaxis And Inflammation
Jeffrey Smith, Dylan Eiger, Chia-Feng Tsai, Lowell Nicholson, Rachel Glenn, Priya Alagesan, Amanda MacLeod, John Jacobs, Tujin Shi, and Sudarshan Rajagopal
Drugging Chemokine Receptors: Biased CXCR3 Agonists Differentially Regulate Chemotaxis And Inflammation
Jeffrey Smith, MD, PhD
Providence Portland Medical Center – Portland, OR
Additional Authors: Dylan Eiger, BS; Chia-Feng Tsai, PhD; Lowell Nicholson,MD; Rachel Glenn, BS; Priya Alagesan, BS; Amanda MacLeod, MD; John Jacobs, PhD; Tujin Shi, PhD; Sudarshan Rajagopal, MD,PhD
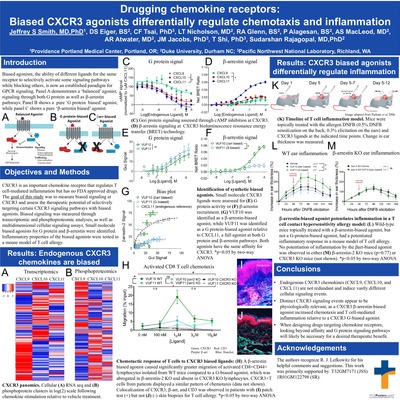
Introduction: G protein-coupled receptors (GPCRs) are the largest class of transmembrane receptors and the target of ~30% of FDA approved drugs. It is now well established that GPCRs can signal through multiple transducers, including classical heterotrimeric G proteins but also GPCR kinases and β-arrestins (1). While these signaling pathways can be activated or blocked by ‘balanced’ agonists or antagonists, they can also be selectively activated in ‘biased’ responses. This new GPCR signaling paradigm of ‘biased signaling’ heralds drugs with increasing efficacy and fewer side effects (2). With over 50 ligands and 20 receptors, biased agonism is prominent within the chemokine system. Here, ligands and receptors bind one another with significant redundancy. For example, the GPCR CXCR3 is expressed on activated T cells and has three established endogenous ligands: CXCL9, CXCL10, and CXCL11 (3,4). Despite its role in inflammation, infectious disease, and cancer (5), no approved drugs target CXCR3. The purpose of my research is to measure biased signaling at CXCR3 and assess the therapeutic potential of selectively targeting certain CXCR3 signaling pathways with biased agonists.
Methods: Utilizing state-of-the-art transcriptomic and phosphoproteomic analyses (6), we show vast differences in CXCR3-regulated intracellular signaling. Responses were compared between vehicle, CXCL9, CXCL10, or CXCL11 treatment assessing >5,000 unique phosphopeptides and >13,000 genes. Biased responses were assessed in both immortalized cell lines and primary human T cells. Utilizing various second messenger reporter systems and bioluminescence resonance energy transfer assays (2,3), we identify an important proximal GPCR signaling pathway, β-arrestin, and demonstrate that CXCL11 acts as a β-arrestin-biased agonist at CXCR3. Furthermore, we screened small molecules to identify a G protein-biased and a β-arrestin-biased small molecule agonist of CXCR3. We then utilized these small molecules to measure physiological readouts of inflammation and chemotaxis in both mice and patients.
Results: Endogenous chemokines of CXCR3 activate divergent intracellular signaling pathways. Using both chemokines and small molecules, we show that β-arrestin pathway signaling through CXCR3 is necessary for full efficacy chemotaxis of activated T cells in both mice and patients (p<0.05). In addition, a β-arrestin-biased small molecule potentiated the cutaneous inflammatory responses in wild-type mice (p<0.05), but not in either β-arrestin KO (p=0.77) or CXCR3 KO (p=0.72) mice, indicating both CXCR3 and β-arrestin dependence in T cell mediated inflammatory responses.
Conclusions: Here we show that CXCL9, CXCL10, and CXCL11 activate distinct CXCR3 intracellular signaling pathways with divergent physiological effects. We clearly demonstrate that the multiple CXCR3 chemokines, CXCL9, CXCL10, and CXCL11, are not redundant in their CXCR3 signaling properties. We show that non-canonical β-arrestin signaling is necessary for certain CXCR3-regulated inflammatory responses and for chemotaxis in both mice and patients. These data strongly suggest that CXCR3 biased agonists have therapeutic promise to treat inflammatory conditions.
References
- Smith, J.S. and Rajagopal, S., 2016. The β-arrestins: multifunctional regulators of G protein-coupled receptors. Journal of Biological Chemistry, 291(17), pp.8969-8977.
- Smith, J.S., Lefkowitz, R.J. and Rajagopal, S., 2018. Biased signaling: from simple switches to allosteric microprocessors. Nature Reviews Drug Discovery, 17(4), p.243.
- Smith, J.S., Alagesan, P., Desai, N.K., Pack, T.F., Wu, J.H., Inoue, A., Freedman, N.J. and Rajagopal, S., 2017. CXC motif chemokine receptor 3 splice variants differentially activate beta-arrestins to regulate downstream signaling pathways. Molecular pharmacology, 92(2), pp.136-150.
- Smith, J.S., Nicholson, L.T., Suwanpradid, J., Glenn, R.A., Knape, N.M., Alagesan, P., Gundry, J.N., Wehrman, T.S., Atwater, A.R., Gunn, M.D. MacLeod, A.S., and Rajagopal, S., 2018. Biased agonists of the chemokine receptor CXCR3 differentially control chemotaxis and inflammation. Sci. Signal., 11(555), p.eaaq1075.
- Chow, M.T., Ozga, A.J., Servis, R.L., Frederick, D.T., Lo, J.A., Fisher, D.E., Freeman, G.J., Boland, G.M. and Luster, A.D., 2019. Intratumoral activity of the CXCR3 chemokine system is required for the efficacy of anti-PD-1 therapy. Immunity.
- Tsai, C.F.*, Smith, J.S.*, Krajewski, K., Zhao, R., Moghieb, A.M., Nicora, C.D., Xiong, X., Moore, R.J., Liu, T., Smith, R.D. and Jacobs, J.M., 2019. TMT labeling facilitates RPLC-MS analysis of hydrophilic phosphopeptides. Analytical chemistry.
-

HIV-Associated Burkitt Lymphoma: More than a starry sky appearance
Rahwa Ghebremichael and Amy Dechet
Introduction: •People with HIV infection are at least 50 times more likely to get lymphoma as compared to the general population. •25-40% of these lymphomas will be Burkitt Lymphoma (BL) – an aggressive B cell malignancy with a high proliferative rate and potentially fatal within months if not diagnosed and treated in a timely manner. •This translates to a 10-20% individual life-time risk of BL for an HIV infected person. •The incidence of BL declined after the introduction of highly active antiretroviral therapy (HAART), but to a lesser extent than other HIV-associated malignancies. •Epidemiologic studies suggest the incidence of BL will increase as the HIV-infected population ages
Case Presentation: A 24 yo woman with known HIV presented with 1 month of intermittent fevers, chills, nausea and diffuse abdominal pain most notable in the epigastric region. Her symptoms acutely worsened in the last week, prompting her visit to the Emergency Department.
Past Medical History: •HIV- diagnosed in 2014. Last on ART Feb-May 2019 while in jail. CD4 count 596 (low at 26%) and HIV RNA viral count 26,400 prior to ART initiation. CD4 count improved to 33% with an undetectable viral load in April. •Chronic hepatitis C •Active IVDU – heroin, methamphetamines •Tobacco dependence
Exam: •Vitals: HR 135, RR 22, Temp 102.8 F, normotensive,SpO2>95% on room air •Profuse sweating, notably uncomfortable •New 2/6 holosystolic heart murmur in LUSB with no radiation •Left lower quadrant and epigastric tenderness, negative Murphy’s sign
Labs on admission: •Hgb 9 (baseline: 11) •Normal complete metabolic panel •HIV RNA viral load 55,800 •CD4 count 596, 32%
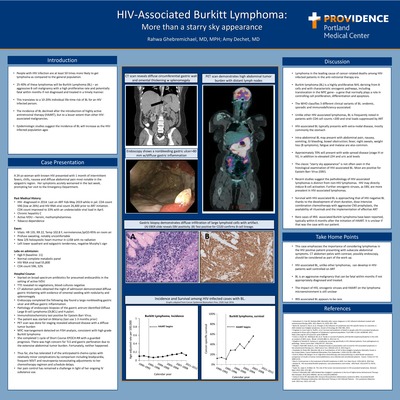
Hospital Course: •Started on broad spectrum antibiotics for presumed endocarditis in the setting of active IVDU •TTE revealed no vegetations, blood cultures negative •CT abdomen pelvis obtained the night of admission demonstrated diffuse gastric thickening with evidence of omental seeding with nodularity and splenomegaly •Endoscopy completed the following day found a large nonbleeding gastric ulcer and diffuse gastric inflammation. •Pathology of endoscopic biopsies of the gastric antrum identified Diffuse Large B-cell Lymphoma (DLBCL) and H.pylori. •Immunohistochemistry test positive for Epstein Barr Virus. •The patient was started on Biktarvy (last use 1-3 months prior) •PET scan was done for staging revealed advanced disease with a diffuse tumor burden •MYC rearrangement detected on FISH analysis, consistent with high grade Burkitt lymphoma •She completed 1 cycle of Short Course EPOCH-RR with a guarded prognosis. There was high concern for TLS and gastric perforation due to the extensive abdominal tumor burden. Fortunately, neither happened. •Thus far, she has tolerated 3 of the anticipated 6 chemo cycles with relatively minor complications by comparison including bradycardia, frequent NSVT and neutropenia necessitating adjustments to her chemotherapy regimen and schedule delays. •Her pain control has remained a challenge in light of her ongoing IV substance use. Discussion: •Lymphoma in the leading cause of cancer-related deaths among HIV-infected patients in the anti-retroviral therapy era. •Burkitt lymphoma (BL) is a highly proliferative NHL deriving from B cells and with characteristic oncogenic pathways, including translocation in the MYC gene-- a gene that normally plays a role in controlling cell proliferation, differentiation and apoptosis. •The WHO classifies 3 different clinical variants of BL: endemic, sporadic and immunodeficiency-associated. •Unlike other HIV-associated lymphomas, BL is frequently noted in patients with CD4 cell counts >200 and viral loads suppressed by ART •HIV-associated BL typically presents with extra-nodal disease, mostly commonly the stomach •Intra-abdominal BL may present with abdominal pain, nausea, vomiting, GI bleeding, bowel obstruction; fever, night sweats, weight loss (B symptoms), fatigue and malaise are also common. •Approximately 70% will present with wide spread disease (stage III or IV), in addition to elevated LDH and uric acid levels •The classic “starry sky appearance” is not often seen in the histological examination of HIV-associated BL. Most are positive for Epstein Barr Virus (EBV). •Recent studies suggest the pathobiology of HIV-associated lymphomas is distinct from non-HIV lymphomas. HIV may directly induce B-cell activation. Further oncogenic viruses, as EBV, are more prevalent in HIV-associated lymphomas. •Survival with HIV-associated BL is approaching that of HIV-negative BL thanks to the development of short duration, dose intensive combination chemotherapy with aggressive CNS prophylaxis, the availability of rituximab and the implementation of effective ART •Rare cases of IRIS- associated Burkitt Lymphoma have been reported, typically within 6 months after the initiation of HAART. It is unclear if that was the case with our patient.
-

Mixed Signals: A Case Of Hypothyroid-Induced Ogilvie’s
Brieanna Brown and Paul Wichienkeur
Mixed Signals:
A Case Of Hypothyroid-Induced Ogilvie’s
Brieanna Brown, MD
Providence Portland Medical Center – Portland, OR
Additional Author: Paul Wichienkeur, MD
Ogilve's syndrome, or acute colonic pseudo-obstruction (ACPO), is characterized by acute dilation of the colon, in the absence of a mechanical lesion, which obstructs the flow of intestinal contents. Pseudo-obstruction typically occurs in the critically ill, though the underlying pathophysiology is poorly understood and the etiology is often multifactorial. We present a case of a 51-year-old morbidly obese woman presenting with symptoms of severe hypothyroidism found to have massive acute colonic pseudo-obstruction.
Case presentation:
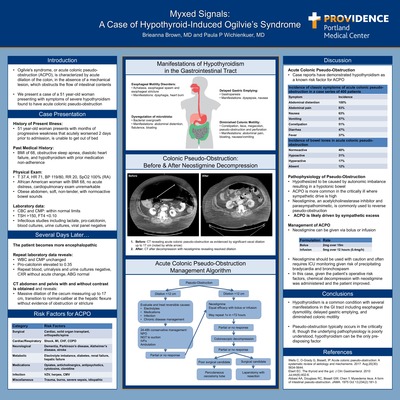
A 51-year-old African-American woman with BMI of 68, OSA, CHF, hypothyroidism and medication non-adherence presented with severe generalized weakness. On admission she was found to have TSH >150 and undetectable free T4. The patient was started on oral replacement therapy but despite this developed acute encephalopathy several days into the admission. She was evaluated for myxedema coma but lacked bradycardia, hypothermia and hyponatremia. Along with encephalopathy, she had poor oral intake and mild nausea, but no vomiting or abdominal pain, and continued having regular bowel movements. CT chest abdomen and pelvis was obtained in the work up of her encephalopathy, which revealed massive dilation of the cecum measuring 17 cm with no obvious mechanical obstruction concerning for pseudo-obstruction. GI and surgical services were consulted, and the patient was ultimately managed non-operatively with neostigmine given her comorbidities. Nasogastric and rectal tubes were placed for decompression and subsequent CT scans revealed decompression without perforation or re-obstruction. The patient was discharged several days later on thyroid replacement with normalization of her T4 and no evidence of re-obstruction.
Discussion:
Acute colonic pseudo-obstruction typically occurs in hospitalized patients in severe illness or after surgery and is hypothesized to be caused by an autonomic imbalance resulting in a hypotonic bowel. This mechanism was originally hypothesized by Ogilvie, who originally suggested lack of sympathetic signaling in the colon1. Sympathetic excess rather than parasympathetic causes are felt to be the more likely etiology, as evidenced by ACPO being more prevalent in the critically ill with high sympathetic drive. Neostigmine, an acetylcholinesterase inhibitor and parasympathomimetic is commonly used to reverse pseudo-obstruction, further suggesting restoration of autonomic balance as a central pathophysiological mechanism. Neostigmine should be used with caution and often requires ICU monitoring given risk of precipitating bradycardia and bronchospasm. Case series of ACPO point to critical illness, surgery, electrolyte imbalance as the most common causes, but hypothyroidism is a rare cause of pseudo-obstruction. Hypothyroidism is a common condition and known to have several manifestations in the GI tract including esophageal dysmotility, delayed gastric emptying, and diminished colonic motility. This case represents the latter, which typically manifests as constipation, but instead presented as a life-threatening pseudo-obstruction which was masked by encephalopathy, body habitus, and lack of prominent abdominal physical examination findings. When conservative management fails, or the cecum exceeds 12cm, typically decompressive colonoscopy or surgery is warranted. In this case, given the patient’s operative risk factors, chemical decompression with neostigmine was administered and the patient improved.
-

Soft Rock – When Blasting It Doesn’t Work
Mark Schneider and Jesse Powell
Soft Rock – When Blasting It Doesn’t Work
Mark Schneider, MD
Providence Portland Medical Center – Portland, OR
Additional Authors: Jesse Powell, MD
Case-History of Present Illness: 68-year-old female presents with several days of malodorous urine and fevers. Brought to the ED by her daughter who diagnosed urinary tract infection (UTI) due to the distinct urine odor. No hematuria, dysuria, retention, or incontinence.
Past Medical History: Recent hospitalization for UTI with culture that grew P.mirabilis, completed course of cefdinir, with follow-up culture ordered by PCP that grew extended-spectrum beta lactamase (ESBL) E.coli.
Physical Exam and Vital Signs: Vitals: 115/48, 101, 38°C, 18, 93% without supplemental oxygen. • Lumbar spine tenderness, no CVA tenderness. Large area of erythema of right inner thigh and chronic lower extremity edema. Otherwise a non-focal exam.
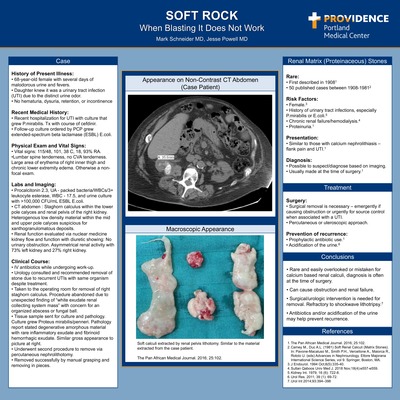
Labs and Imaging: Procalcitonin 2.3, UA - packed bacteria/WBCs/3+ leukocyte esterase, WBC - 17.5, and urine culture with >100,000 CFU/mL ESBL E.coli. CT abdomen : Staghorn calculus within the lower pole calyces and renal pelvis of the right kidney. Heterogenous low density material within the mid and upper pole calyces suspicious for xanthogranulomatous deposits. Renal function evaluated via nuclear medicine kidney flow and function with diuretic showing: No urinary obstruction. Asymmetrical renal activity with 73% left kidney and 27% right kidney.
Clinical Course: IV antibiotics while undergoing work-up. Urology consulted and recommended stone removal due to recurrent UTIs with same organisms despite treatment. Went to OR for stone removal. Procedure abandoned due to unexpected finding of “white exudate renal collecting system mass” with concern for an organized abscess or fungal ball. Tissue sample sent for culture and pathology. Culture grew Proteus mirabilis/penneri. Pathology report stated degenerative amorphous material with rare inflammatory exudate and fibrinoid hemorrhagic exudate. Macroscopic appearance similar to picture at right. Patient readmitted for planned percutaneous nephrolithotomy. The stone was successfully removed by manual grasping and removal in pieces. Renal Matrix (Proteinaceous) Stones.
Rare: First described in 1908. 50 published cases between 1908-1981.
Risk Factors: Female. History of urinary tract infections, chronic renal failure, hemodialysis. • Infection with P.mirabilis or E.coli. Proteinuria.
Presentation: Similar to those with calcium nephrolithiasis – flank pain and UTI.
Diagnosis: Possible to suspect/diagnose by imaging. Usually made at the time of surgery.
Treatment Surgery: Surgical removal is necessary – emergently if obstruction or urgently for source control when associated with a UTI. Percutaneous or uteroscopic approach – Shockwave lithotripsy does not work.
Prevention of recurrence: Prophylactic antibiotic use. Acidification of the urine.
Conclusions • Rare and easily overlooked/mistaken for calcium based renal calculi • Diagnosis often at the time of surgery • Can cause obstruction and renal failure • Surgical/urologic intervention is needed for removal. Refractory to shockwave lithotripsy. • Antibiotics and/or acidification of the urine may help prevent recurrence.
-

The Dangers Of Gardening – Nocardia Infection In An Immunocompromised Patient
Gerald Hutfles and Justin Jin
The Dangers Of Gardening –
Nocardia Infection In An Immunocompromised Patient
Gerald Hutfles, DO
Providence Portland Medical Center – Portland, OR
Additional Authors: Justin Jin, MD
Introduction: Nocardia is a gram-positive, partially-acid fast, aerobic, branching bacillus that can be found in soil and water. It is typically an opportunistic pathogen, with most infections occurring in the immunocompromised. Disease can be localized or disseminated, preferring pulmonary, nervous, and cutaneous tissues. Optimal antimicrobial therapy depends on speciation of the isolate, as Nocardia may exhibit variable antimicrobial susceptibility. A high clinical suspicion and appropriate empiric antimicrobial therapy is necessary. This clinical case highlights the importance of these two factors, as well as the difficulties associated with treatment of disseminated Nocardiosis in the immunocompromised patient.
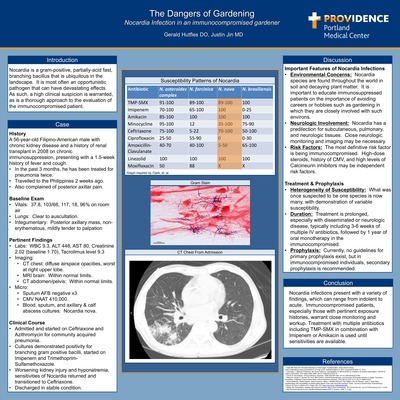
Case Presentation: A 56-year-old Filipino-American male with a history of renal transplant in 2008 due to Membranoproliferative Glomerulonephritis on chronic immunosuppression presented with a three-month history of recurrent cough and chills, worsening in the past week. He had sought medical care twice during this period and had received full courses of Doxycycline and Amoxicillin-Clavulanate with intermittent improvement. He then presented hypoxic, febrile, and tachycardic to the emergency room, with a right upper lobe consolidation and right posterior axillary pain. Respiratory and blood were drawn, as well as Mycobacterium Tuberculosis sputum cultures given recent travel to the Philippines. Patient was then started on Ceftriaxone and Azithromycin for treatment of community-acquired pneumonia. He gradually improved over the next few days, but after several days, blood and sputum cultures were positive for what was found to be Nocardia nova. He also had right axillary and calf abscesses that were subsequently drained and growing Nocardia nova. MRI of his brain, CT of his abdomen, and transthoracic echocardiogram were performed to evaluate the extent of disease, and all were negative. He was transitioned to Imipenem and Trimethoprim-Sulfamethoxazole for treatment of disseminated Nocardiosis. While on therapy, he developed severe hyponatremia, which was thought to be due to current treatment. He was transitioned to Ceftriaxone based on available sensitivities and had improvement of his drug toxicities and symptoms on this regimen. After six weeks of IV antibiotics, he was transitioned to oral Cefpodoxime for an expected twelve months of therapy. Furthermore, nephrology discontinued his Azathioprine to reduce his immunosuppression, and his graft has continued to function well.
Discussion: Nocardia is a ubiquitous organism that uncommonly becomes pathogenic to humans, but infections can be serious, especially in the immunocompromised. It is important to have a high clinical suspicion in immunocompromised patients. As more information emerges about this genus, it is important to fully speciate and obtain antimicrobial sensitivity patterns, which can be quite variable. Duration of treatment in immunocompromised patients and those with CNS infections is at least one year. There are no guidelines for primary prophylaxis for Nocardiosis. Some experts recommend indefinite secondary prophylaxis in patients with ongoing immunosuppression.
-

Vocal Cord Dysfunction Masquerading As Exercise-Induced Bronchoconstriction
Brandon Tempte, Meera Jain, and Jason Wells
Vocal Cord Dysfunction Masquerading As
Exercise-Induced Bronchoconstriction
Brandon Temte, DO
Providence Portland Medical Center – Portland, OR
Additional Authors: Meera Jain, MD, FACP; Jason Wells, MD
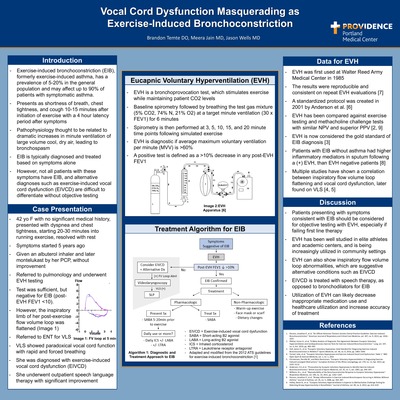
Intro: Exercise-induced bronchoconstriction (EIB), previously exercise-induced asthma, has a high prevalence in the community. Patients with these symptoms are typically diagnosed clinically and treated empirically with pre-exercise albuterol. Eucapnic voluntary hyperventilation (EVH) has been used to objectively test for EIB and can help to confirm the diagnosis, as well as rule out other causes such as exercise-induced vocal cord dysfunction (EIVCD), which may mimic EIB.
Case Description: A 42-year old female with no significant medical history, presented with dyspnea and chest tightness, starting 20-30 minutes into running exercise. Symptoms started five years ago. She was given an albuterol inhaler and later montelukast by her PCP, without improvement. She was referred to pulmonology and underwent EVH testing. Testing was negative for EIB. However, the inspiratory limb of her flow volume loop was flattened on post-exercise spirometry. She was subsequently referred to ENT for videolaryngoscopy (VLS) to rule out EIVCD. VLS showed paradoxical vocal cord function with rapid and forced breathing, and the diagnosis of EIVCD was made. Albuterol and montelukast were discontinued. She underwent outpatient speech language therapy with significant improvement in her symptoms.
Discussion: EIB has a prevalence of 5-20% in the general population and may affect up to 90% of patients with symptomatic asthma. It typically presents as shortness of breath, chest tightness, and cough 10-15 minutes after initiation of exercise. In a community setting, EIB is typically diagnosed and treated based on symptoms alone. However, not all patients with these symptoms have EIB, and may fail expensive inhaler treatments. EVH can help to objectively confirm the diagnosis of EIB and help rule out other potential causes such EIVCD.
EVH requires the patient to breath at a high target minute ventilation to simulate exercise while breathing a set gas mixture to maintain eucapnia. Spirometry is then performed at 3, 5, 10, 15, and 20 minutes to evaluate for a decrease in post-exercise FEV1 >10%, indicating EIB. It is considered by many literature sources to be the “gold standard” of EIB diagnosis when compared to exercise testing and methacholine challenge.
Recent studies utilizing EVH have shown increasing evidence that EIVCD may be a more common cause of exercise-induced symptoms than previously thought. EIVCD can be suggested on EVH by flattening of the inspiratory flow volume loop on post-exercise spirometry. EIVCD can then be confirmed by videolaryngoscopy (VLS). EIVCD is treated with speech language therapy, which is much different from EIB. Utilizing EVH to objectively diagnose EIB can likely lead to a decrease in inappropriate medication use and healthcare utilization with the added benefit of more accurate treatment modalities.
-

When less-virulent becomes virulent!! An atypical presentation of Streptococcus Viridians.
Samreen Khan, Stavan Patel, and Mary Anne Nidiry
When Less Virulent Becomes Virulent!!
An Atypical Presentation Of Streptococcus Viridians
Samreen Kahn, MBBS
Providence Portland Medical Center – Portland, OR
Additional Authors: Stavan Patel MS, MD
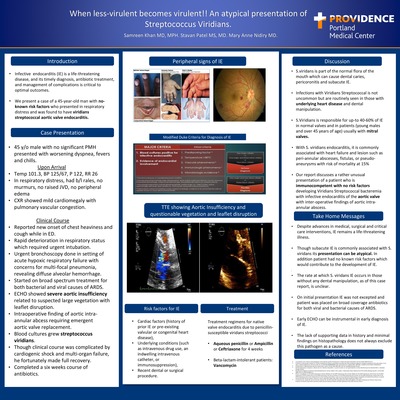
Introduction: There are several cardiac and non-cardiac causes and risk factors for the development of infective endocarditis (IE) in young healthy adults. Some risk factors include prior IE, history of valvular or congenital heart disease, IV drug use, indwelling intravenous lines, immunosuppression, or a recent dental or surgical procedure. Most two common sites of IE are mitral and aortic valve. We present a case of a 45-year-old man with no-known risk factors, who presented with respiratory distress and was found to have streptococcal viridians (SV) endocarditis.
Case Presentation: A healthy 45-year-old male presented with a four-day history of acute dyspnea and new-onset of fevers and chills for 24 hours before arrival. He denied any chest pain, dizziness, palpitations, LOC, weakness, increasing LE edema, or palpations. Patient denied any recent travels, prolonged non-ambulatory state, recent sick contacts, IV drug abuse, high risk sexual activities, no-known personal cardiac history, no recent dental manipulation. While in ED, he reported new onset of chest heaviness, and a non-productive cough. Vitals: T 37.2 C, BP 125/9, P 122, RR 26. EKG showed sinus tachycardia with non- specific ST&T wave abnormalities/No prior ECG where available to compare. Troponin 64 ng/L. ABG pH 7.230, PCO2 27.4 mmHg, PO2 82.1 mmHg. A-a gradient calculated to be greater than 200. CXR showed pulmonary vascular congestion. CTPA for PE was deferred as patient could not remain supine during examination secondary to worsening respiratory status. Patient was moved to medical ICU, with rapid worsening of respiratory status requiring intubation. Urgent bronchoscopy revealed diffuse alveolar hemorrhage consistent with severe acute respiratory distress syndrome (ARDS) with multifocal pneumonia. On initial presentation IE was not excepted and patient was treated for viral and bacterial causes of ARDS. Echocardiogram showed aortic valve insufficiency with questionable vegetation with leaflet disruption. Subsequently blood cultures showed gram-positive cocci. Given the combination of aortic insufficiency (AI) and gram-positive cocci IE speculated which was soon followed by aortic valve replacement with intraoperative finding of aortic intra-annular abscess. Clinical course was complicated with cardiogenic shock and multi-organ failure. Blood cultures subsequently grew SV.
Case Discussion: Despite advances in medical, surgical and critical care interventions, IE remains a life-threatening illness. SV is not uncommon but are routinely seen in those with underlying heart disease and dental manipulation. SV is responsible for 40-60% of IE in normal valves [3, 4] and patients (young males and over 45 years of age) usually with mitral valves. It is commonly associated with heart failure and lesion such as peri-annular abscesses, fistulas, or pseudo-aneurysms with risk of mortality at 15% [1, 2]. Diagnosis may be difficult given no risk factors, non-specific symptoms but does not exclude this pathogen as a cause.
-

Wrap It Up – Sexually Transmitted Primary Cytologmegalovirus Proctitis In Immunocompetent Host: A Case Report
Vanessa Nwaokocha, Brinton Clark, and Ronald Dworkin
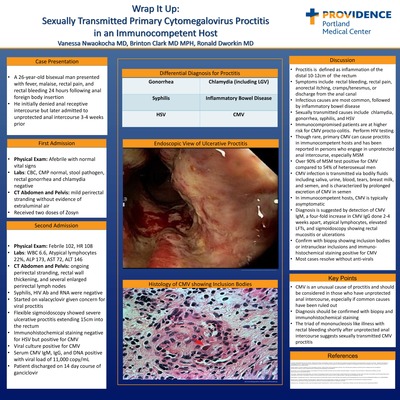
Background: In persons who presents with fever, rectal pain and bleeding, CMV proctitis should be considered if other workup is negative, especially if recent unprotected anal receptive intercourse.
Case Presentation: A 26-year-old bisexual man presented with chief complaints of fever, malaise, rectal pain, and rectal bleeding after anal insertion of foreign body. He initially denied any unprotected sexual intercourse. CBC, CMP, stool pathogen, rectal gonorrhea, and rectal chlamydia were unremarkable. He returned after 1 week with the similar complaints, however admitted to unprotected anal receptive intercourse a month prior. His vitals were notable for temperature of 102 with tachycardia to 108. Labs were significant for WBC 6.6, atypical lymphocytes 22%, ALP 173, AST 72, and ALT 146. CT AP with contrast showed perirectal fat stranding, rectal wall thickening, and several perirectal lymph nodes. Syphilis and HIV testing were negative. Given concern for viral proctitis from HSV, he was treated with valacyclovir. Flexible sigmoidoscopy showed diffuse severe inflammation with deep ulcerations consistent with severe ulcerative proctitis extending 15cm into the rectum. Biopsies were positive for CMV on immunohistochemical staining and viral culture. CMV serology was positive for IgM, IgG, and viral DNA. The patient was treated with ganciclovir for primary CMV proctitis for a 14-day course.
Conclusion: Proctitis typically presents with rectal bleeding, rectal pain, anorectal itching, cramps/tenesmus, or discharge from the anal canal. Common sexually transmitted infectious causes include chlamydia, gonorrhea, syphilis, HSV. CMV has also been shown to be a cause of procto-colitis in immunocompromised patients with HIV. Though rare, primary CMV in an immunocompetent host can cause proctitis and has been reported in persons who engage in unprotected anal intercourse, especially MSM. Diagnosis of primary CMV proctitis requires multiple diagnostic tests in the right clinical setting. Detection of CMV IgM, a four-fold increase in CMV IgG done 2-4 weeks apart, and sigmoidoscopy showing rectal mucositis or ulceration are suggestive of CMV proctitis. In our patient, his atypical lymphocytes and elevated liver function tests were also suggestive of CMV. Biopsy showing presence of inclusion bodies or basophilic intranuclear inclusions and immunohistochemical staining that is positive for CMV are confirmatory. Treatment for primary CMV proctitis has not been well defined and is typically conservative management though we chose to treat with ganciclovir given severity of symptoms. In conclusion, a mononucleosis-like illness with rectal bleeding and/or pain after unprotected anal intercourse can suggest a diagnosis of CMV proctitis.
Providence Portland Internal Medicine Residency in Portland, Oregon, offers academic training in a leading community-based medical center. Our program fosters a learning environment where the intellectual rigor of an academic medical center and the cutting-edge health systems of a top community hospital merge for the betterment of both patient care and education.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}