
Files
Download Full Text (1.3 MB)
Publication Date
4-29-2020
Disciplines
Internal Medicine
Abstract
INTRODUCTION: Catastrophic Antiphospholipid Syndrome (CAPS) is a rare and extreme manifestation of Antiphospholipid Syndrome (APS) that features widespread thrombotic disease affecting multiple small vessels in a short time frame. CAPS affects only 0.8% of APS patients, but when it occurs it is has a mortality rate of approximately 50%.
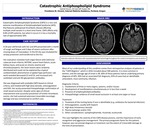
CASE REPORT: A 50 year old female with SLE and APS presented with 1 month of cough and fatigue and 2 days of severe confusion after missing doses of rivaroxaban. In the ED she was intubated for airway protection and transferred to the ICU. Her evaluation revealed multi-organ failure with extensive subacute brain infarcts, NSTEMI, severe heart failure, acute kidney injury, and acute on chronic anemia and thrombocytopenia. Her brain lesions were randomly distributed and could not be explained by a typical cardioemobolic phenomenon or global hypo-perfusion. Lab work revealed decreased C3 and C4, and increased anticardiolipin and anti-B2-glycoprotein antibodies. She was diagnosed with probable CAPS based on clinical criteria, and treated with high dose steroids, anticoagulation and IVIG. Her acuity prevented histopathologic confirmation of small vessel occlusion. Despite some signs of clinical improvement and successful prevention of further thrombotic events, she had sustained extensive irreversible neurologic damage and was transitioned to comfort care.
DISCUSSION: Most of our understanding of this condition comes from retrospective analyses of patients in the “CAPS Registry”, which in 2016 included about 500 patients. It is more common in women, and the average age of onset is 38. 60% of these patients had an underlying primary diagnosis of APS; 30% had an associated SLE diagnosis; 65% of cases had an identifiable antecedent, most commonly, infection. Diagnostic Criteria: 1. Involvement of three or more organs, systems, and/or tissues 2. Development of manifestations simultaneously or in less than a week 3. Presence of antiphospholipid antibodies 4. Histopathologic evidence of small vessel occlusion in at least one organ or tissue Treatment: 1. Treatment of the inciting factor if one is identifiable (e.g. antibiotics for bacterial infection) 2. Anticoagulation, usually with heparin 3. High dose intravenous steroids 4. Plasma exchange and/or IVIG 5. Other considerations: cyclophosphamide, rituximab, eculizumab This case highlights the severity of the CAPS disease process, and the importance of early recognition and aggressive management. The primary prognostic factor for this patient, however, was not prompt diagnosis or treatment, but the extent of irreversible damage at the time of presentation.
Specialty/Research Institute
Internal Medicine
Specialty/Research Institute
Graduate Medical Education
Conference / Event Name
Academic Achievement Day, 2020
Location
Providence St. Vincent, Internal Medicine Residency, Portland, Oregon



