
-

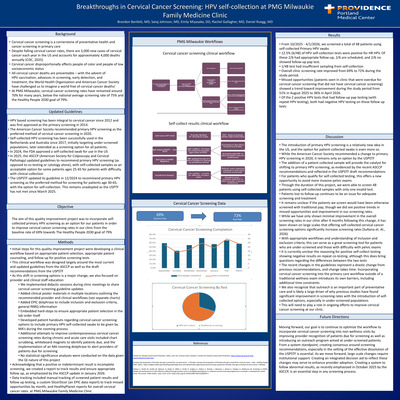
Breakthroughs in Cervical Cancer Screening: HPV self-collection at PMG Milwaukie Family Medicine Clinic
Brandon Bartlett, Sataj Johnson, Emily Miyasako, Rachel Gallagher, and Daniel Ruegg
-

Enhancing Gestational Diabetes Screening
Sataj Johnson and Daniel Ruegg
Background: Gestational diabetes mellitus (GDM) screening is recommended between 24–28 weeks of gestation to allow timely diagnosis and treatment and reduce adverse maternal and neonatal outcomes. The two-step glucose tolerance testing method is supported by ACOG, though completion can be delayed due to the need for multiple tests. In 2024 at Providence Milwaukie Family Medicine Clinic, incomplete GDM screening occurred in 23.1% of patients, and incomplete two-step screening occurred in 33.3%, with an average completion time of 12 days. Objective: To increase completion rates of two-step GDM screening and reduce time between abnormal 1-hour and diagnostic 3-hour glucose tolerance tests by offering clinic-based testing instead of lab-only screening. Methods: Clinic-based screening was implemented by obtaining supplies and establishing a workflow. Outcomes were evaluated through chart review and data collection. Results: Prior to implementation, the two-step screening completion rate was 70%, with an average completion time of 15 days. From March 2025 to February 2026, completion increased to 81%, with 72.7% completed in clinic and 9% in the lab. Non-completion decreased to 18%. Average completion time improved to 11 days. Conclusion: GDM affects approximately 1 in 11 pregnancies in the United States and can lead to significant maternal and neonatal complications if untreated. Clinic-based screening modestly improved completion rates and reduced time to diagnostic testing. Patients reported the clinic option as convenient. Expanding clinic-based screening may improve access, patient satisfaction, and timely diagnosis, particularly in settings with limited laboratory access. Larger studies are needed to assess statistical significance and long-term obstetric and neonatal outcomes.
-

Addressing Food Insecurity through partnering with the Community Teaching Kitchen on Lifestyle Medicine Hypertension Class
Emily Miyasako and Jill Christensen
Background: Food insecurity is defined as limited or unreliable access to adequate and nutritious food. In Oregon, approximately 1 in 8 residents experience food insecurity, with rates disproportionately affecting low-income individuals, racial and ethnic minorities, and households with children or elderly individuals. Food insecurity remains a significant threat to our patients’ health and is associated with obesity, malnutrition, and poor mental health. As a primary care provider, I have seen the effects of food insecurity on my patients, but I am thankful for the presence of our Community Teaching Kitchen. The Community Teaching Kitchen (CTK) at Providence Milwaukie provides nutritional counseling, operates a community garden that provides a sustainable source of fresh produce, and manages a family food pantry providing nutritious foods available to patients experiencing food insecurity. CTK serves a vital role in providing reliable access to healthy foods for individuals in our community. However, after HR 1 was passed in July 2025, SNAP benefits were significantly reduced. This severely impacted CTK’s ability to help support our community due to decreased funding and increased need. Our clinic has been implementing a group hypertension class as part of the lifestyle medicine elective. My passion project involved partnering with the CTK for the lifestyle medicine group hypertension class to help provide revenue for the CTK and the family food pantry, while also introducing our patients to this valuable resource. Goals and objectives: To introduce our patients to the services offered by the Community Teaching Kitchen, as well as to create a sustainable source of revenue for the Community Teaching Kitchen so they can continue to provide nutritious food for our patients with food insecurity. Methods: We adapted the 4-week lifestyle medicine group hypertension course to incorporate services offered by CTK. The classes are scheduled on 3/11, 3/18, 3/25 and 4/1. One of the sessions of the class will be held in the community garden, where we will discuss the importance of exercise and demonstrate a meditation class. The final session will be held at the teaching kitchen, where we will demonstrate how to cook a DASH diet meal by using resources and a recipe provided by the CTK staff. We will measure patient learning and satisfaction with pre and post-course surveys. Results: In order to increase recruitment, I personally reached out to my panel of patients who had uncontrolled hypertension via Mychart messages. We were able to recruit 7 patients (of which 6 attended the first class), thereby meeting our goal of 6-8 participants. We will be able to share the proceeds of the class (each session is billed as a level 3 visit) with our Community Teaching Kitchen, which will be able to fund the family food pantry. We have collected pre-course survey on baseline hypertension knowledge and plan to compare this to post-course survey results to evaluate patient learning. We will also analyze patient satisfaction scores on the post-course survey. Discussion/conclusion: Food insecurity is a highly prevalent yet under-addressed determinant of health among our patients. Our Community Teaching Kitchen has been essential in helping our patients with food insecurity by providing nutritious food and dietary counseling. By partnering with the CTK for our group lifestyle medicine hypertension class, we can introduce our patients to this valuable resource as well as provide a sustainable source of income for our community food pantry to continue to support our patients with food insecurity.
-

Improving Cervical Cancer Screening at PMG Southeast Family Medicine Through Implementing a New Screening Tool: Patient-Collected High-Risk HPV Screening
Brianna Pickering, August Stuppy, Eric Waelbroeck, Ben Pederson, and Daniel Ruegg
-

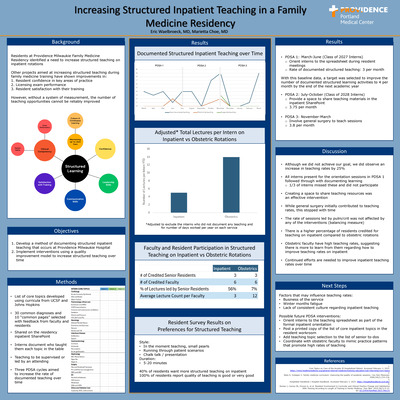
Increasing Structured Inpatient Teaching in a Family Medicine Residency
Eric Waelbroeck and MH Choe
Background: What is not measured cannot be improved. Residents at Providence Milwaukie Family Medicine Residency identified a need to increase structured teaching on inpatient rotations. Other projects aimed at increasing structured teaching during family medicine training have demonstrated improvements in resident confidence in key areas of practice, licensing exam performance, and resident satisfaction with their training. However, without a system of measurement, the number of teaching opportunities cannot be reliably improved. Objectives: Develop a method of documenting structured inpatient teaching that occurs at Providence Milwaukie Hospital. Then, implement interventions using a quality improvement model to increase structured teaching over time. Methods: A list of inpatient topics was developed referencing inpatient curricula from UCSF and Johns Hopkins. This list was narrowed down to 30 common admitting diagnoses and 10 “common pages” using feedback from the residency inpatient committee. A table was shared on the residency inpatient SharePoint where interns could document who taught them each topic. Then, three PDSA cycles each lasting 4 months aimed to increase the rate of documented teaching over time. Results: The baseline rate of intern-documented structured learning activities during inpatient rotations over the final 4 months of the class of 2027 intern year was 3 per month. This includes the first PDSA, where interns were oriented to the spreadsheet during resident meetings. With this baseline data, a target was selected to improve the number of documented structured learning activities to 4 per month by the end of the subsequent academic year. After providing a space to share teaching materials in the SharePoint, the rate of teaching for the first 4 months of the class of 2028 intern year increased to 3.75 per month. After asking general surgery to teach sessions, the rate of teaching for the subsequent 4 months remained stable at 3.8 per month. Discussion/Conclusions/Next Steps: This project was successful in producing a method of documenting structured inpatient teaching that interns receive in a family medicine residency. Quality improvement efforts were successful in generating a ~25% increase in teaching rates, with the most effective intervention being sharing a space for teaching resources. Comparing adjusted teaching rates on inpatient to obstetric rotations demonstrates a continued discrepancy (5.5 vs 14 per month). This highlights the imbalance that residents experience in their education and reaffirms the need for continued efforts at improving structured learning in the inpatient setting. Future efforts could consider posting the list of teaching topics in the resident workroom, adding teaching topic selection to the list of to-dos on the senior inpatient guide, and engaging faculty to improve teaching rates.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}