
Files
Download Full Text (269 KB)
Publication Date
4-29-2026
Keywords
oregon, psvmc, psvmc gme, psvmc oaa, oregon gme
Disciplines
Medical Education | Pharmacy and Pharmaceutical Sciences | Substance Abuse and Addiction
Abstract
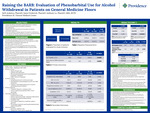
Abstract: Alcohol withdrawal syndrome (AWS) can present as a spectrum of symptoms such as a mild headache, gastrointestinal issues, and diaphoresis. However, if not treated properly, it can progress to severe hallucinations, seizures, or delirium tremens. Current guidelines from the American Society of Addiction Medicine (ASAM) recommend benzodiazepines as first line agents for alcohol withdrawal with phenobarbital recommended as an adjunct agent or replacement to benzodiazepines by providers who are familiar with its use. Although most evidence supporting phenobarbital in AWS comes from critical care settings, emerging data suggest it may also be safe and effective in general ward patients. Providence St. Vincent Medical Center (PSVMC) recently expanded phenobarbital use for AWS to the general ward floors with a dose cap of 20 mg/ kg ideal body weight (IBW), but guidance is lacking for alcohol withdrawal management. The purpose of this study is to evaluate the efficacy, safety, and ordering practices of phenobarbital in comparison to Benzodiazepines for alcohol withdrawal on general medicine floors and whether modifications to the alcohol withdrawal treatment protocol at PSVMC are needed. This will be a single-center, retrospective, observational cohort study evaluating patients admitted outside of the ICU and emergency department settings at PSVMC. Patients will be included if they are greater than 18 years of age, non-ICU patients diagnosed with alcohol withdrawal syndrome and received either phenobarbital or a benzodiazepine for alcohol withdrawal. The primary endpoints for this study will be treatment failure, defined as ICU transfer, and time to resolution, defined as CIWA score < 9 sustained until discharge. Secondary endpoints will include hospital length of stay, medication-related adverse effects (e.g. respiratory depression, neurologic effects), average doses of phenobarbital and benzodiazepines, intubation rates, use of adjunct agents for alcohol withdrawal symptoms, and percent of patients who hit the phenobarbital protocol dose cap of 20 mg/kg IBW. Manual chart review and EPIC Slicer Dicer will be used to identify patients and retrieve data from the electronic health record. Descriptive statistics will be used to describe baseline characteristics of study population, efficacy, and safety for both the benzodiazepines and phenobarbital groups. A chi-square test will be used to evaluate categorical data while a t-test will be used for numerical outcomes. Results and conclusions will be shared when the project is completed. (IRB approved). Learning Objectives: Evaluate the efficacy, safety, and ordering practices of phenobarbital in comparison to benzodiazepines for alcohol withdrawal on the general medicine floors. Presentation Category: Inpatient clinical services
Area of Special Interest
Mental Health
Specialty/Research Institute
Behavioral Health
Specialty/Research Institute
Graduate Medical Education
Specialty/Research Institute
Pharmacy
Included in
Medical Education Commons, Pharmacy and Pharmaceutical Sciences Commons, Substance Abuse and Addiction Commons



