
-

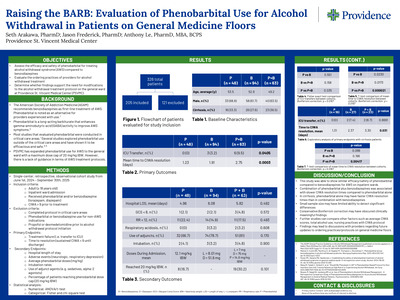
Raising the BARB: Evaluation of Phenobarbital Use for Alcohol Withdrawal in Patients on General Medicine Floors
Seth Arakawa, Jason Frederick, and Anthony Le
Abstract: Alcohol withdrawal syndrome (AWS) can present as a spectrum of symptoms such as a mild headache, gastrointestinal issues, and diaphoresis. However, if not treated properly, it can progress to severe hallucinations, seizures, or delirium tremens. Current guidelines from the American Society of Addiction Medicine (ASAM) recommend benzodiazepines as first line agents for alcohol withdrawal with phenobarbital recommended as an adjunct agent or replacement to benzodiazepines by providers who are familiar with its use. Although most evidence supporting phenobarbital in AWS comes from critical care settings, emerging data suggest it may also be safe and effective in general ward patients. Providence St. Vincent Medical Center (PSVMC) recently expanded phenobarbital use for AWS to the general ward floors with a dose cap of 20 mg/ kg ideal body weight (IBW), but guidance is lacking for alcohol withdrawal management. The purpose of this study is to evaluate the efficacy, safety, and ordering practices of phenobarbital in comparison to Benzodiazepines for alcohol withdrawal on general medicine floors and whether modifications to the alcohol withdrawal treatment protocol at PSVMC are needed. This will be a single-center, retrospective, observational cohort study evaluating patients admitted outside of the ICU and emergency department settings at PSVMC. Patients will be included if they are greater than 18 years of age, non-ICU patients diagnosed with alcohol withdrawal syndrome and received either phenobarbital or a benzodiazepine for alcohol withdrawal. The primary endpoints for this study will be treatment failure, defined as ICU transfer, and time to resolution, defined as CIWA score < 9 sustained until discharge. Secondary endpoints will include hospital length of stay, medication-related adverse effects (e.g. respiratory depression, neurologic effects), average doses of phenobarbital and benzodiazepines, intubation rates, use of adjunct agents for alcohol withdrawal symptoms, and percent of patients who hit the phenobarbital protocol dose cap of 20 mg/kg IBW. Manual chart review and EPIC Slicer Dicer will be used to identify patients and retrieve data from the electronic health record. Descriptive statistics will be used to describe baseline characteristics of study population, efficacy, and safety for both the benzodiazepines and phenobarbital groups. A chi-square test will be used to evaluate categorical data while a t-test will be used for numerical outcomes. Results and conclusions will be shared when the project is completed. (IRB approved). Learning Objectives: Evaluate the efficacy, safety, and ordering practices of phenobarbital in comparison to benzodiazepines for alcohol withdrawal on the general medicine floors. Presentation Category: Inpatient clinical services
-

Spur Cell Anemia: A Crucial Unanticipated Anemia in Critical Care
Jobe Ashby
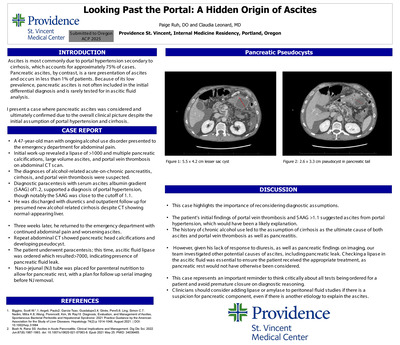
INTRODUCTION: Spur Cell Anemia (SCA) is a rare underrecognized non-autoimmune hemolytic anemia occurring in severe liver disease with prognostic implications. Since the 1980s there have been only a few dozen case reports and clinical images concerning SCA. We present a case of a young man managed in the ICU with multiorgan failure and a masked diagnosis of SCA. DESCRIPTION: A 33-year-old man was found down and presented to the ICU with hematemesis and hemorrhagic shock. He required massive transfusion for bleeding esophageal varices that were later banded and an expanding thigh hematoma. He was diagnosed with alcohol induced liver cirrhosis with a MELD-Na score of 38 and eventually discharged with persistent anemia. He was not a transplant candidate due to recent alcohol use. He returned three weeks later with anasarca and shortness of breath and was diagnosed with hepatorenal syndrome requiring vasopressors. While back in the ICU his hemoglobin declined to 6 g/dL and remained below goal despite transfusion. His continued anemia was thought to be secondary to portal gastropathy and bleeding in his thigh. No active bleeding was found on physical exam or with repeated CT imaging of his hematoma. His LDH and haptoglobin were 653 IU/L and < 1 mg/dL with a total bilirubin of 25.59 mg/dL prompting work up for hemolytic anemia. The peripheral smear demonstrated moderate acanthocytes, which combined with his refractory hemolytic anemia in severe liver disease established a diagnosis of SCA. DISCUSSION: SCA in alcoholic cirrhosis is shown to be an independent predictor of mortality with median reported survival of 1.9 months. SCA is managed with supportive care and rapid evaluation for liver transplant which is the only known effective therapy. Pentoxifylline and flunarizine have been explored with little success in small studies and case reports. These measures were considered for our patient, but ultimately, he was transferred to a transplant center and underwent a successful liver transplant with resolution of his SCA. Our diagnosis of SCA was delayed by focus on his other pathologies that more commonly cause anemia. This illustrates why common issues such as anemia require a broad differential in the ICU where pathology is severe and complex
-

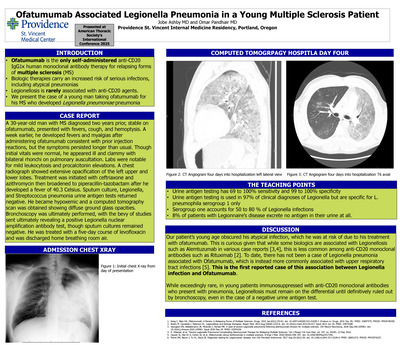
Ofatumumab Associated Legionella Pneumonia in a Young Multiple Sclerosis Patient
Jobe Ashby and Omar Panhair
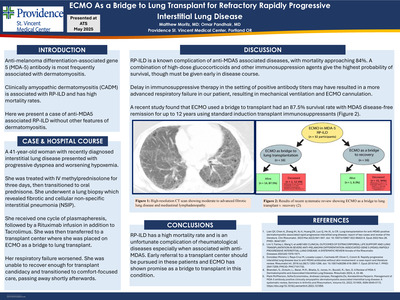
Ofatumumab is the only anti-CD20 IgG1κ human monoclonal antibody therapy for relapsing forms of multiple sclerosis (MS) that patients can self-administer subcutaneously. Anti-CD20 agents are biologic therapies that carry an increased risk of serious infections, but rarely Legionellosis. We present the case of a young man taking ofatumumab for his MS who developed Legionella pneumoniae pneumonia. A 30-year-old man with MS diagnosed two years prior, stable on ofatumumab, presented with fevers, cough, and hemoptysis. A week earlier, he developed fevers and myalgias after administering ofatumumab, but these symptoms persisted longer than usual. Though initial vital signs were normal, he appeared ill and clammy and had bilateral rhonchi on pulmonary auscultation. There was leukocytosis and an elevated procalcitonin level. A chest radiograph showed extensive opacification of the left upper and lower lobes. Treatment with ceftriaxone and azithromycin was initiated. Overnight, he developed a high fever to 40.3 Celsius and treatment was broadened to piperacillin-tazobactam. Sputum culture and urine antigen tests for Legionella and Streptococcus pneumonia were negative. Days later he became hypoxemic, and a computed tomography scan was obtained showing diffuse ground glass opacities. Bronchoscopy was ultimately performed, ultimately revealing a positive Legionella nuclear amplification antibody test, though sputum cultures remained negative. He was treated with levofloxacin for a five-day course with improvement and discharged breathing room air. Our patient’s young age belied his atypical infection, which he was at risk of due to his ofatumumab. While some biologics are associated with Legionellosis such as alemtuzumab, this is less common among anti-CD20 therapies like rituximab. While ofatumumab has been associated with upper respiratory tract infections, this is the first report of an association with Legionella. The final diagnosis in our case was delayed because the Legionella urine antigen testing was negative. Urine antigen testing is commonly used to rule out Legionella as a cause of atypical pneumonia; Urine antigen testing is used in 97% of clinical diagnoses. However, this test is not definitive, despite 69 to 100% sensitivity and 99 to 100% specificity, because it is specific for L. pneumophila serogroup 1 only. Serogroup 1 accounts for 50 to 80 % of Legionella infections and 8% of patients with Legionnaire’s disease excrete no antigen in their urine. This first report demonstrates that in patients immunosuppressed with anti-CD20 therapies presenting with pneumonia, Legionellosis must be considered until definitively ruled out by bronchoscopy, even when urine antigen testing is negative.
-

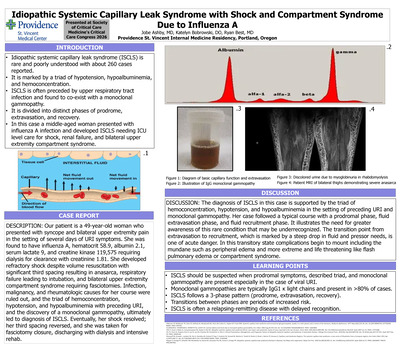
Idiopathic Systemic Capillary Leak Syndrome with Shock and Compartment Syndrome Due to Influenza A
Jobe Ashby, MD; Katelyn Bobrowski, DO; and Ryan Best, MD
INTRODUCTION: Idiopathic systemic capillary leak syndrome (ISCLS) is a rare, poorly understood condition that leads to extreme pathology with severe but predictable complications. First described in 1960, ISCLS has been identified in about 260 case reports and is marked by a triad of hypotension, hypoalbuminemia, and hemoconcentration often preceded by upper respiratory tract infection. It is divided into distinct phases of prodrome, extravasation, and recovery. We present a case of a middle-aged woman who presented with influenza A infection and developed ISCLS needing ICU level care for shock and bilateral upper extremity compartment syndrome. DESCRIPTION: Our patient is a 49-year-old woman who presented with syncope and bilateral upper extremity pain in the setting of several days of URI symptoms. She was found to have influenza A, hematocrit 58.9, albumin 2.1, serum lactate 9, and creatine kinase 119,575 requiring dialysis for clearance with creatinine 1.81. She developed refractory shock despite volume resuscitation with significant third spacing resulting in anasarca, respiratory failure leading to intubation, and bilateral upper extremity compartment syndrome requiring fasciotomies. Infection, malignancy, and rheumatologic causes for her course were ruled out, and the triad of hemoconcentration, hypotension, and hypoalbuminemia with preceding URI, and the discovery of a monoclonal gammopathy, ultimately led to diagnosis of ISCLS. Eventually, her shock resolved; her third spacing reversed, and she was taken for fasciotomy closure, discharging with dialysis and intensive rehab. DISCUSSION: The diagnosis of ISCLS in this case is supported by the triad of hemoconcentration, hypotension, and hypoalbuminemia in the setting of preceding URI and monoclonal gammopathy. Her case followed a typical course with a prodromal phase, fluid extravasation phase, and fluid recruitment phase. It illustrates the need for greater awareness of this rare condition that may be underrecognized. The transition point from extravasation to recruitment, which is marked by a steep drop in fluid and pressor needs, is one of acute danger. In this transitory state complications begin to mount including the mundane such as peripheral edema and more extreme and life threatening like flash pulmonary edema or compartment syndrome.
-

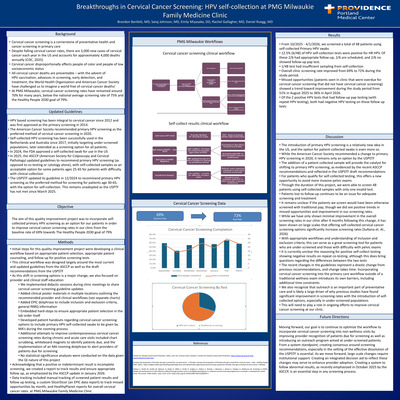
Breakthroughs in Cervical Cancer Screening: HPV self-collection at PMG Milwaukie Family Medicine Clinic
Brandon Bartlett, Sataj Johnson, Emily Miyasako, Rachel Gallagher, and Daniel Ruegg
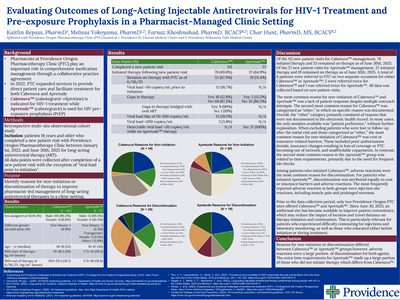
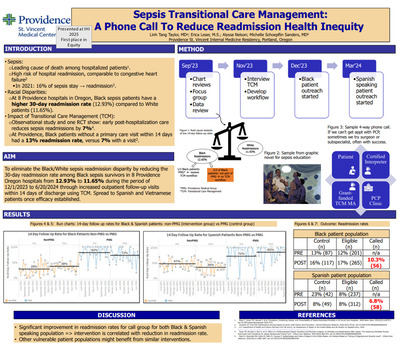
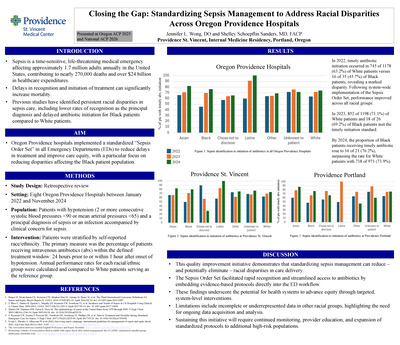
Background: Cervical cancer screening is a cornerstone of preventative healthcare and cancer screening in primary care. Based on data from the CDC, in the US alone, the rate of new cervical cancers each year is ~13,000, accounts for ~4,000 deaths annually, and disproportionally effects people of color and people of low SES (CDC, 2025). In our clinic (PMG Milwaukie), the rate of cervical cancer screening has remained around 70% for years, which is below the national average of ~75% (Healthy People, 2021). Primary HPV screening with self-collected swabs has been used successfully for years outside of the US, improving screening rates, specifically for under-screened groups. In 2024, the FDA approved a self-collected swab for use in the US. In February 2025, the ASCCP (American Society for Colposcopy and Cervical Pathology) updated guidelines to recommend primary HPV screening (as opposed to co-testing or cytology alone), with self-collected samples as an acceptable option for some patients ages 25-65. This is a seismic shift in cervical cancer screening, allowing for less invasive screening options to a multitude of patients for which exam was a barrier to receiving care. Objectives: The aim of this quality improvement project was to incorporate self collected primary HPV screening as an option for our patients to improve cervical cancer screening rates in our clinic. The Healthy People Initiative has set a goal benchmark for cervical cancer screening of 79.2% by 2030. Methods: Given the understanding that self-collected primary HPV screening is a large change from prior guidelines and is a relatively new concept in the US for cervical cancer screening, we first developed a workflow focused on appropriate patient selection and counseling as well as follow up for positive screening tests. As provider education and adoption is essential to this process, we addressed this through didactic sessions, clinical poster materials, and at the bedside through a PARQ dotphrase to aid providers in counseling and appropriate patient selection. As a precaution to ensure appropriate patient selection during the adoption of this new screening process, we embedded a hard stop acknowledgement to ensure providers reviewed eligibility criteria. The final aspect of our workflow is quality assurance. Acknowledging that a positive or indeterminant result is incomplete screening, we created a report to track results and ensure appropriate follow-up. The next process that we are focusing on is adoption of contemporaneous cervical cancer screening for overdue and/or under-screened patients developing strategies to identify and counsel patients due for cervical cancer screening outside of wellness exams. To prompt patients to request screening outside preventative care visits, those identified during the schedule scrub are given patient education handouts highlighting this recent change in screening options during the rooming process. Additionally, we focused on enhancing medical assistant to provider handoffs through an MA rooming dotphrase, whiteboard magnets, and chart scrubbing. Results: From 10/2025 - 2/2026, we screened a total of 39 patients using self-collected Primary HPV swabs. Of these, there were a total of 4 positive HPV results of which ¾ of those had appropriate follow up testing. Of the 39 completed tests, only one was identified as invalid by the lab and not able to be run. Based on the generated SlicerDicer reports in Epic, we did not see any significant change in the overall cervical cancer screening rates in our clinic after the introduction of self-collected primary HPV swabs, after 4 months of adoption Discussion: The introduction of primary HPV screening is a relatively new idea in the US, and the option for patient-collected swabs is even more so. Most patients in our clinic ages 25-65 are being screened using co-testing or cytology with reflex as recommended by the USPTF. While the American Cancer Society recommended a change to primary HPV screening in 2020, it remains only an option by the USPTF. The addition of a patient collected sample will provide the catalyst for shifting to primary HPV screening, as evidenced by the recent ASCCP recommendations and reflected in the USPSTF draft recommendations. For patients who qualify for self-collected testing, this offers a new opportunity to avoid more invasive pelvic exams. Through the duration of this project, we were able to screen 39 patients using self-collected samples with only one invalid test and one patient lost to follow up after a positive result. With appropriate workflows and understanding of inclusion and exclusion criteria, this can serve as a great screening tool for patients who are under screened and those with difficulty with pelvic exams. While we have yet to show any improvement in the overall screening rates in our clinic after 4 months following this change, it has been shown on large scales that offering self-collected cervical cancer screening options significantly increase screening rates (Sultana et. Al., 2026). The recent changes in the guidelines represent a drastic change from previous recommendations, and change takes time. Incorporating cervical cancer screening into the primary care workflow outside of a traditional wellness exam introduces its own barriers, including additional time constraints. We also recognize that outreach is an important part of preventative care and will likely play a role in ongoing efforts to improve cervical cancer screening at our clinic. Moving forward, our goal is to continue to optimize the workflow to incorporate cervical cancer screening into non-wellness visits by improving provider recognition of patients due for screening as well as introducing an outreach program aimed at under-screened patients. From a system standpoint, creating consensus around screening recommendations, especially in the setting of the effective dissolution of the USPSTF is essential. As we move forward, large scale changes require institutional support. Creating an integrated decision aid to reflect these changes may serve to enhance provider adoption. Creating a system to follow abnormal results, as recently emphasized in October 2025 by the ASCCP, is an essential step in any screening process.
-
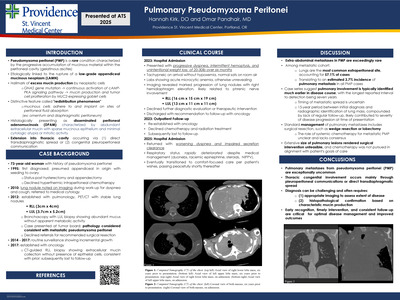
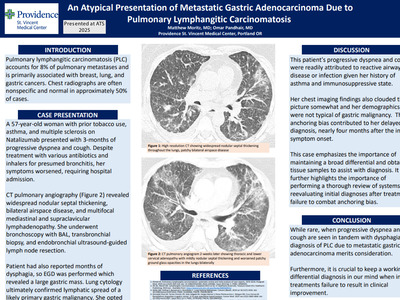
 In Acute Chest Syndrome by Natalie Bolton, MD and Omar Pandhair")
Extracorporeal Membrane Oxygenation (ECMO) In Acute Chest Syndrome
Natalie Bolton, MD and Omar Pandhair
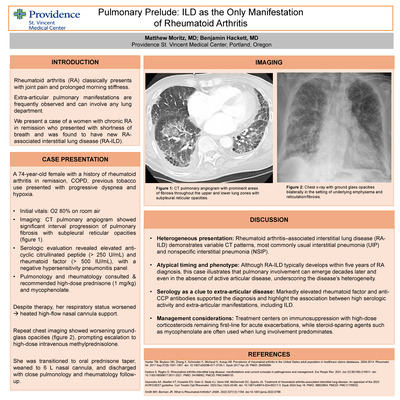
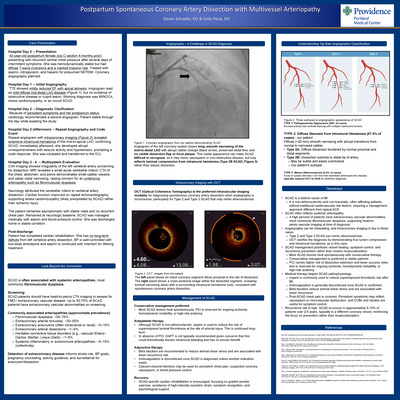
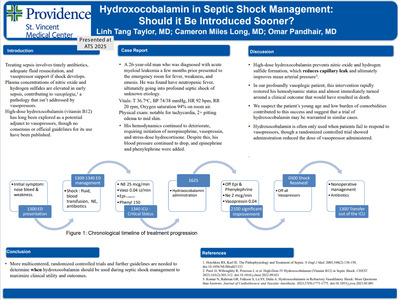
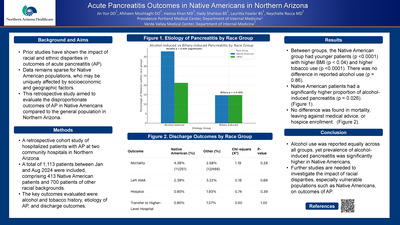
Introduction: Acute chest syndrome (ACS) is a severe complication of sickle cell disease. Rarely, it may progress to acute respiratory distress syndrome (ARDS). Inability to oxygenate despite mechanical ventilation necessitates consideration of extracorporeal membrane oxygenation (ECMO). Case Summary: A 31-year-old man with sickle cell disease presented with low back pain similar to prior pain crises. Vital signs were normal, and his hemoglobin level was 10.2 g/dL, with a reticulocyte index of 0.05. He was admitted for pain control and rehydration. That night, he developed fever, tachypnea, and hypoxemia with imaging showing a right lower lobe infiltrate, consistent with ACS. He was treated with broad-spectrum antibiotics and escalated to high flow nasal cannula. Hematology recommended transfer to a center capable of exchange transfusion, and he was admitted to the intensive care unit in the interim. Repeat hemoglobin level decreased to 8.0 g/dL and a stat transfusion was ordered. Despite noninvasive ventilation, he remained hypoxemic and endotracheal intubation was performed; however, he remained hypoxemic and suffered a cardiac arrest with successful resuscitation within three minutes, though he developed shock. His hemoglobin level rapidly dropped to 4.3 g/dL. He received multiple transfusions and vasopressor support and remained persistently hypoxemic and with worsening lactic acidosis. He was found to have severe right heart failure on echocardiography and underwent placement of a Protek Duo right ventricular assist device before transferring to a tertiary center. Continuous renal replacement therapy was started and despite transition to veno-arterial-venous ECMO for new onset left ventricular failure, he suffered a ventricular tachycardia arrest and expired. Discussion: This case highlights the need for early recognition and management of both acute vaso-occlusive crisis requiring transfusion support and refractory ARDS potentially needing ECMO. Our patient’s hemoglobin level was not re-checked until he arrived in the ICU, by which time it dropped significantly. Earlier supportive transfusion may have provided benefit, targeting a goal hemoglobin level of at least 10g/dL. Employment of ECMO for management of ACS is rare, and limited data suggests cohorts including adults have a lower survival rate compared to exclusively pediatric cases (27% vs. 52%). Due to this rarity, there are no official guidelines on if or when to use ECMO in ACS. With advances in this therapy, including awake ECMO, we advocate for further study to determine whether earlier initiation of ECMO may be beneficial in saving the lives of young, otherwise healthy sickle cell patients such as ours.
-

Phenazopyridine-induced sulfhemoglobinemia: A diagnostic and management dilemma
Natalie Bolton, MD; Linh Tang Taylor, MD; Kristy Poonyagarlyagorn, MD; and Cameron Long, MD
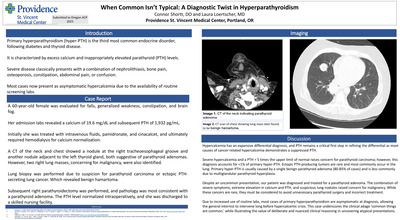
Introduction: Sulfhemoglobinemia is a rare dyshemoglobinemia which occurs when sulfur irreversibly binds to hemoglobin. Presents similarly to methemoglobinemia. Common offending medications: dapsone, acetanilide, phenacetin, and nitrates. Rarely observed secondary to phenazopyridine, an over-the counter medication used to treat dysuria. Few facilities are capable of testing for sulfhemoglobinemia Case Background: A 67-year-old woman with recurrent urinary tract infections and interstitial cystitis presented with encephalopathy and recurrent falls for three days. PMH: multiple sclerosis, recurrent urinary tract infections, asthma, neurogenic bladder, neuropathic pain, and obstructive sleep apnea. Chronically on multiple centrally acting medications. Not on medications for multiple sclerosis due to cost. Has many urinary tract infections annually Usually infected with antibiotic resistant bacteria, including escheria coli, raoultella ornithinolytica, and klebsiella pneumoniae. Often requires meropenem to treat for infections given degree of resistance. Per husband, chronically takes large doses of phenoazopyridine (available over the counter as Azo) to treat her interstitial cystitis Dosage: Recommended: no more than 2 days without consulting doctors Actual: multiple bottles of Azo weekly Conclusion: 1. Sulfhemoglobinemia is rare & difficult to diagnose, unlike ethemoglobinemia which is uncommon but easily identified & diagnosed 2. Common causes of sulhemoglobinemia: medications, including over-the counter drugs such as phenazopyridine 3. Rapid identification of the uncommon conditions are key in managing patients with one or both of these dyshemoglobinemias
-
 Infection by Natalie Bolton and Jeffrey Youker")
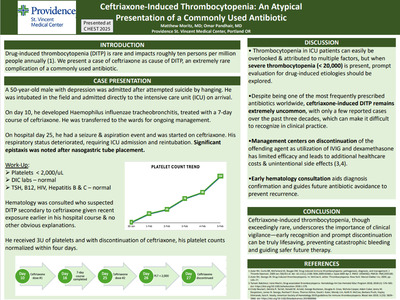
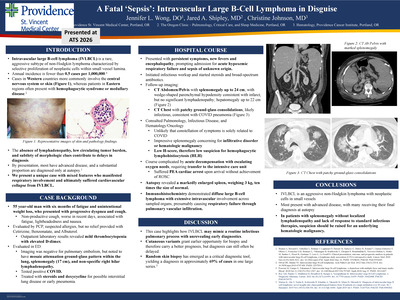
A Rare and Fatal Complication of Herpes Simplex Virus (HSV) Infection
Natalie Bolton and Jeffrey Youker
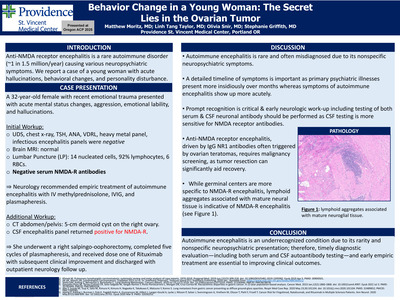
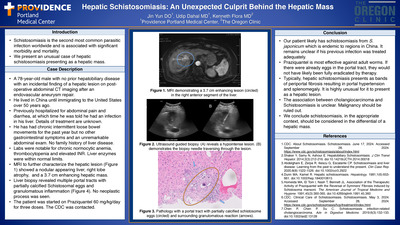
Introduction: Hemophagocytic Lymphohistiocytosis (HLH) is a rare syndrome characterized by overactive immune activation, cytokine storm, and uncontrolled hemophagocytosis. Primary HLH is familial and most often seen in infants, whereas secondary HLH occurs more frequently in adults and is triggered by infections, malignancies, or autoimmune disorders. Clinically, secondary HLH often mimics sepsis but fails to respond to standard therapies, contributing to delayed diagnosis and treatment. Without timely intervention, HLH can result in extensive tissue damage, multiorgan failure, and death. In rare cases, central nervous system (CNS) involvement may occur, manifesting as histiocytic infiltration that can be misinterpreted as malignancy or infection. Case Presentation: A 51 year-old man presented with four days of nausea, vomiting, diarrhea, and fevers. Initial evaluation revealed persistent hypotension, severe transaminitis, neutropenia, thrombocytopenia, and penile lesions, prompting ICU admission. Hemodynamic stability was achieved with fluid administration and empiric antibiotics, after which the patient was transferred to the general ward and started on acyclovir following positive HSV results from genital lesion swabs and CSF samples. Subsequently, the patient developed acute renal failure, encephalopathy, and hepatic failure, suspected to be secondary to HSV hepatitis, necessitating ICU readmission. Due to the severity of organ dysfunction, N-acetyl-cysteine and continuous renal replacement therapy (CRRT) were initiated. Although HLH was initially considered unlikely due to its rare association with HSV, further evaluation confirmed the diagnosis. The patient was treated with high-dose steroids and etoposide chemotherapy, resulting in clinical improvement and transfer out of critical care. However, the patient later experienced recurrent encephalopathy. Brain MRI revealed multifocal lesions suggestive of HLH related infiltrative disease. Neurologic deterioration progressed to anisocoria and loss of brainstem reflexes, and repeat CT imaging revealed new lesions with mass effect and brain stem compression. Despite aggressive management, the patient succumbed to the disease. Discussion: This case underscores a complex diagnostic and therapeutic challenge involving a rare etiology of HLH. The clinical overlap between HLH and sepsis, both capable of causing multiorgan failure, contributes to under-recognition and delayed treatment. Initial management focused on treating HSV infection and its complications, which inadvertently postponed HLH diagnosis. Delayed recognition and initiation of immunosuppressive therapy, including corticosteroids and etoposide, are associated with increased mortality. Conclusions: This case highlights the importance of maintaining a high index of suspicion for HLH in patients with severe systemic illness, particularly when clinical deterioration persists despite appropriate treatment for presumed sepsis. Early identification and prompt initiation of HLH-directed therapy are critical to improving outcomes.
-

GLP-1 Medication Risk Assessment
Brendan Bu, PharmD
GLP‑1 receptor agonists are increasingly prescribed across diverse clinical settings. As overall utilization of these drugs increase, there has also been an associated uptick in reported patient safety concerns. Some of these reports have been associated with unconventional dosing schedules, product transitions, and evolving therapeutic uses. To assess these risks within PMG Oregon, a Common Cause Analysis (CCA) was conducted to evaluate all GLP‑1– related medication safety events reported between September 2023 and September 2025. A total of 27 events were identified, including near misses, precursor events, and patient‑reaching errors, and were analyzed by event type, MERP stage, contributing human factors, and system-level vulnerabilities. Most safety events originated during the prescribing or ordering stage, highlighting early workflow vulnerabilities related to incorrect dose selection, titration errors, and inappropriate starting doses when switching GLP‑1 products. Dispensing events represented the second most common category, while transcription errors occurred less frequently. These errors resulted in a range of patient outcomes—from no harm to significant gastrointestinal illness, dehydration, acute kidney injury, and emergency department visits. Human factor analysis demonstrated that consciousness-related lapses (IE: slips, inattention, interruptions) were the most frequently reported contributors, followed by critical thinking and competency-related errors. System-level contributors were dominated by policy and procedure gaps, process breakdowns, and technology limitations such as inappropriate EHR defaults and lack of automated guardrails. Issues related to storage and handling of Medication Assistance Program (MAP) products further reflected workflow vulnerabilities at individual clinics. Unfortunately, limited or incomplete documentation within the HRP events limits the ability to assess and identify patterns and characteristics fully. However, the analysis shows that GLP‑1 medication errors arise from intersecting human, workflow, and system factors. Opportunities for improvement include standardizing titration workflows, implementing EHR‑based safeguards, strengthening MAP handling processes, and clarifying caregiver roles to create a safer prescribing environment for GLP‑1 therapies. (IRB Exempt)
-

The Rash After the Remedy
Elaine Chen, MD
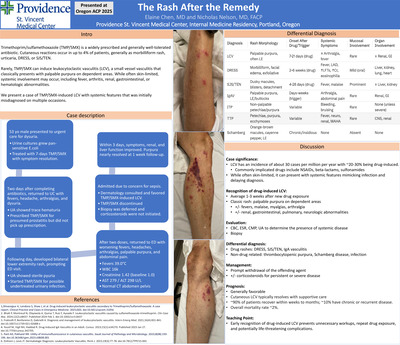
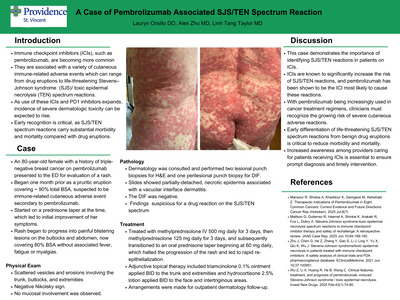
Introduction: Trimethoprim/sulfamethoxazole (TMP/SMX) is a widely prescribed and generally well-tolerated antibiotic. Cutaneous reactions occur in up to 4% of patients, including morbilliform rash, urticaria, DRESS, Stevens-Johnson syndrome, and toxic epidermal necrolysis. More rarely, TMP/SMX can trigger leukocytoclastic vasculitis (LCV), a small-vessel vasculitis characterized by neutrophilic infiltration, fibrinoid necrosis, and leukocytoclasia. LCV typically manifests as palpable purpura on dependent areas. While often skin-limited, systemic involvement may occur. We present a case of TMP/SMX-induced LCV with multi-organ features. Case description: A 53-year-old healthy male presented to urgent care with dysuria. Urine culture grew pan-sensitive E. coli, and he completed a 7-day course of TMP/ SMX with symptom resolution. Two days later, he returned with fevers, headaches, arthralgias, and dysuria. Urinalysis showed trace hematuria, and he was re-prescribed TMP/SMX for presumed prostatitis. Before restarting, his fevers improved but he developed a bilateral lower-extremity rash, prompting ED evaluation. TMP/SMX was re-prescribed a third time for possible undertreated infection. After two doses, he returned with worsening fevers, headaches, arthralgias, progressive palpable purpura, and abdominal pain. He was febrile to 39.0°C with creatinine 1.42 mg/dL (baseline 1.0), WBC 16K, Hgb 12 g/dL, platelets 127K, AST 279 U/L, ALT 298 U/L, and was admitted for concern of sepsis. Dermatology was consulted and favored TMP/SMX induced LCV. Biopsy was deferred, and corticosteroids were not initiated. Following drug discontinuation, his symptoms and renal function improved within 3 days, and purpura nearly resolved at 1 week. Discussion: LCV is rare, with an incidence of ~30 per million annually, and 10-20% of cases being drug-induced. Other causes of LCV include infections, autoimmune disorders, malignancies, and idiopathic. Symptoms typically arise within 1-3 weeks of exposure and present with palpable purpura, sometimes accompanied by fever, arthritis, renal, gastrointestinal, or hematologic involvement. The diagnosis here was supported by the classic rash, temporal association with TMP/SMX, worsening on re-exposure, and rapid improvement after withdrawal. Other TMP/SMX reactions were considered, as it can cause hepatitis, and a physiologic creatinine elevation of ~17-31% via inhibition of tubular secretion. This patient’s creatinine exceeded that range and coincided with palpable purpura, supporting LCV rather than DRESS or TEN/SJS. Drug-induced IgA vasculitis was also possible, as it can mimic LCV with multi-organ involvement. In this case, drug-induced LCV was favored, as IgA vasculitis is rarer. Management is drug withdrawal, with resolution usually within 2-3 weeks. Corticosteroids are reserved for severe or refractory disease. The prognosis is favorable with prompt withdrawal of the drug. TMP/SMX-induced LCV is a rare but important adverse reaction. Clinicians should suspect it in patients with new palpable purpura after medication exposure. Early recognition and drug withdrawal are crucial to prevent repeat exposure, unnecessary testing, and serious complications.
-

Snuggles, not struggles: evaluation of a post-operative pain management protocol in a level III community NICU
MaLeane Chin, Danielle Megano, Aiyana Ooki-Knutson, and Deasy Erin Wilson
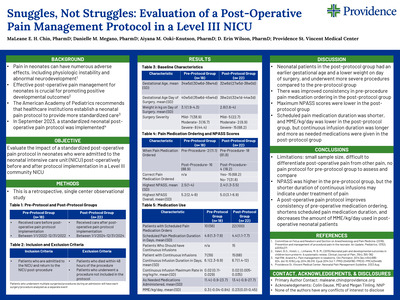
Abstract: Neonates are an extremely sensitive population often subject to painful interventions. This pain can have numerous adverse effects including physiologic instability, altered brain development, and abnormal stress responses, which can persist into childhood. Effective post-operative pain management for neonates is crucial for promoting positive developmental outcomes. No specific post-operative pain protocol for neonatal patients has shown to be most effective, so the American Academy of Pediatrics recommends that healthcare institutions establish a neonatal pain protocol to provide more standardized care. This project is a retrospective, single center observational study determined to be exempt by the institutional review board. Infants cared for in a Level III community neonatal intensive care unit (NICU) between January 1, 2022 and December 31, 2022 receiving post-operative care prior to the implementation of a standardized post-operative pain protocol, and between January 1, 2024 and December 31, 2024 receiving post-operative care after the implementation of a standardized post-operative pain protocol will be identified. Infants with pain following procedures not included in the policy and patients who died within 48 hours of the procedure will be excluded. Data collected will include gestational age at birth, corrected gestational age on date of surgery, weight, date and type of operation, operating surgeon, adherence to protocol, NPASS scores, total amount of morphine milligram equivalents, duration of continuous analgesic infusions and scheduled pain medications, number of as needed analgesics administered, and post-operative complications. Based on this information, the impact and clinical outcomes of a standardized postoperative pain protocol in a level III community NICU can be evaluated. Results and conclusions will be presented. Learning Objectives: Evaluate the impact of a standardized post-operative pain protocol in neonates who were admitted to the neonatal intensive care unit (NICU) post-operatively before and after protocol implementation in a Level III community NICU Presentation Category: Pediatrics
-

Supplement Risk
Allison Connor, BS; Linh Tang Taylor, MD; and Jeffrey Youker, MD
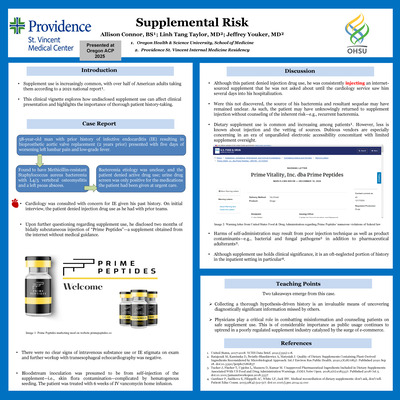
Introduction: Increasingly, it is the case that patients are using a variety of supplements. About half of American adults use supplements. ¹. The purpose of this case report is to consider the impact of surreptitious supplement use on clinical presentation and under score the value in gathering a robust patient history. Case report: A 58-year-old man with prior history of infective endocarditis (IE) resulting in bioprosthetic aortic valve replacement (2 years prior) presented with worsening left lumbar pain and low-grade fever. He was found to have Methicillin resistant Staphylococcus aureus bacteremia with L4/5 vertebral osteomyelitis and a left psoas abscess. The bacteremia etiology was unclear, and patient denied active drug use; urine drug screen was positive for the medications the patient had been given at urgent care. Cardiology was consulted with concern for IE given his past medical history. Upon further probing however, the patient disclosed 2 months of bidaily subcutaneous injection of a peptide supplement obtained from the internet without medical guidance. There were no clear signs of intravenous substance use or IE stigmata on exam and subsequent workup with transesophageal echocardiography was negative. Bloodstream inoculation was presumed to be from self-injection of the supplement complicated by hematogenous seeding. The patient Was treated with 6 weeks of IV vancomycin home infusion. Discussion: Although this patient denied injection drug use, he was consistently injecting an unregulated internet-sourced peptide supplement that he was not asked about until the cardiology service saw him several days into his hospital course. Were this not discovered, the source of his bacteremia and resultant sequelae may have remained unclear. As such, the patient may have unknowingly returned to supplement injection without counseling of the inherent risk; hence, continuing the vicious cycle of introducing nidus for recurrent bacteremiaDietary supplement use is common and increasing among patients¹. However, less is known about the vetting of supplement sources and non-oral methods of administration. Dubious vendors of products and information are especially concerning in an era of unparalleled electronic accessibility concomitant with limited supplement oversight. Harms of self-administration may result from poor injection technique as well as product contaminants—e.g., bacterial and fungal pathogens². Pharmaceutical adulterants are another possible source of injury³. Although supplement use holds clinical significance, it is an oft-neglected portion of history in the inpatient setting in particular⁴. Conclusion --- There are 2 takeaways from this case. 1) Collecting a thorough history is an invaluable means of uncovering diagnostically significant information missed in prior interviews. 2) Physicians play a critical role in combatting medical misinformation and counseling patients on safe and appropriate supplement use. This is of considerable importance as public usage continues to uptrend in a poorly regulated supplement industry catalyzed by the surge of e-commerce.
-
An Exploration of Positive Psychology Practices in an Integrated Primary Care Setting
Rebecca Crowder and Carissa Bravo
Positive psychology is a theory of well-being which scientifically studies factors that promote human flourishing (Seligman, 2018). The pillars of positive psychology are defined by the acronym PERMA, which is a framework for positive emotion, engagement, relationships, meaning, and accomplishment. Positive psychology seeks to find the character strengths and behaviors that can help people move beyond surviving and into flourishing (Seligman, 2018). Increasingly, primary care professionals report mental fatigue and burnout due to heavy workloads, limited resources, and ongoing exposure to suffering (Clifton et al., 2021, Batanda, 2024; Kober, 2024). Through principles derived from positive psychology, this project aimed to incrementally promote well-being and psychological resilience in healthcare professionals in a primary care setting. A one-week program inclusive of a didactic in Positive Psychology was provided to primary care physicians; a team-based digital exercise of brief daily well-being insights and simple practices were shared with the medical clinic staff. A pre and post assessment (i.e., Flourishing Scale (FS), and Brief Resilience Scale (BRS)) were facilitated to evaluate the perceived level of well-being and psychological resilience in primary care professionals
-

Diagnostic Overlap in HUS: an Atypical Case
Ryan Daily, Med, DO and Andrea Roast, MD
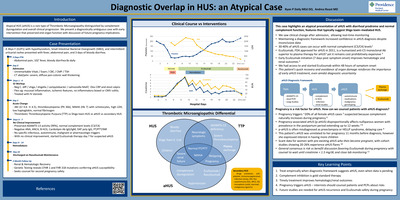
Introduction: Atypical HUS (aHUS) is a rare type of Thrombotic Microangiopathy distinguished by complement dysregulation and overall clinical progression. We present a diagnostically ambiguous case with early intervention that preserved end-organ function with discussion of future pregnancy implications. Case Presentation: A 36yo F (G2P1) with hypothyroidism, Small Intestinal Bacterial Overgrowth (SIBO), and intermittent urticarial rashes presented with fever, abdominal pain, and 3 days of bloody diarrhea. Discussion: This case highlights an atypical presentation of aHUS with diarrheal prodrome and normal complement function, features that typically suggest Shiga toxin–mediated HUS. We saw clinical change after admission, allowing real-time monitoring. Maintaining a diagnostic framework increased confidence in aHUS diagnosis despite inconclusive data. 30-40% of aHUS cases can occur with normal complement (C3/C4) levels. Eculizumab, FDA approved for aHUS in 2011, is a humanized anti-C5 monoclonal Ab superior to plasma therapy for aHUS2 yet it remains cost prohibitively expensive. Early Eculizumab initiation (7 days post symptom onset) improves hematologic and renal outcomes. We had access to and started Eculizumab within 48 hours of symptom onset, This patient's quick recovery and avoidance of organ damage reinforces the importance of early aHUS treatment, even amidst diagnostic uncertainty
-

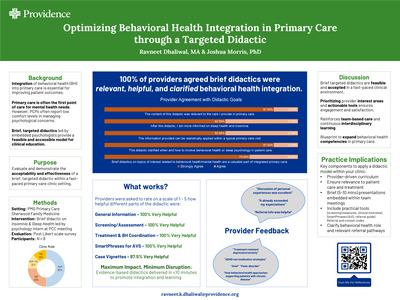
Optimizing Behavioral Health Integration in Primary Care through a Targeted Didactic
Ravneet Dhaliwal, M.A., Behavioral Health Intern and Joshua Morris
Background: The integration of behavioral health into primary care settings is an essential strategy for improving patient outcomes, increasing access to mental health services, and achieving the Triple Aim of healthcare.1, 2 To maximize this integration and bridge the gap for primary care providers (PCPs), targeted didactic training and continued education are pivotal. National surveys indicate that PCPs often report low comfort levels in managing psychological concerns due to a lack of formal training, despite the high prevalence of these issues in primary care. 3, 4 Brief didactics facilitated by embedded behavioral health psychologists offer an accessible, adaptable method for disseminating evidence-based information.1 However, the success of this model hinges on its feasibility within a busy clinical environment and its acceptability to the providers. Method: This quality improvement project implements a targeted didactic on sleep health, a topic identified as a high-priority interest in a preliminary provider survey at PMG Sherwood Family Medicine. The 10-minute didactic will be delivered during a scheduled monthly provider meeting to minimize disruption to clinical workflows. Following the presentation, providers will complete a brief satisfaction survey assessing the relevance of content and satisfaction. The researcher will qualitatively evaluate the feasibility of this delivery model and the barriers to implementation. Anticipated Results: It is anticipated that the targeted didactic will be rated moderately to highly acceptable and relevant to primary care practice. Expected outcomes include high provider satisfaction and a stated interest in future didactics tailored to clinic-specific needs. Qualitative results are expected to highlight the value of having embedded behavioral health experts to provide "on-the ground" specialty training that is relevant and applicable to patient care and barriers. Conclusion: This project plans to demonstrate that brief, evidence-based didactics are an effective method for enhancing behavioral health integration in primary care. By addressing specific provider identified interest areas, such as sleep health, embedded psychologists can foster a culture of continuous learning and interdisciplinary collaboration.5 Future iterations of this model could serve as a blueprint for expanding behavioral health competencies across diverse primary care teams, ultimately contributing to more holistic patient care and improved population health outcomes.
-

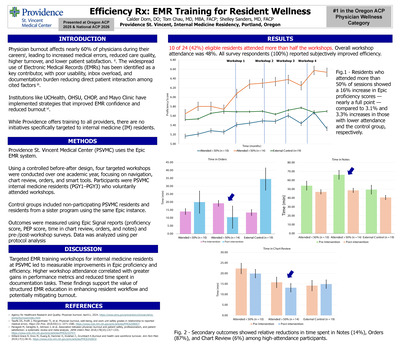
Efficiency Rx: EMR Training for Resident Wellness
Calder Dorn, DO; Tom Chau, MD, MBA, FACP; and Shelley Sanders, MD, FACP
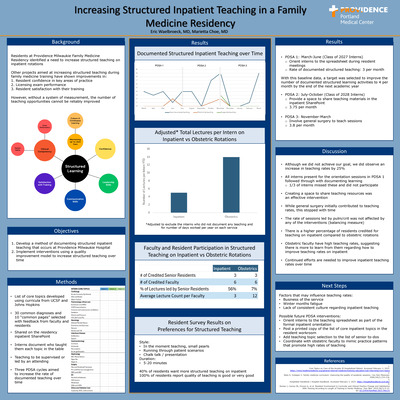
Introduction: Physician burnout affects nearly 60% of physicians during their careers, leading to increased medical errors, reduced care quality, higher turnover, and lower patient satisfaction. ii. The widespread use of Electronic Medical Records (EMRs) has been identified as a key contributor, with poor usability, inbox overload, and documentation burden reducing direct patient interaction among cited factors iii. Institutions like UCHealth, OHSU, CHOP, and Mayo Clinic have implemented strategies that improved EMR confidence and reduced burnout vi. While Providence offers training to all providers, there are no initiatives specifically targeted to internal medicine (IM) residents. Methods: Providence St. Vincent Medical Center (PSVMC) uses the Epic EMR system. Using a controlled before-after design, four targeted workshops were conducted over one academic year, focusing on navigation, chart review, orders, and smart tools. Participants were PSVMC internal medicine residents (PGY1–PGY3) who voluntarily attended workshops. Control groups included non-participating PSVMC residents and residents from a sister program using the same Epic instance. Outcomes were measured using Epic Signal reports (proficiency score, PEP score, time in chart review, orders, and notes) and pre-/post -workshop surveys. Results: Overall workshop attendance among residents was 48%. Residents who attended more than 50% of sessions showed a 16% increase in Epic proficiency scores—nearly a full point—compared to 3.1% and 3.3% increases in those with lower attendance and the control group, respectively. Secondary outcomes showed relative reductions in time spent in Notes (14%), Orders (87%), and Chart Review (6%) among high-attendance participants. All survey respondents (100%) reported subjectively improved efficiency from the workshops. Conclusion: \Targeted EMR training workshops for internal medicine residents at PSVMC led to measurable improvements in Epic proficiency and efficiency. Higher workshop attendance correlated with greater gains in performance metrics and reduced time spent in documentation tasks. These findings support the value of structured EMR education in enhancing resident workflow and potentially mitigating burnout.
-

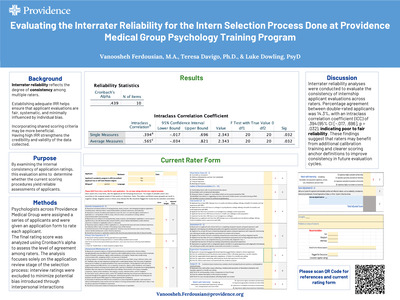
Evaluating the Interrater Reliability for the Intern Selection Process Done at Providence Medical Group Psychology Training Program
Vanoosheh Ferdousian, M.A.; Teresa Davigo; and Luke Dowling
Interrater reliability (IRR) is an important component of evaluation processes that involve subjective judgments, as it reflects the degree of consistency among multiple raters. In training and hiring contexts, establishing adequate IRR helps ensure that applicant evaluations are fair, systematic, and minimally influenced by individual bias. The present program evaluation examines the interrater reliability of the intern selection process at the Providence Medical Group Psychology Training Program. Specifically, this project evaluates the consistency of raters’ scores assigned to internship applicants using the program’s standardized application rating forms. Numerical ratings from multiple reviewers were collected for each applicant and analyzed using Cronbach’s alpha to assess the level of agreement among raters. The analysis focuses solely on the application review stage of the selection process; interview ratings were excluded to minimize potential bias introduced through interpersonal interactions. By examining the internal consistency of application ratings, this evaluation aims to determine whether the current scoring procedures yield reliable assessments of applicants. Findings from this project may inform future refinements to the internship selection process, including clarification of rating criteria and improvements to reviewer training, ultimately supporting a more equitable and consistent evaluation system.
-
Evaluation of Clinical Pharmacist-Led Ambulatory Blood Pressure Monitoring Service and its Impact on Hypertension Outcomes in a Primary Care Setting
Ariel Ford, PharmD; Justin Bachman, PharmD, BCACP; and Abby Frye, PharmD, BCACP
Abstract: Based on current hypertension treatment guidelines, ambulatory blood pressure monitoring (ABPM) is one of the preferred methods to obtain out-of office BP measurements for the diagnosis and management of hypertension. It is considered the gold-standard for identifying white-coat hypertension, masked hypertension, and resistant hypertension. ABPM is commonly underutilized due to cost and other factors, which has the potential to contribute to hypertension treatment disparities. In 2017, a pharmacist-led ABPM service was introduced at Providence Medical Group (PMG) at St. Vincent. During the first year of use at PMG at St. Vincent, 53 patients completed ABPM, and the results were positive: 87% of pharmacist recommendations were accepted and/or implemented and 84% of patients were at their HTN goal at follow-up. Since then, pharmacist-led ABPM services have been implemented at many other PMG primary care clinics in Oregon; however, the impact of this expansion has not been studied. The purpose of this study is to evaluate the impact of pharmacist-led ABPM services on hypertension outcomes in the primary care setting. This is a multi-center retrospective chart review that used a Slicer Dicer report to identify the total number of ABPM exams completed at PMG Oregon Primary Care clinics from April 1, 2024, to April 1, 2025. One hundred and fifty patients were randomly selected for data collection. Patients whose ABPM results were not evaluated by a clinical pharmacist or did not complete ABPM were excluded. Data collection will include baseline characteristics and demographics, reason for referral, baseline blood pressure, ABPM findings, relevant medication changes, pharmacist clinical intervention, and blood pressure findings at least six months after ABPM. Collected data will be used to assess whether pharmacist recommendations were implemented and the impact that recommendation had on blood pressure control. Results and conclusions will be shared upon completion of this clinical inquiry. (IRB exempt) Learning Objectives: Describe the impact of pharmacist-led ambulatory blood pressure monitoring services on hypertension outcomes Presentation Category: Ambulatory Care/Disease State Management
-
 Gan, DO")
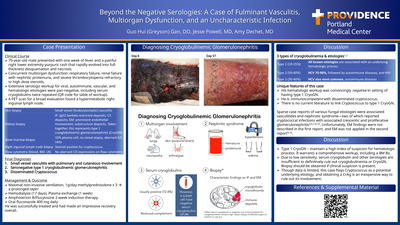
Beyond the Negative Serologies: A Case of Fulminant Vasculitis, Multiorgan Dysfunction, and an Uncharacteristic Infection
Guo Hui (Greyson) Gan, DO
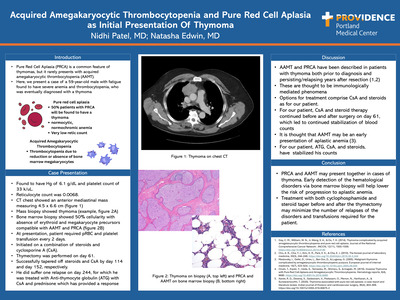
Case Presentation: 70-year-old male presented with one week of fever and a painful right lower extremity purpuric rash that rapidly evolved into fullthickness desquamation and necrosis. Concurrent multiorgan dysfunction: respiratory failure, renal failure with nephritic proteinuria, and severe thrombocytopenia refractory to high dose steroids. Extensive serologic workup for viral, autoimmune, vascular, and hematologic etiologies were pan-negative, including serum cryoglobulins twice repeated (QR code for table of workup). A PET scan for a broad evaluation found a hypermetabolic right inguinal lymph node. Discussion: Unique features of this case: His hematologic workup was convincingly negative in setting of having type 1 CryoGN. He is immunocompetent with disseminated cryptococcus. There is no current literature to link Cryptococcus to type 1 CryoGN. Sparse case reports of various fungal etiologies were associated vasculitides and nephrotic syndrome—two of which reported cryptococcal infections with associated crescentic and proliferative glomerulonephritis5,6,7,9,10. Unfortunately, EM findings were not described in first report and EM was not applied in the second report. Type 1 CryoGN – maintain a high index of suspicion for hematologic process. It warrants a comprehensive workup, including a BM Bx. Due to low sensitivity, serum cryoglobulin and other serologies are insufficient to definitively rule out cryoglobulinemia or CryoGN. Biopsy should be obtained if clinical suspicion is present. Though data is limited, this case flags Cryptococcus as a potential underlying etiology, and obtaining a CrAg is an inexpensive way to rule out its involvement.
-

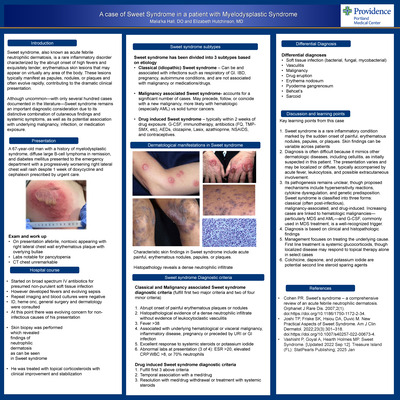
A case of sweet Syndrome in a patient with Myelodysplastic Syndrome
Malia’ka Hall, DO and Elizabeth Hutshinson, MD
Introduction: Sweet syndrome, also known as acute febrile neutrophilic dermatosis, is a rare inflammatory disorder characterized by the abrupt onset of high fevers and exquisitely tender, erythematous skin lesions that may appear on virtually any area of the body. These lesions typically manifest as papules, nodules, or plaques and often evolve rapidly, contributing to the dramatic clinical presentation. Although uncommon—with only several hundred cases documented in the literature—Sweet syndrome remains an important diagnostic consideration due to its distinctive combination of cutaneous findings and systemic symptoms, as well as its potential association with underlying malignancy, infection, or medication exposure. Presentation: A 67‑year‑old man with a history of myelodysplastic syndrome, diffuse large B‑cell lymphoma in remission, and diabetes mellitus presented to the emergency department with a progressively worsening right lateral chest wall rash despite 1 week of doxycycline and cephalexin prescribed by urgent care. Discussion: Key learning points from this case; Sweet syndrome is a rare inflammatory condition marked by the sudden onset of painful, erythematous nodules, papules, or plaques. Skin findings can be variable across patients. Diagnosis is often difficult because it mimics other dermatologic diseases, including cellulitis, as initially suspected in this patient. The presentation varies and may be localized or diffuse, typically accompanied by acute fever, leukocytosis, and possible extracutaneous involvement.Its pathogenesis remains unclear, though proposed mechanisms include hypersensitivity reactions, cytokine dysregulation, and genetic predisposition. Sweet syndrome is classified into three forms: classical (often post‑infectious), malignancy‑associated, and drug‑induced. Increasing cases are linked to hematologic malignancies— particularly MDS and AML—and G‑CSF, commonly used in MDS treatment, is a well‑recognized trigger. Diagnosis is based on clinical and histopathologic findings Management focuses on treating the underlying cause. First line treatment is systemic glucocorticoids, though localized disease may respond to topical therapy alone in select cases Colchicine, dapsone, and potassium iodide are potential second line steroid sparing agents
-
Evaluation of blood culture contamination: impact on antibiotic use and clinical outcomes
Natalie Hart, PharmD; Nyles Fowler; and Emily Fox
Abstract: Blood cultures are one of the most frequently ordered microbiological tests in the hospital. While this diagnostic tool is necessary for determining management of certain infections, contaminated samples often lead to unnecessary antibiotic administration. Blood culture contamination is a critical aspect of antimicrobial stewardship, as previous literature has shown that treatment of a blood culture contaminant is associated with increased hospital costs, length-of-stay, morbidity, and mortality rates. To better understand the impact of blood culture contamination on patients within our facility, we evaluated antibiotic use and other patient outcomes associated with contaminated blood cultures. This was a single-center retrospective cohort study at a tertiary care hospital. Adult patients with two sets of blood cultures drawn within 24 hours of presentation to the hospital from March to August 2025 were screened for inclusion. Patients were excluded if only one set of blood cultures is drawn, if patient was not admitted to hospital, if true-positive blood culture not meeting microbiological contaminant definition, or neutropenic defined as absolute neutrophil count less than 500 cells/uL. The primary outcome was overall days of inpatient antibiotics in patients with contaminated blood cultures in comparison to patients with negative blood cultures. Secondary outcomes included in-hospital mortality, hospital length-of-stay, incidence of repeat blood cultures obtained, incidence of antibiotic escalation (addition of anti-MRSA therapy), and transthoracic echocardiograms performed. Patients were identified utilizing the electronic health record (EHR) and chart review was performed to record patient demographics (age, sex, BMI), patient characteristics (comorbidities, infection type), and evaluate the primary and secondary outcomes. Statistical analysis was performed utilizing student t-tests for continuous variables, chi-squared tests for categorical variables. A P-value of less than 0.05 was considered statistically significant. Results and conclusions will be shared when the project is completed. (IRB approved) Learning Objectives: Describe and evaluate clinical outcomes associated with contaminated blood culture results. Presentation Category: Antibiotic Stewardship
-

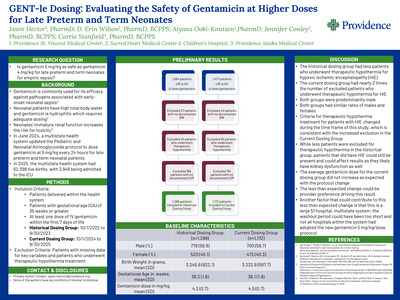
GENT-le Dosing: Evaluating the Safety of Gentamicin at Higher Doses for Late Preterm and Term Neonates
Jason Hector, D. Erin Wilson, Aiyana Ooki-Knutson, and Jennifer Conley
Abstract: In June 2024, Providence St Joseph Health updated the standard gentamicin dose in the Pediatric and Neonatal Aminoglycoside protocol from 4 mg/kg to 5 mg/kg every 24 hours for late preterm and term neonates. This project aims to evaluate late preterm and term neonatal patients who received gentamicin for empiric sepsis coverage within the first seven days of life, at 4 mg/kg/dose or 5 mg/kg/dose, to assess the safety of the standardized 5 mg/kg dosing for late preterm and term neonates after the protocol change. This study is a multicenter retrospective pre-/post-intervention analysis at a multistate health system spanning 51 hospitals. Term neonatal patients who received either 4 mg/kg/dose every 24 hours or 5 mg/kg/dose every 24 hours for empiric sepsis will be included. Further inclusion criteria include receipt of at least one dose of gentamicin, gestational age of at least 35 weeks, and delivery at a hospital within the Providence St Joseph Health system. The pre-intervention group will include patients who meet inclusion criteria that were born from October 1, 2022, through September 30, 2023, while the post-intervention group will include qualifying patients born from October 1, 2024 to September 30, 2025. Primary endpoints include urine output and urine occurrences per 24 hours for a 4-day period following the first dose of gentamicin. Secondly, endpoints include daily serum creatinine values when available and duration of gentamicin dosing. Serum gentamicin levels are not routinely collected in this patient population, as duration of therapy is often limited, and standard practice is to avoid drawing blood when not entirely necessary. For patients who received gentamicin long enough to warrant drawing a trough and/or peak, a subgroup analysis will be performed to evaluate if the higher dosing regimen resulted in significantly higher levels. This will be evaluated not only based on numeric serum concentration values reported but also based on the incidence of sub- and supra-therapeutic levels. Descriptive statistics will be used to describe the baseline characteristics of the study population. A p-value of less than 0.05 will be considered statistically significant. Results and Conclusions will be reported and shared when the project is complete. (IRB approved) Learning Objectives: Describe the difficulties of gentamicin dosing in late preterm and term neonates. Evaluate the safety of gentamicin when dosed at 4 mg/kg/dose vs 5 mg/kg/dose for late preterm and term neonates. Presentation Category: Pediatrics and Neonates
-
Lemierre Syndrome: From Scalp to Cerebrum
Jack Hildenbrand, MD and Brinton Clark, MD
Background: Lemierre syndrome is a rare but severe infection, most commonly caused by Fusobacterium species originating from head and neck sources. Intracranial complications occur in only 11% of cases and are particularly uncommon in the absence of internal jugular vein thrombosis or endocarditis. Case Presentation: A 32-year-old previously healthy woman was admitted with sepsis due to Fusobacterium necrophorum bacteremia. Three weeks earlier, she had been hospitalized for sore throat and community-acquired pneumonia; blood and bronchoscopy cultures were negative, and she was discharged on amoxicillin-clavulanate. On readmission, blood cultures were positive for Fusobacterium necrophorum and evaluation revealed a right parietal scalp abscess, which was surgically drained. Transthoracic e chocardiography showed no valvular vegetations, and CT imaging revealed no thrombosis or thrombophlebitis of the head or neck. She was treated with ceftriaxone and metronidazole and discharged in stable condition on oral antimicrobials. Two days later, she re-presented with acute left-sided sensory changes and weakness. Neuroimaging demonstrated a right frontoparietal brain abscess and parietal meningitis with thrombosis of the right calvarial subarachnoid veins. She underwent craniectomy and surgical evacuation of the brain abscess, followed by four weeks of intravenous antibiotics. Despite aggressive management, she was left with partial left-sided hemiparesis and required inpatient rehabilitation for significant functional deficits. Discussion: Lemierre syndrome classically presents as oropharyngeal infection with subsequent septic thrombophlebitis. This case is notable for its atypical progression: likely unrecognized Fusobacterium pneumonia, followed by bacteremia, extracranial scalp abscess, and ultimately contiguous intracranial abscess with hemiparesis, despite timely source control and appropriate antibiotics. In the largest series of over 700 Lemierre syndrome cases, 17% developed early complications after diagnosis and treatment, with 3.8% developing septic intracranial lesions. In this patient, the brain abscess was contiguous with the scalp abscess, suggesting spread via emissary veins connecting scalp veins to the dural venous sinuses. Multiple imaging studies failed to demonstrate internal jugular vein thrombosis, but thrombosis of subarachnoid veins near the abscess was identified, supporting local contiguous spread. This case underscores the persistence and severity of Fusobacterium infections and highlights the risk of serious complications despite aggressive therapy. It emphasizes the need for vigilance, follow-up imaging, and consideration of prolonged therapy in Fusobacterium bacteremia. Conclusion: Clinicians should maintain a high index of suspicion for intracranial extension in patients with Fusobacterium bacteremia, even in the absence of classic findings such as endocarditis or internal jugular vein thrombosis. Early recognition, aggressive management, and appropriate antimicrobial duration are essential to mitigate neurologic morbidity.
-

Enhancing Gestational Diabetes Screening
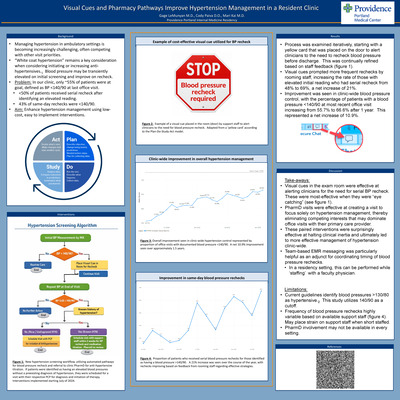
Sataj Johnson and Daniel Ruegg
Background: Gestational diabetes mellitus (GDM) screening is recommended between 24–28 weeks of gestation to allow timely diagnosis and treatment and reduce adverse maternal and neonatal outcomes. The two-step glucose tolerance testing method is supported by ACOG, though completion can be delayed due to the need for multiple tests. In 2024 at Providence Milwaukie Family Medicine Clinic, incomplete GDM screening occurred in 23.1% of patients, and incomplete two-step screening occurred in 33.3%, with an average completion time of 12 days. Objective: To increase completion rates of two-step GDM screening and reduce time between abnormal 1-hour and diagnostic 3-hour glucose tolerance tests by offering clinic-based testing instead of lab-only screening. Methods: Clinic-based screening was implemented by obtaining supplies and establishing a workflow. Outcomes were evaluated through chart review and data collection. Results: Prior to implementation, the two-step screening completion rate was 70%, with an average completion time of 15 days. From March 2025 to February 2026, completion increased to 81%, with 72.7% completed in clinic and 9% in the lab. Non-completion decreased to 18%. Average completion time improved to 11 days. Conclusion: GDM affects approximately 1 in 11 pregnancies in the United States and can lead to significant maternal and neonatal complications if untreated. Clinic-based screening modestly improved completion rates and reduced time to diagnostic testing. Patients reported the clinic option as convenient. Expanding clinic-based screening may improve access, patient satisfaction, and timely diagnosis, particularly in settings with limited laboratory access. Larger studies are needed to assess statistical significance and long-term obstetric and neonatal outcomes.
-

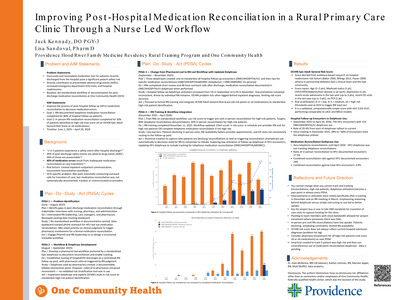
Improving Post-Hospital Medication Reconciliation in a Rural Primary Care Clinic Through an RN-Led Workflow
Jack Kennady
Context/background: Adverse events after hospital discharge are common and represent a major patient safety concern. Approximately 1 in 5 patients experience a safety event after discharge, and 39% of these events are adverse drug events (ADEs), with 26% considered preventable. Medication discrepancies during transitions of care contribute significantly to these events, with an estimated 40% of medication errors resulting from inadequate medication reconciliation. Rural primary care clinics face additional challenges, including limited communication between inpatient and outpatient systems and inconsistent reconciliation workflows. Improving medication reconciliation during the transition from hospital discharge to outpatient follow-up represents an important opportunity for family medicine practices to reduce preventable ADEs. Objective: To implement and evaluate a standardized RN-led workflow to improve medication reconciliation for patients discharged from the hospital and presenting for follow-up at One Community Health. Project goals included completion of telephone medication reconciliation for 80% of hospital follow-up patients and in-person RN medication reconciliation visits for 50% of patients identified as high risk. Methods: Quality improvement project conducted at One Community Health in Hood River, Oregon using sequential Plan-Do-Study-Act (PDSA) cycles from June 2025 to June 2026. • PDSA 1 (June–Aug 2025): Problem identification; stakeholder interviews (nursing leadership, care managers, pharmacists, administrators). Baseline: no standardized workflow or documentation for post-discharge medication reconciliation. • PDSA 2 (Aug–Sept 2025): Workflow design; development of standardized EHR dotphrase to document medication reconciliation and enable tracking. • PDSA 3 (Sept–Nov 2025): Implementation of documentation intervention. Hospital discharges (ED and inpatient) routed to a centralized follow-up pool. RN chart review and outreach calls within 48 hours; medication list review and reconciliation documented using dotphrase. • PDSA 4 (Dec 2025–Mar 2026): RN training and workflow integration. Standardized reconciliation during outreach calls and prior to follow-up visits scheduled within 7–14 days. • Next cycle: Audit outcomes, identify barriers, refine workflow to improve reconciliation rates toward target goals. • Data sources: EHR dotphrase utilization and hospital follow-up encounter chart review Results: Between September 2025 and February 2026, 462 hospital follow-up visits were identified. RN-led medication reconciliation documentation occurred in 100 encounters (21.6%). After dotphrase implementation in September, reconciliation rates increased from 1.6% in September to 13.6% in November. Following RN workflow training in December, telephone reconciliation documentation increased to 71.7% of follow-up visits that month and 54.4% in January. Further manual data analysis will be performed at the end of March and June to determine how many telephone medication reconciliations were completed and how many high risk patients had completed medication reconciliations in-person with RN prior to provider appointments. Discussion/conclusions: Medication discrepancies during care transitions are a major contributor to preventable ADEs in primary care. Implementation of a standardized RN-led medication reconciliation workflow improved the clinic’s ability to identify recently discharged patients and document reconciliation prior to follow-up visits. Early findings suggest nursing-led interventions and standardized EHR tools can strengthen transitional care processes in rural family medicine practices. Continued evaluation will assess how best to implement medication reconciliations in a team-based setting
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}