
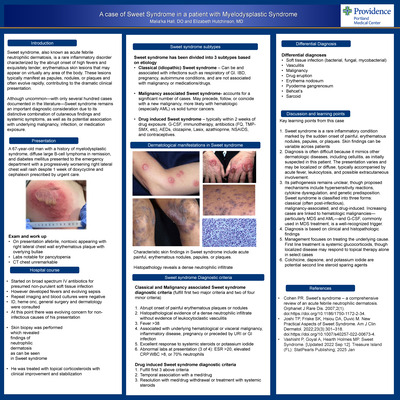
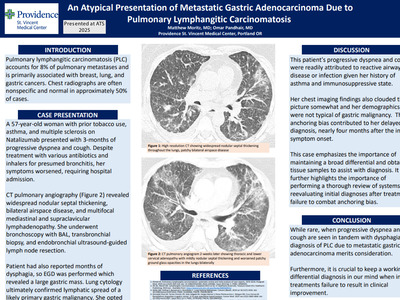
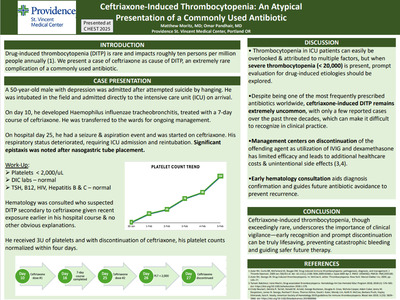
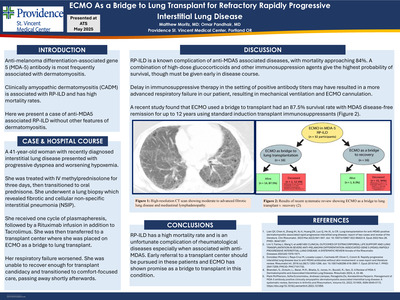
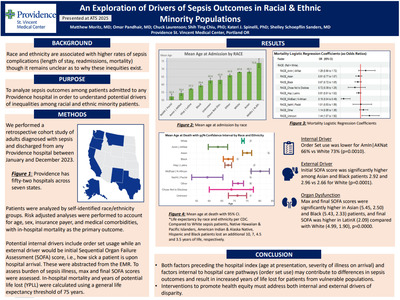
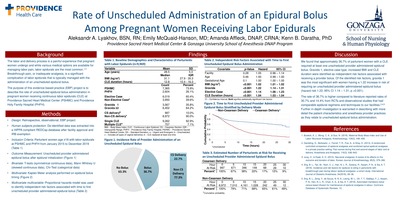
-

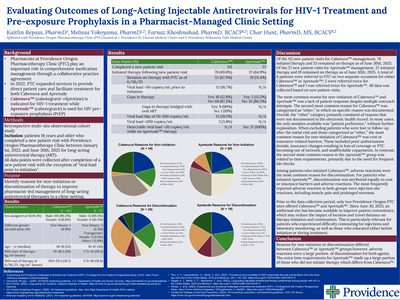
Sugammadex versus Neostigmine: Operating Room Time and Cost
Annie Benscheidt and Kenn B Daratha
Background The choice of neuromuscular blockade reversal agents impacts cost and operating room time. Currently, the two medications used to reverse neuromuscular blockade are Neostigmine and Sugammadex. These medications differ in both cost and pharmacologic profiles which effect the time and predictability of reversal (Carron, Zarantonello, Tellaroli, & Ori, 2016). Evaluating cost and time differences in reversal using Sugammadex and Neostigmine helps anesthesia providers select the appropriate medication. This evidence based practice project examined the difference in case length and operating room and reversal agent costs in cases using Sugammadex and Neostigmine at Providence Sacred Heart Medical Center.
Methods • Retrospective, observational, evidence-based practice project • Facility approved and IRB exemption determination granted • Extracted case data deidentified and securely extracted into a HIPPA compliant REDCap database • 11,944 cases evaluated from January 1, 2015 to December 31, 2018 • Inclusion criteria: ASA rating I, II, III; age <70; BMI <40; no diagnosed reduced pulmonary reserve conditions; no diagnosed pre-existing neuromuscular disease • Cases removed: Surgical case duration not calculated; Neostigmine units <1 mg; Neostigmine units >5 mg; Sugammadex units >1000 mg; Sugammadex units <50 >mg; Neither Neostigmine and Sugammadex used; Neostigmine and Sugammadex both used; Neostigmine given without Glycopyrrolate; Surgical procedures labeled ‘50’ • Analytical plan: Categorical variables described by frequency distributions; skewed continuous variables described by median and interquartile range. Average medication costs, operating rooms minutes, and estimated operating room costs/case reported by reversal agent. • Simulation: Total operating room and reversal agent costs were projected using an estimated operating room rate. Sensitivity analysis was completed in which the estimated operating room rate was varied.
Discussion Operating room (OR) time and cost of neuromuscular blockade reversal agents were compared among cases in which either reversal agent could be used. The average reversal agent cost per case using Sugammadex was $99.13 compared to cases using Neostigmine/Glycopyrrolate at $32.55 per case. A side by side comparison between Sugammadex and Neostigmine for like surgeries found that Sugammadex shortened surgical case duration for most procedures. Across all project cases the average surgical case duration for cases reversed using Sugammadex was 150 minutes (estimated operating room costs $14,623 per case). Neostigmine reversed cases averaged 153 minutes for surgical case duration (estimated operating rooms costs $14,901 per case). In simulated models, exclusive use of Sugammadex across all cases for the past four years would have resulted in cost savings across a range of estimated OR costs per minute. The findings of this observational project showed an average of about three minutes were saved in OR time when using Sugammadex versus Neostigmine. Surgical case duration is complex and multi-factorial. The results of this observational project signal a difference in OR time and agent costs as the result of reversal agent choice. Further randomized investigations are warranted.
-

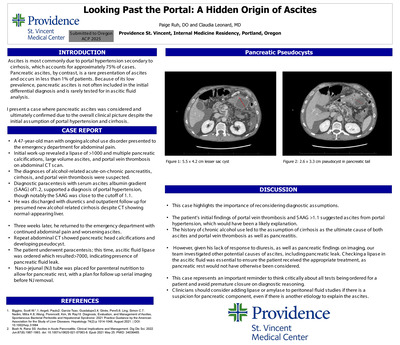
Increase in Video Evaluations but Not Complications Over Time in a Large Stroke Network
Archit Bhatt, Elizabeth Baraban, Leslie Corless, and Lindsay Lucas
Introduction: Telestroke technology allows evaluation of stroke patients remotely. We sought to determine if there was any change in the standard of care and evaluation of stroke patients over time and whether there were differences in complication rates between those who were evaluated using telestroke technology and those who were not.
Methods: Data from April 2010 to May 2018 from a large stroke network were used. Acute ischemic stroke patients who presented to the emergency departments (ED) with last-known-well-to-door less than 4.5 hours and were treated with IV-alteplase were included. The number of facilities ranged from 7 in 2010 to 18 in 2017. Primary outcomes included the number and percentage of cases that were treated using telepresence (Beam-In) versus conventional care (no Beam-In) over time, as well as their discharge status and complications. Chi-squared or Linear By Linear Association were used to compare categorical variables and Mann-Whitney U Tests were used to compare continuous variables.
Results: A total of 1,150 patients were treated from 2010 to 2018, 75.8 % (n=872) via Beam-In. The number of Beam-Ins increased overtime and there was a significant increased trend in the percentage of treated Beam-Ins (p<.001) (graph). There were fewer patients discharged home (38.0% vs 50.4%, p<.001), more transferred to acute care facilities (37.6% vs 13.8%, p<.001) and fewer hospice or deaths (5.9% vs 12.9%, p<.001) for those treated via Beam-In. There was no significant difference in number of symptomatic intracranial hemorrhage, life threatening systemic hemorrhage or other serious complications.
Conclusion: Stroke care has evolved from traditional bedside care to more video evaluations in patients who received alteplase without increase in complications.
-

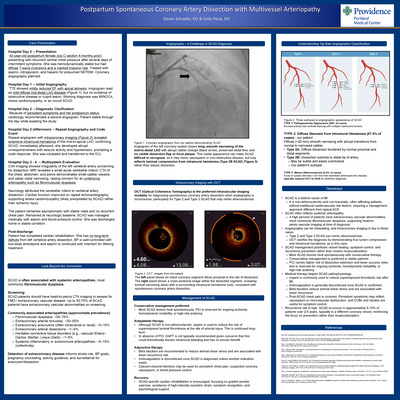
Ultrasound Simulation for Regional Anesthesia
Kayla Brown and Kenn B Daratha
Background Regional anesthesia is an essential skill in the practice of Nurse Anesthesia, and future employment demands expertise. Literature supports the addition of simulation training to existing didactic and apprenticeship education to improve clinical expertise. The purpose of this project was to trial simulation training, focused on anatomical visualization with ultrasound for regional anesthesia, as a means to improve student performance and confidence.
Methods • Facility project approval and exemption determination by IRB. • Hands-On Test: Ultrasound to obtain visualization for axillary (cohort 1), interscalene (cohort 2) block on live-model. Expert CRNA observed performance to determine if image was clinically acceptable. Yes/No result, and time necessary for visualization recorded. • Written Test: Anatomical structures to be named, (fig. 1). • Expert led practice with visualization for interscalene, supraclavicular, axillary, TAP, adductor canal, popliteal and IPACK blocks. • Testing repeated after completion of training.
Discussion Student performance in ultrasound demonstration and written anatomy identification improved after implementation of expert-led ultrasound training and simulation practice. Survey results demonstrated improvements in perceived confidence with the use of ultrasound following simulation training. Clinically significant improvement as demonstrated by this educational innovation project, provides a compelling statement to the University; additional simulation training should be integrated into the curriculum. Furthermore, this project opens dialogue about purchasing an ultrasound machine dedicated to the Nurse Anesthesia program.
-

Ibuprofen Does Not Increase Blood Pressure in Preeclampsia
Sofia Costas, Sherry Hutton, and Cindy Kenyon
Objective: The aim of this IRB approved study was to evaluate the impact of ibuprofen on Mean Arterial Pressure (MAP) in the immediate postpartum period of women with preeclampsia.
Design: A retrospective chart audit of 633 preeclampsia patients who had treated severe hypertension (BP > 160/105) during their hospital stay.
Setting: Metropolitan Level 3 facility in Portland OR.
Patients/Participants: 169 patients met criteria; received magnesium sulfate postpartum and had severe hypertension postpartum. 60 were randomly selected, 30 received ibuprofen, 30 did not.
Methods: Baseline was obtained at 2 hours postpartum. Each patients MAP for each 24 hour interval were averaged. The Mean arterial pressures (MAP) were compared in women who received Ibuprofen versus those who did not. MAPs of the two groups of patients were then compared at the following intervals: 24, 48, 72 and 96 hours and compared using t-tests to determine statistical significance.
Results: When comparing the average overall MAP pressures between the two groups of patients, there was no significant difference. In other words there was no statistically significant difference in average blood pressure at the following time intervals: 2 to 24 (p=0.46), 24 to 48 (p=0.56), 48 to 72 (p=0.45), 72 to 96 (p=0.49) Average total hours (p=0.48)
Implications for nursing practice: Our data collection results revealed that there was not a significant increase in MAP for Preeclamptic patients who received Ibuprofen in the postpartum period which is consistent with the current literature. Based on this finding, Ibuprofen following birth should be included in the pain control plan in hopes to reduce narcotic use and dependence
-

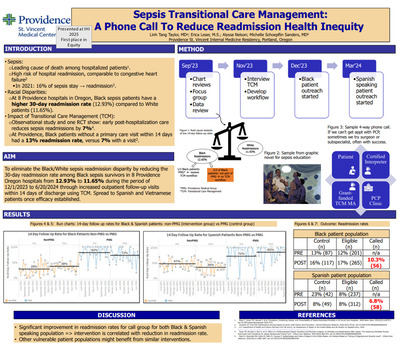
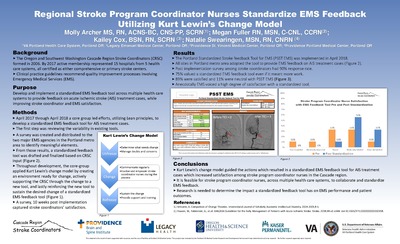
Standardized Code Stroke Inpatient Activation Process Resulted in Consistent Acute Stroke Evaluation Times Regardless of Primary Problem or Patient Location
Kailey Cox, Brandon Sheets, Alyx Lesko, Lindsay Lucas, Elizabeth Baraban, Ronda Chandler, and Diane Clark
Introduction: Inpatient strokes have a higher mortality risk and longer length of stay compared to community-onset strokes. The inpatient stroke population is often not included in national registries. This study examines a hospital-wide standardized process for acute triage of Code Stroke Inpatient Activations (CSIAs) at a Comprehensive Stroke Center.
Methods: CSIA data collected between September 2016-July 2018 from the Stroke and Rapid Response Team pager were used. False CSIAs were excluded. Outcomes included percentage of CSIAs by patient location (PL), primary problem (PP), and final discharge diagnosis (FDD), as well as percentage treated with IV-alteplase (tPA) and thrombectomy. Evaluation times of symptom discovery-to-stroke MD page (Sx-SMDP), symptom discovery-to-CT (Sx-CT), stroke MD page time-to-CT (SMDP-CT) were compared across PP and PL using one-way analysis of variance for log-transformed time with pairwise comparisons. Among CSIAs with a new stroke diagnosis at discharge, the percentage found in our Comprehensive Stroke Registry (CSR) was identified.
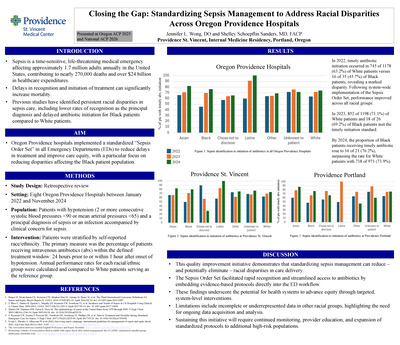
Results: Among all CSIAs (n=99), 47.1% (n=41) of patients were admitted for cardiac, post cardiac surgery or TAVR; 19.5% (n=17) for stroke; and 33.3% (n=29) for other PP. Among 79 CSIAs with PL, 30.4% (n=24) were in cardiac units, 24.1% (n=19) in stroke units, 21.5% (n=17) in non-stroke/non-cardiac units, 17.7% (n=14) in peri-procedural units and 6.3% (n=5) in the observation unit. Among 72 CSIAs with FDD, 72.2% (n=52) had a new stroke diagnosis whereas 27.8% (n=20) did not. Overall treatment rate was 6.0% with median Sx-tPA of 68 minutes (n=2) and median Sx-GP of 147 minutes (n=4). No differences in Sx-SMDP, Sx-CT, or SMDP-CT by PL or PP were found. Among 52 CSIAs with stroke FDD, 21.2% (n=11) were identified as inpatient strokes at discharge in our CSR.
Conclusions: Standardized Code Stroke Inpatient Activation process resulted in consistent evaluation times regardless of primary problem or patient location. Code Stroke Inpatient Activations in the cardiac population need further examination and may reflect the presence of comprehensive cardiac surgical services at this hospital. National stroke registries do not reflect the size or full spectrum of the inpatient stroke population.
-
 Delawska-Elliott, Helene Anderson, and Marla London")
The Force of Magnetism: Nursing-Library Collaborations to Support Magnet
Barbara (Basia) Delawska-Elliott, Helene Anderson, and Marla London
Background: The ANCC Magnet model is built on 5 Model Components and 14 Forces of Magnetism. The Components and Forces, including Transformational Leadership, Structural Empowerment, Exemplary Professional Practice, New Knowledge, Innovation & Improvement, and Empirical Quality Results (Models), and Professional Development, Quality Improvement, Nurses as Teachers, and Quality of Care (Forces) encourage and recognize professional growth, care improvement, and knowledge dissemination. Familiarity with searching professional literature and information literacy are key skills needed to grow Magnetism. This presentation will describe a collaboration between Magnet leadership and the library to build programs designed to support Magnet values and outcomes.
Description: Magnet leadership at a four-time Magnet-designated hospital approached the library with a proposal for an evidence-based program pilot. The librarian’s role in the pilot was co-developing the instructional module introducing EBP, searching the literature and evidence appraisal, and hands-on small group search training with a PhD-prepared nurse. The program was launched in 2015 and post-program analysis showed improved understanding of the EBP process and higher information literacy confidence. Building on the success, the following year the interdisciplinary team consisting of hospital magnet leadership, nursing research leadership, and the librarian added a nursing research program.
The ongoing educational programs were named best practice by ANCC Magnet appraisers and the program projects were cited in the Magnet documentation. Following appraiser evaluation, to address the need to disseminate knowledge externally, this year the hospital is launching a program helping nurses publish.Conclusion: The program started as an instructional venture introducing the concepts of evidence-based practice and nursing research to hospital staff nurses. Since its inception, 6 projects have led to practice change, 3 have been presented at conferences, one is being written up for publication. Some projects evolved from evidence-based to research questions and from smaller to larger studies in different hospital settings. Many original program participants have continued with the program or have developed independent research studies. The success of this collaborative program lies not only in renewed Magnet designation, but also by nurse engagement in practice change and nursing research.
-

Institutional Repository Workflow, Project Management, and Outreach in a Remote/Online Library Environment
Daina Dickman
In 2018 Providence St. Joseph Health launched an institutional repository, primarily staffed by a librarian located in Oregon and a library assistant located in Montana with occasional help from other Library Services staff. Workflow and communication standards had to be created that would allow library staff in multiple locations and time zones to seamlessly launch, populate, and manage the institutional repository. Outreach, instruction, and promotion tactics had to also be created to reach researchers and clinical staff across six states and 100+ locations.
-

Social Justice and Medical Library Institutional Repositories: Tactics and Outreach
Daina Dickman
Objective: This paper discusses the experiences of an institutional repository (IR) manager at a multi-state health system. Launched in 2018 the IR aims to gather published articles, presentations, posters, etc. produced across the 50+ hospitals in the system. Since the IR is new, there is the opportunity to build social justice and critical librarianship in to the strategic planning from the beginning.
Methods: How can a social justice lens inform what is added to an IR? If an IR aims to collect the entire body of research at an institution what steps can be taken to make sure works promoting diversity, equity, and inclusion (both authors and subject matter) are being found? What happens to the work of colleagues at our rural clinics versus the work of colleagues at well-funded research institutes who have the resources to publish articles?
Targeted outreach efforts undertaken to promote equity and representation will be examined, including successes and failures. Outreach at an individual author level, organizational departments, and employee affinity groups will be discussed. While PubMed searches capture most articles for inclusion, outreach and awareness is the main tactic to collect gray literature.
Results: Without targeted outreach efforts and a social justice framework an IR will not provide representation, equity, and inclusion. Having these as part of the launch and strategic planning for the IR creates the space to devote staff time and energy and sees it as an intrinsic goal in the IR.
Conclusions: There are no absolute conclusions, as this is an ongoing approach to medical library IR management and designed to open a conversation. Time will be included for an interactive think-pair share activity. Participants will be invited to brainstorm ideas to incorporate social justice in to medical library institutional repositories and to share experiences from their own institutions.
-

Organizing Your Organization: Taxonomy and Organizational Schemes in a Health System Institutional Repository
Daina Dickman and Heather J. Martin
Background: In the development of a new institutional repository, library staff at a large health system were faced with building an organizational structure that would be meaningful to both internal and external users. The health system context meant unique challenges designing a taxonomy that supported end users as well as institutional goals and branding. Health systems have unique user needs for specialized collections and organizational schemes. With a comparatively large volume of items being added there are also concerns with the backend structures to accommodate the institutions’ large research output.
Description: This large, recently merged health system did not already have a predefined structure or taxonomy by which to organize or make collections browsable. Complex institutions without clearly set “Departments” will be interested to hear how library staff created and implemented an organizational structure and taxonomy for their institutional repository. By considering existing classification schemes, internal naming practices, and consulting small stakeholder focus groups publications are now easily browsable by both internal and potential external users.
Additional organizational structures were created to house collections in support of institutional goals. One of the debut specialized collections focuses on nursing evidence-based practice, and was leveraged as documentation during a recent Magnet re-certification.
Tactics for creating back end organizational structures that support large volumes of items is also an area being explored in the first year of their institutional repository.
Conclusion: The institutional repository launched in 2018 with a taxonomy and organizational structure developed for the health system. The library continues to solicit feedback from stakeholders for improvements and ideas to serve internal and external users. Currently, different backend organizational structures are being tested in support of the large volume of items entered on a monthly basis in the institutional repository. -
 Among Nurses, Nursing Assistants, and Unit Secretaries by Kim Dimaunahan, Sandy Martir, Amber Norman, and Trisha Saul")
Knowledge, Attitudes, and use of Complementary and Alternative Medicine (CAM) Among Nurses, Nursing Assistants, and Unit Secretaries
Kim Dimaunahan, Sandy Martir, Amber Norman, and Trisha Saul
-

Conversations Matter: Initiating a Serious Illness Conversation
Matthew J Gonzales and Suzanne Engelder
-

Using REDCap to Collect Library Service Statistics in a Large Health System
Carrie Grinstead
Background: In January 2018, library services at Providence Health/Swedish and St. Joseph Health merged to form a single, unified system, incorporating nine libraries and sixteen full-time staff. We faced several challenges in collecting and reporting service statistics, including the disparate methods of our legacy organizations, the variation in services offered at different libraries, and our large geographic spread. Our merged library serves patrons in seven states, and much of our work, including communication with patrons and each other, is conducted over email.
Description: We chose a tool, REDCap, early in our process. REDCap is easy to use and allowed us to build a web form that would be accessible on site and off, and regardless of legacy organization. REDCap allows for quick and easy reporting, facilitating our annual infographic and allowing us, for the first time, to produce monthly usage reports.
One librarian compiled a list of items that had been tracked at each hospital library. We then convened a small task force to decide what information we would collect and at what level of detail. This group included representatives each legacy organization. We considered issues such as accurate representation of the various services performed at each site and usefulness for reporting out. We then built a sample form and invited all team members to test it for one month.Conclusion: Our REDCap form for statistics collection went live on April 1, 2018. The form is simple to use, and REDCap’s branching logic functions allow us to collect detailed information without making the form unwieldy. Occasional communication and retraining for our team has been necessary, to ensure that fields in the form are understood and used consistently. Finally, we are using our reports to assess and further refine the form for 2019. Some fields, such as the purpose of a request, are rarely used and may be eliminated, while new fields may be added in consultation with the team.
-

Nurses’ Experiences and Perceptions of Using Online Resources for Patient and Family Education: A Qualitative Interview Study
Carrie Grinstead, Sarah Sumner, Julius Shakari, and Martha Inofuentes
-

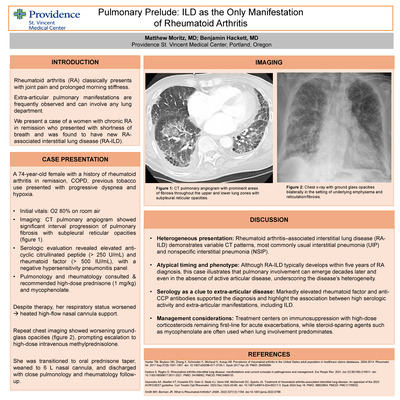
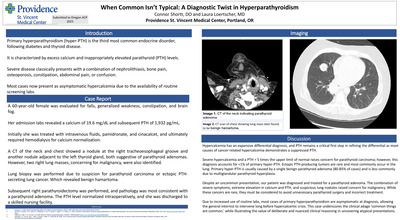
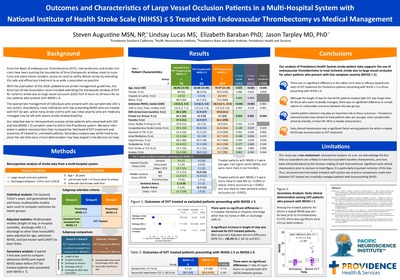
Hyperoxia: Current Practice of Oxygen Delivery During General Anesthesia
Christa Kirby and Kenn B Daratha
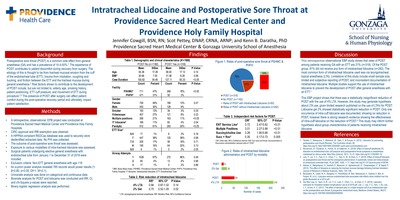
Background While supplemental oxygen is routinely administered during anesthesia to prevent oxygen desaturation and optimize tissue oxygenation, oxygen delivery practices after intubation are largely unknown. Compiled evidence suggests limiting intraoperative fraction of inspired oxygen (FiO2) to below 60%. The deleterious effects of hyperoxia and the mortality benefit of conservative oxygen administration are being demonstrated in contemporary critical care literature. The lack of consensus guidelines and high level evidence on the topic of intraoperative oxygen delivery begs the question to what degree are patients being exposed to hyperoxia during general anesthesia. The purpose of this evidence-based practice project was to better understand oxygen administration practices during general anesthesia and assess independent risk factors for hyperoxia for patients at Providence Sacred Heart Medical Center.
Methods A comprehensive literature review was conducted • Institutional approval and IRB exemption determination granted • Relevant de-identified patient data was extracted from electronic health record • Encrypted data was stored in a HIPAA compliant REDCap database • Inclusion criteria: Adults 18 years of age or older who received general anesthesia at PHSMC during 2018 • Patients must have been intubated with an ETT or LMA and extubated at the end of the case • Additional exclusion criteria: ENT, thoracic, cardiac, pulmonary service lines and emergent procedures • Median FiO2 and SpO2 from intubation to extubation were measured and analyzed • Binary logistic regression analyzed the independent effects of hyperoxia (median FiO2 in excess of 60% while under anesthesia) • Level of significance set to 0.05
Discussion Of the cases reviewed for this project, 39% of the patients were exposed to median FiO2 in excess of 60% during anesthesia. Median FiO2 from intubation to extubation largely fell between 50% and 70% and SpO2 averaged 99%. Independent risk factors for median FiO2 in excess of 60% included higher ASA status, increasing age, and female gender. Case duration was inversely independently related. No effects were observed from smoking, COPD or BMI. Further studies are needed to evaluate the implications of oxygen exposure during general anesthesia and the safety and feasibility of more conservative intraoperative oxygen administration. The emerging evidence will likely prompt providers to be more mindful of oxygen delivery practices during anesthesia.
-

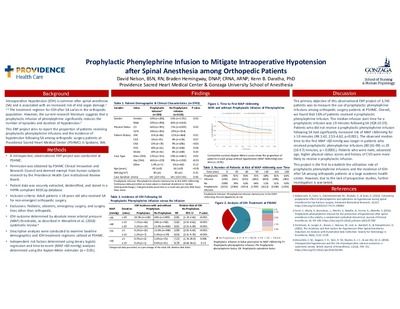
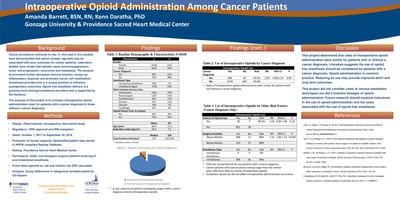
Intraoperative Hypotension in Non-Cardiac Surgery Patients at Providence Sacred Heart Medical Center
Genna LeDrew and Kenn B Daratha
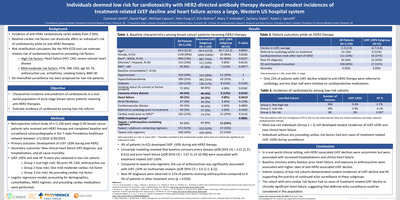
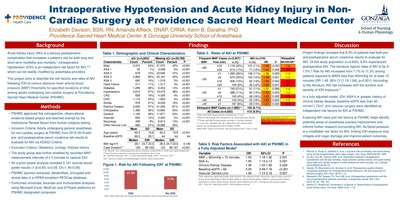
Background Intraoperative Hypotension (IOH) during non-cardiac surgery is a common side effect of anesthesia that is associated with acute kidney injury (AKI), myocardial injury (MI), mortality, and other adverse outcomes1,3,4. These risks increase as the duration and severity of IOH exposure increase3,4. Blood pressure is a modifiable risk factor of mortality and organ damage that can be readily treated by the anesthesia provider2 . Limiting IOH can improve patient outcomes and produce monetary savings5 . The objective of this project is to report the incidence of IOH at a large tertiary teaching hospital, and extrapolate the risks of mortality and organ damage among patients with IOH. This project also identifies IOH risk factors, and reports timing of IOH during surgery.
Methods We conducted a retrospective analysis of secondary, observational data at Providence Sacred Heart Medical Center (PSHMC) • Eligibility Criteria. Inclusion: patients >18 years of age who received general anesthesia for elective non cardiac surgery from October 1, 2017 to September 30, 2018 Exclusion: cardiopulmonary bypass, emergent, cesarean & pediatric surgical populations; persons with blood pressure frequency >5 minutes • Patient demographic and surgical data from electronic medical records were extracted using a REDCap data collection tool • We defined IOH according to absolute mean arterial pressure thresholds described by Wesselink et al., 20184 • Descriptive analyses were conducted to examine baseline demographics, incidence and timing of IOH in the study population • Multivariable analyses using binary logistic regression were performed to examine risk factors associated with IOH ( = 0.5) • The risks of mortality, AKI & MI associated with each IOH definition were extrapolated based upon data from a 2018 systematic review4 • This project was approved by the PSHMC Clinical Innovation and Research Council, and deemed exempt from human subjects research by Providence Health Care institutional review board
Discussion At a large tertiary teaching hospital, we found that 24% of our study population experienced IOH associated > 50% increased risk of MI, while 8% and 6% of patients experienced IOH associated with a >2 times greater risk for AKI and mortality, respectively. Female sex, longer case duration, and interventional radiology, cardiology, and plastics service lines were among the top IOH risk factors. 42% of IOH occurred between anesthesia induction and surgical incision, even though that time period only accounted for 19% of the intraoperative time. These findings suggest that up to one-quarter of non-cardiac surgical patients may be at elevated risk for organ damage, and as much as 6% patients may double their risk of mortality due to IOH. Given these risks, anesthesia providers should minimize IOH, and be aware of patient and surgical characteristics associated with higher IOH risk. The period between anesthesia induction and surgical incision may represent a time in which the anesthesia providers can work independently to reduce IOH exposure. Future projects should examine the utility of strategies for anesthesia providers to reduce IOH exposure in patients undergoing noncardiac surgery and reassess incidence rates.
-

Using AI and NLP to Alleviate Physician Burnout
Aaron Martin
Artificial Intelligence (AI) is widely recognized as a powerful tool with potential for many healthcare applications. One application gaining interest is using AI to help solve physician burnout – the state of disillusionment among doctors tired of repetitive data entry tasks, as well as administrative duties, and excessive time spent combing through patient data. In this session, one of healthcare’s top innovators will examine how the power of AI, when merged with natural language processing (NLP), can alleviate many physician burnout woes.
Aaron Martin, a former executive leader and innovator at Amazon before he moved to healthcare, will take a realistic approach, recognizing that “the next big thing” will still require time, focus, and collaboration to get it right. However, with a solid AI and NLP strategy, physician burnout – as well as better patient service, improved outcomes, and more – can all be addressed. -

The Goldilocks Method: Demonstrating Your Value in Small, Medium, and Large Bites
Heather J. Martin
Background: In an era of financial constraint hospital libraries are facing closer scrutiny and must prove their value in order to survive. Leadership at a large health system library found the traditional written annual report lacked the impact needed to capture the attention and the imagination of administration. Taking different approaches over the years, this library has found a solution that is “just right”, creating three very different documents – small, medium, and large – to demonstrate its worth.
Description: Library leadership moved away from the traditional written annual report toward a one-page infographic that depicted the library’s scope, scale, and impact. This visual representation of library statistics captured the attention of administration and patrons in a new, compelling way. As it didn’t allow for telling deeper stories of special projects and partnerships, the library later added back in a written supplement and a “Selected Thanks” section that directly quoted satisfied library patrons. But, when the library’s very existence was at stake, the need for a much more comprehensive value-case was necessary, and a 20-page white paper tied to the organization’s strategic plan and key initiatives was created. Providing an annual report in 3 different formats – small, medium, and large, allows the library to tell just the right story, to the right person, in the right place.
Conclusion: Reporting on library usage statistics, initiatives, and successes in different formats has allowed the health system library to tell its story in just the right way at the right time. The posted infographic provides a lasting snapshot that draws people in. As such, it has been viewed by far more people than reports in the past. The written supplement tells stories from our patrons, and is delivered to key leadership. The value-case effectively tied ALL the work the library does directly to the institution’s strategic goals, and this past year effectively convinced senior leadership to stave off cuts.
-
 Delawska-Elliott, and Daina Dickman")
Building a Health System Institutional Repository: Setting Yourself Up for Success from the Start
Heather J. Martin, Barbara (Basia) Delawska-Elliott, and Daina Dickman
Background: While more common in university settings, institutional repositories (IR) have a place within hospitals and healthcare systems too, though the challenges in creating them may be different. This paper looks at the development of a Digital Commons institutional repository at Providence St. Joseph Health. The authors present the necessary steps for a successful initiative beginning with the planning process and building from there. Highlighted are some of the different challenges faced in non-academic settings; considerations when selecting a platform and designing and structure; and recommendations for doing outreach and promotion to unique user groups.
Description: Library staff proactively followed trends in IRs and prepared for future state. Identifying technology requirements and platform options, exploring other health system IRs, and building a search algorithm to capture the affiliations within a newly merged enterprise meant that when approached by senior leadership about publication tracking the library was well positioned for success. Library staff selected a platform, determined the repository’s scope, and identified key stakeholders. An implementation plan included securing funding and executive support, hiring a librarian, and developing a framework for year 1 of the project. A complex organization presented unique challenges when designing a metadata and taxonomy structure. Getting buy-in from clinicians required a strong elevator pitch, and a direct tie to the organization’s strategic goals. Anticipating organizational needs meant a platform able to accommodate datasets, visual collections, Magnet documentation, and locally-published peer-reviewed journals
Conclusion: Digital Commons launched in July 2018, and within 3 months was populated with 700+ publications and included profiles from several world-renowned researchers. A successful Year 1 is on track and will be measured by hitting a publication target of 1000 and successfully importing all 2018 affiliated publications from PubMed. Library staff is now focused on marketing and outreach, with the intention to rapidly grow the Expert Gallery to include individuals from a diverse representation of disciplines and health system markets, increase submission of non-periodical scholarly activity, and to form collaborative partnerships for growth into new areas like datasets, and video.
-

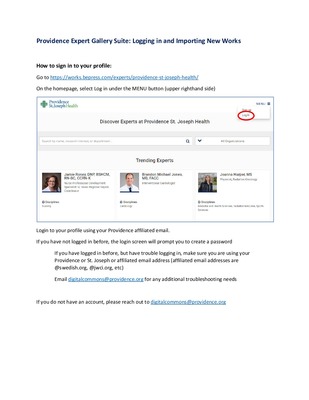
Managing Researcher Expectations: Defining the Scope of Your Expert Gallery
Heather J. Martin and Daina Dickman
This presentation explains Providence St. Joseph Health's experiences in creating researcher/author profiles in the Expert Gallery of Digital Commons, their institutional repository. It discusses some of the unique challenges with creating profiles in a health system environment and the need to set clearly communicated limitations of the project.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}