
-
 women receiving palbociclib (PAL) for hormone receptor-positive (HR+)/human epidermal growth factor receptor 2-negative (HER2‒) advanced breast cancer (ABC) in a real-world setting: Treatment patterns from POLARIS by MS Karuturi, A Garrett, JL Blum, J Anderson, E Jensen, T Pluard, Thomas Stanton, K Manning, JC Cappelleri, F Beery, Y Wang, and D Tripathy")
Pre/perimenopausal (preMeno) women receiving palbociclib (PAL) for hormone receptor-positive (HR+)/human epidermal growth factor receptor 2-negative (HER2‒) advanced breast cancer (ABC) in a real-world setting: Treatment patterns from POLARIS
MS Karuturi, A Garrett, JL Blum, J Anderson, E Jensen, T Pluard, Thomas Stanton, K Manning, JC Cappelleri, F Beery, Y Wang, and D Tripathy
-

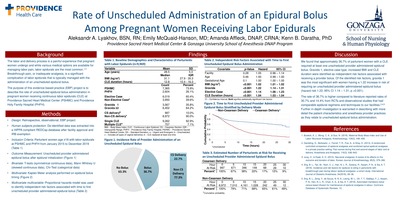
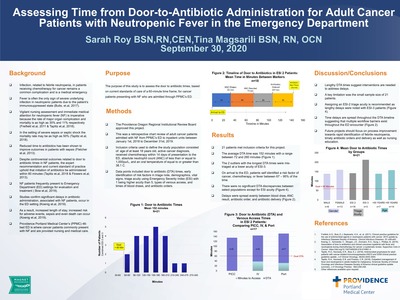
Rate of Unscheduled Administration of an Epidural Bolus Among Pregnant Women Receiving Labor Epidurals
Aleksandr A. Lyakhov, Emily L. McQuaid-Hanson, Amanda Affleck, and Kenn B Daratha
Background The labor and delivery process is a painful experience that pregnant women undergo and while various medical options are available for managing labor pain, labor epidurals are the most common.1,3 Breakthrough pain, or inadequate analgesia, is a significant complication of labor epidurals that is typically managed with the administration of an unscheduled epidural bolus. The purpose of this evidence-based practice (EBP) project is to describe the rate of unscheduled epidural bolus administration in pregnant women receiving continuous labor epidurals (CLE) at Providence Sacred Heart Medical Center (PSHMC) and Providence Holy Family Hospital (PHFH).
Methods • Design: Retrospective, observational, EBP project • Human subjects protection: De-identified data was extracted into a HIPPA compliant REDCap database after facility approval and IRB exemption • Inclusion Criteria: Parturient women age ≥18 with labor epidurals at PSHMC and PHFH from January 2015 to December 2019 (Table 1) • Outcome Measurement: Unscheduled provider administered epidural bolus after epidural initialization (Figure 1) • Bivariate: T-tests (symmetrical continuous data), Mann Whitney U (skewed continuous data), Chi-Test (categorical data) • Multivariate: Kaplan Meier analysis performed on epidural bolus timing (Figure 2) • Multivariate multivariable: Proportional hazards model was used to identify independent risk factors associated with time to first unscheduled provider administered epidural bolus (Table 2)
Discussion We found that approximately 36.7% of parturient women with a CLE required at least one unscheduled provider administered epidural bolus. Gravida 1, elective case type, increased BMI and CLE duration were identified as independent risk factors associated with receiving a provider bolus. Of the identified risk factors, gravida 1 was the most significant with women having a 1.22 increase in risk of requiring an unscheduled provider administered epidural bolus (hazard risk 1.22; 95% CI 1.14 – 1.31; p <0.001). The rate of 36.7% is higher compared to literature reported rates of 30.7% and 14.4% from RCTs and observational studies that had comparable epidural regimens and techniques to our facilities. 2,4,5 Further in-depth investigation is warranted in describing with more detail the patient characteristics and anesthesia provider practices as they relate to unscheduled epidural bolus administration.
-
Pulmonary Exacerbations
Kristina Montemayer, Allison A. Lambert, and Natalie E. West
Pulmonary exacerbations (PEx) are a frequent occurrence in the lives of individuals with cystic fibrosis (CF) and are associated with worsened morbidity, mortality, and quality of life. Approximately 25–35% individuals with CF don’t recover to 90% of baseline lung function after treatment for a PEx. Currently, there is scant evidence upon which to base guidelines for detection and management of PEx; therefore, the CF Foundation convened a working group to design and conduct clinical trials in order to establish evidence for best practices (Standardized Treatment of Pulmonary Exacerbations, STOP). The STOP program has conducted an observational study which has helped define the phenotype of PEx, characterize physician treatment practices, and evaluate clinical endpoints to use in future clinical trials. STOP-2 is an ongoing clinical trial of duration of antibiotics, which should guide establishment of best practices on duration. This chapter reviews the definition, epidemiology, current treatment practices, prognosis, and associated outcomes related to CF PEx. A patient perspective highlights the burden of PEx on the lives of individuals with CF. Current research is reviewed to clarify future directions in PEx. Upcoming clinical trials of PEx should provide robust clinical data in order to provide clear guidelines on detection and treatment of PEx.
-

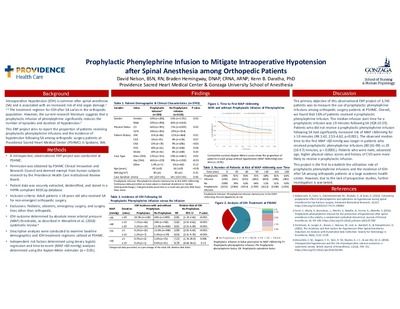
Prophylactic Phenylephrine Infusion to Mitigate Intraoperative Hypotension after Spinal Anesthesia among Orthopedic Patients
David Nelson, Braden Hemingway, and Kenn B Daratha
Background
Intraoperative Hypotension (IOH) is common after spinal anesthesia (SA) and is associated with an increased risk of end organ damage.1 2 3 The treatment regimen for IOH after SA varies in the orthopedic population. However, the current research literature suggests that a prophylactic infusion of phenylephrine significantly reduces the number of episodes and duration of hypotension.1 This EBP project aims to report the proportion of patients receiving prophylactic phenylephrine infusions and the incidence of hypotension following SA among orthopedic surgery patients at Providence Sacred Heart Medical Center (PSHMC) in Spokane, WA.
Methods
• A retrospective, observational EBP project was conducted at PSHMC. • Permission was obtained by PSHMC Clinical Innovation and Research Council and deemed exempt from human subjects research by the Providence Health Care Institutional Review Board. • Patient data was securely extracted, deidentified, and stored in a HIPPA compliant REDCap database. • Inclusion criteria: Adult patients ≥ 18 years old who received SA for non-emergent orthopedic surgery. • Exclusions: Pediatric, obstetric, emergency surgery, and surgery lines other than orthopedic. • IOH outcome determined by absolute mean arterial pressure (MAP) thresholds, as described in Wesselink et al. (2018) systematic review.4 • Descriptive analyses were conducted to examine baseline demographics and IOH treatment regimens utilized at PSHMC. • Independent risk factors determined using binary logistic regression and time-to-event (MAP <60 >mmHg) analyses determined using the Kaplan-Meier estimator (α = 0.05).
Discussion
The primary objective of this observational EBP project of 3,745 patients was to measure the use of prophylactic phenylephrine infusions among orthopedic surgery patients at PSHMC. Overall, we found that 16% of patients received a prophylactic phenylephrine infusion. The median infusion start time for a prophylactic infusion was 19 minutes following SA [IQR 10-29]. Patients who did not receive a prophylactic phenylephrine infusion following SA had significantly increased risk of MAP <60mmHg for>≥ 10 minutes (RR 3.42, 2.55-4.62, p<0.001). The observed median time to the first MAP <60 mmHg was longer in patients who received prophylactic phenylephrine infusions (80 [41-99] vs 29 [16-57] minutes, p < 0.0001). Patients who were male, advanced age, higher physical status scores and history of CVD were more likely to receive a prophylactic infusion. This project is the first to establish the utilization rate of prophylactic phenylephrine infusions and the incidence of IOH after SA among orthopedic patients at a large academic health center. However, due to the lack of prospective studies, further investigation is warranted.
-

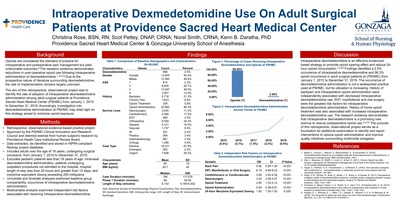
Intraoperative Dexmedetomidine Use On Adult Surgical Patients at Providence Sacred Heart Medical Center
Christina Rose, Scot Pettey, Norel Smith, and Kenn B Daratha
Background Opioids are considered the standard of practice for intraoperative and postoperative pain management but yield unfavorable outcomes.6 The research evidence demonstrates reductions in post-operative opioid use following intraoperative administration of dexmedetomidine.1,3,4,5,6 Due to the prospective nature of literature surrounding dexmedetomidine, the rate of implementation remains largely unknown. The aim of this retrospective, observational project was to identify the rate of adoption of intraoperative dexmedetomidine administration among adult surgical patients at Providence Sacred Heart Medical Center (PSHMC) from January 1, 2015 to December 31, 2019. Accordingly, investigation into dexmedetomidine administration at PSHMC may shed light on this strategy aimed to minimize opioid exposure
Methods • Retrospective, observational evidence-based practice project. • Approved by the PSHMC Clinical Innovation and Research Council and deemed exempt from human subject's research by Providence Health Care Institutional Review Board. • Data extracted, de-identified and stored in HIPPA compliant Redcap project database. • Included adults over the age of 18 years, undergoing surgical procedure from January 1, 2015 to December 31, 2019. • Excluded pediatric patients less than 18 years of age, intranasal dexmedetomidine administration, patients undergoing outpatient procedures not admitted to the hospital, hospital length of stay less than 24 hours and greater than 14 days, and morphine equivalent dosing exceeding 200 milligrams. • Univariate and bivariate analyses examined baseline group comparability, occurrence of intraoperative dexmedetomidine administration. • Multivariable analysis examined independent risk factors associated with receiving intraoperative dexmedetomidine.
Discussion Intraoperative dexmedetomidine is an effective evidencedbased strategy to promote opioid sparing effect and reduce 24- hour opioid consumption.1,4,5,6 Findings identified a 2.5% occurrence of intraoperative dexmedetomidine and 96.3% opioid occurrence in adult surgical patients at (PSHMC) from January 1, 2015 to December 31, 2019. The occurrence of dexmedetomidine administration is not a widespread practice used at PSHMC, but its utilization is increasing. History of backpain and intraoperative opioid administration were independently associated with decreased intraoperative dexmedetomidine use. ENT, maxillofacial and oral surgery were the greatest risk factors for intraoperative dexmedetomidine administration. History of home opioid treatment was also associated with increased intraoperative dexmedetomidine use. The research evidence demonstrates that intraoperative dexmedetomidine is a promising new avenue to reduce postoperative opioid use.3,4,5,6 The purpose of this retrospective, observational project serves as a foundation for additional examination to identify and report interventions to reduce opioid administration and improve quality initiatives surrounding multimodal analgesia.
-

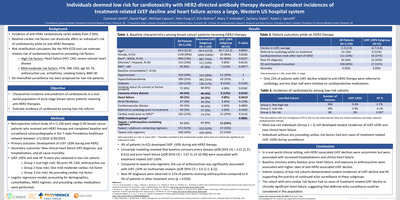
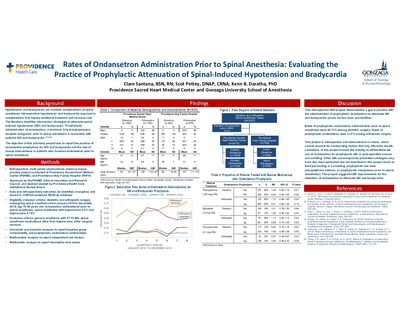
Rates of Ondansetron Administration Prior to Spinal Anesthesia: Evaluating the Practice of Prophylactic Attenuation of Spinal-Induced Hypotension and Bradycardia
Clare Santana, Scot Pettey, and Kenn B Daratha
Background Hypotension and bradycardia are common complications of spinal anesthesia. Intraoperative hypotension and bradycardia may lead to complications that require additional treatment and increase cost. The literature identifies intervention strategies to attenuate spinalinduced hypotension (SIH) and bradycardia.1 Prophylactic administration of ondansetron, a serotonin 5-hydroxytryptamine receptor antagonist, prior to spinal anesthesia is associated with reduced SIH and bradycardia.1,2,3,4,6 The objective of this scholarly project was to report the practice of ondansetron prophylaxis for SIH and bradycardia and the rate of rescue interventions in patients who received ondansetron prior to spinal anesthesia.
Methods Retrospective, multi-center observational evidence-based practice project conducted at Providence Sacred Heart Medical Center (PSHMC) and Providence Holy Family Hospital (PHFH) • Approved by the PSHMC Clinical Innovation and Research Council, and deemed exempt by Providence Health Care Institutional Review Board • Data was retrospectively extracted, de-identified, encrypted, and stored in a HIPAA-compliant REDCap database • Eligibility inclusion criteria: obstetric and orthopedic surgery undergoing spinal anesthesia from January 2018 to December 2019, age 18-90 years old, ondansetron administered prior to spinal anesthesia, spinal anesthesia with bupivacaine 0.5% and bupivacaine 0.75% • Exclusion criteria: general anesthesia with ETT/LMA, spinal anesthesia medications other than bupivacaine, other surgical services • Univariate and bivariate analyses to report baseline group comparability and prophylactic ondansetron relationships • Multivariable analysis to report independent risk factors • Multivariate analysis to report descriptive time series
Discussion This retrospective EBP project demonstrated a gap in practice with the administration of prophylactic ondansetron to attenuate SIH and bradycardia across service lines and facilities. Rates of prophylactic ondansetron administration prior to spinal anesthesia were 42-73% among obstetric surgery. Rates of prophylactic ondansetron were 2-12% among orthopedic surgery. This project is retrospective and observational in nature, which cannot account for confounding factors that may affect the results. Limitations of this project include the inability to differentiate the use of ondansetron for prophylactic SIH or post-operative nausea and vomiting. Other SIH and bradycardia prevention strategies may have also been performed but not described in this project (such as fluid pre-loading or co-loading, prophylactic low dose phenylephrine infusion, or prophylactic vasopressor prior to spinal anesthesia). This project suggests EBP improvements for the utilization of ondansetron to attenuate SIH and bradycardia.
-

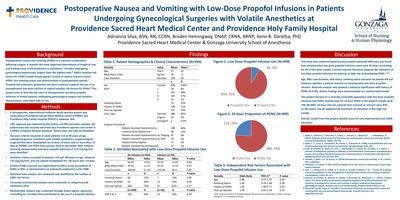
Postoperative Nausea and Vomiting with Low-Dose Propofol Infusions in Patients Undergoing Gynecological Surgeries with Volatile Anesthetics at Providence Sacred Heart Medical Center and Providence Holy Family Hospital
Adrianna Silva, Braden Hemingway, and Kenn B Daratha
Background Postoperative nausea and vomiting (PONV) is a common complication following surgery. It remains the most important determinant of length of stay and leading cause of dissatisfaction in anesthesia.4 Females undergoing gynecological laparoscopic surgery have the highest rates.8 Apfel’s baseline risk factors for PONV include female gender, history of motion sickness and/or PONV, non-smoking status and administration of postoperative opioids.1 Propofol has antiemetic properties and Gan’s evidence supports the use of an intraoperative low-dose infusion to reduce baseline risk factors for PONV.6 This project aims to describe the rates of intraoperative low-dose propofol infusions in female patients undergoing gynecological surgery and baseline characteristics associated with its use.
Methods • A retrospective, observational evidence-based practice project was conducted at Providence Sacred Heart Medical Center (PSHMC) and Providence Holy Family Hospital (PHFH) in Spokane, WA. • CIRC approval was obtained by the facility and IRB exemption granted. All patient data was securely extracted by a Providence sponsor and stored in a HIPAA compliant REDCap database. Patient data was fully de-identified. • Inclusion criteria consisted of adult patients ≥18 to 90 years of age undergoing general anesthesia with volatile anesthetics in gynecological surgeries that were hospitalized for at least 24 hours and no more than 14 days at PSHMC and PHFH from January 2014 to December 2019. Patients receiving intraoperative low-dose propofol infusions of ≤25 mcg/kg/min were identified. • Exclusion criteria consisted of patients <18 and>90 years of age, infusions >25 mcg/kg/min, and any patient hospitalized for <24 hours and>14 days. • 24-hour PONV outcome was determined by PACU nurse assessment of PONV in EPIC or administration of antiemetic medication in the EMR. • Statistical data analysis was conducted and stratified by the number of Apfel risk factors. • Univariate and bivariate analysis were conducted on categorical and continuous data. • Multivariable analysis was conducted through binary logistic regression controlling for variables that contributed to the use of a propofol infusion.
Discussion This multi-year evidence-based practice project examined 499 cases and found that intraoperative low-dose propofol infusions were used 45 times accounting for 9% of the total sample. Current research literature supports the utilization of low-dose propofol infusions for patients at high-risk of developing PONV. 3,6,7 Age, BMI, case duration, ASA status, smoking status and post-op opioids did not influence whether a patient received an intraoperative low-dose propofol infusion. Bivariate analysis only showed a statistical significance with history of PONV (P=0.04). Similar findings were demonstrated in a multivariable model. This project focused on a clinically vulnerable population with low-dose propofol infusions and PONV. Overall rates for 24-hour PONV in this patient sample were 76% (N=499). 24-hour rates for patients that received an infusion were 84% (n=45) which may be explained by treatment by indication in this high-risk sample. Overall, results from this project identify areas for care improvement and CRNA education.
-

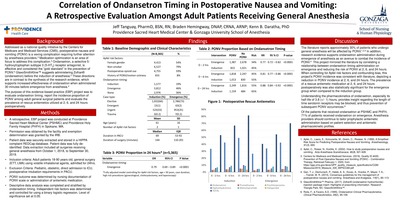
Correlation of Ondansetron Timing in Postoperative Nausea and Vomiting: A Retrospective Evaluation Amongst Adult Patients Receiving General Anesthesia
Jeff Tanguay, Braden Hemingway, and Kenn B Daratha
Background Addressed as a national quality initiative by the Centers for Medicare and Medicaid Services (CMS), postoperative nausea and vomiting (PONV) is a vexing complication requiring further attention by anesthesia providers.3 Medication optimization is an area of focus to address this complication.4 Ondansetron, a selective 5- hydroxytryptophan subtype 3 (5-HT3 ) receptor antagonist, is effective and considered the “gold standard” in the prevention of PONV.4 GlaxoSmithKline™ suggests administering Zofran® (ondansetron) before the induction of anesthesia.5 These directions are in contrast to the synthesis of the research evidence, which supports increased effectiveness of ondansetron when administered 30 minutes before emergence from anesthesia.4 The purpose of this evidence-based practice (EBP) project was to evaluate ondansetron timing, report the incidence proportion of PONV among adult general surgical patients and evaluate the prevalence of rescue antiemetics utilized at 2, 6, and 24 hours postoperatively.
Methods A retrospective, EBP project was conducted at Providence Sacred Heart Medical Center (PSHMC) and Providence Holy Family Hospital (PHFH) in Spokane, WA. • Permission was obtained by the facility and exemption determination was granted by the IRB. • Patient data was securely extracted and stored in a HIPPA complaint REDCap database. Patient data was fully deidentified. Data extraction included all surgeries receiving general anesthesia from October 1, 2018, to September 30, 2019. • Inclusion criteria: Adult patients 18-90 years old, general surgery (ETT, LMA) using volatile inhalational agents, admitted for 24hrs. • Exclusion Criteria: Pediatric, obstetric, direct admission to ICU, postoperative intubation requirements in PACU. • PONV outcome was determined by nursing documentation of PONV scale or administration of antiemetic medication. • Descriptive data analysis was completed and stratified by ondansetron timing. Independent risk factors was determined and controlled for using a binary logistic regression. Level of significance set at 0.05.
Discussion The literature reports approximately 30% of patients who undergo general anesthesia will be affected by PONV. 1,2,4 In addition, research evidence supports ondansetron administration during emergence of anesthesia as an avenue to combat the incidence of PONV. 4 This project mirrored the literature by correlating a relationship between ondansetron timing administration on emergence and reducing the risk of PONV at 2, 6, and 24 hours. When controlling for Apfel risk factors and confounding bias, this project’s PONV incidence was consistent with literature, depicting a reduction in PONV incidence at 2, 6, and 24 hours. The prevalence of a rescue antiemetic medication at 2, 6, and 24 hours postoperatively was also statistically significant for the emergence group when compared to the induction group. Understanding the pharmacokinetics of ondansetron, especially its half-life of 3.8 (+/- 1) hours, provides insight regarding the length of time serotonin receptors may be blocked, and thus prevention of subsequent PONV occurrences. 6 Of the patients that received ondansetron at PSHMC and PHFH, 71% of patients received ondansetron on emergence. Anesthesia providers should continue to tailor prophylactic antiemetic administration based on patient selection and antiemetic pharmacokinetic profiles.
-

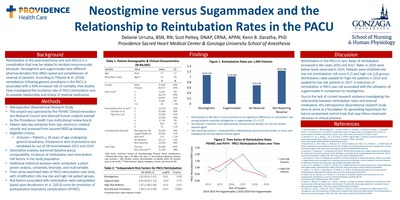
Neostigmine versus Sugammadex and the Relationship to Reintubation Rates in the PACU
Delanie Urrutia, Scot Pettey, and Kenn B Daratha
Background Findings Discussion Reintubation in the post-anesthesia care unit (PACU) is a complication that may be related to residual neuromuscular blockade. Neostigmine and sugammadex have different pharmacokinetics that effect speed and completeness of reversal of paralysis. According to Tillquist et al. (2016) reintubation following general anesthesia in the PACU is associated with a 50% increased risk of mortality. Few studies have investigated the incidence rate of PACU reintubation and its possible relationship and choice of reversal medication.
Methods • Retrospective Observational Research Study. • This project was approved by the PSHMC Clinical Innovation and Research Council and deemed human subjects exempt by the Providence Health Care institutional review board. • Patient data was extracted from Epic electronic medical records and accessed from secured REDCap database. • Eligibility Criteria: • Inclusion – Patients > 18 years of age undergoing general anesthesia, intubated at start of procedure and extubated by out of OR time between 2013 and 2019. • Descriptive analyses examined baseline group comparability, incidence of reintubation and reintubation risk factors in the study population. • Additional statistical analyses were conducted: a-priori power analysis, univariate, bivariate, and multivariable. • Time series examined rates of PACU reintubation over time, with stratification into low risk and high risk patient groups. • Risk factors associated with reintubation were extrapolated based upon Bruekmann et al. (2013) score for prediction of postoperative respiratory complications (SPORC).
Discussion Reintubation in the PACU is rare. Rates of reintubation increased in the years 2016 and 2017. Rates in 2019 were below levels observed in 2014. Patients were stratified into low risk (reintubation risk score 0-2) and high risk (>3) groups. Reintubation rates peaked for high risk patients in 2016 and peaked for low risk patients in 2017. A reduction of reintubation in PACU was not associated with the utilization of sugammadex in comparison to neostigmine. Due to the lack of current research evidence investigating the relationship between reintubation rates and reversal medication, this retrospective observational research study aims to serve as a foundation for generating hypotheses for future randomized control trials that may inform treatment decisions in clinical practice.
-

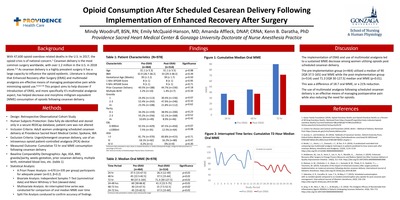
Opioid Consumption After Scheduled Cesarean Delivery Following Implementation of Enhanced Recovery After Surgery
Mindy Woodruff, Emily L. McQuaid-Hanson, Amanda Affleck, and Kenn B Daratha
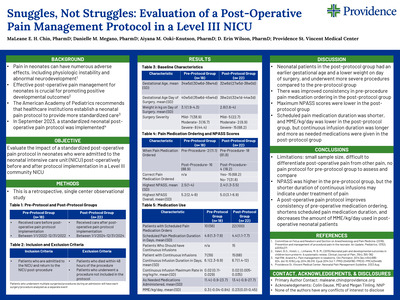
Background With 47,600 opioid overdose related deaths in the U.S. in 2017, the opioid crisis is of national concern.1 Cesarean delivery is the most common surgery worldwide, with over 1.2 million in the U.S. in 2018 alone.2,3 As cesarean delivery is a highly prevalent surgery it has a large capacity to influence the opioid epidemic. Literature is showing that Enhanced Recovery after Surgery (ERAS) and multimodal analgesia are effective means of managing postoperative pain while minimizing opioid use.4,5,6,7,8 This project aims to help discover if introduction of ERAS, and more specifically it’s multimodal analgesia aspect, has helped decrease oral morphine milligram equivalent (MME) consumption of opioids following cesarean delivery.
Methods • Design: Retrospective Observational Cohort Study • Human Subjects Protection: Data fully de-identified and stored only in a secure REDCap database; patient care was not altered • Inclusion Criteria: Adult women undergoing scheduled cesarean delivery at Providence Sacred Heart Medical Center, Spokane, WA • Exclusion Criteria: Urgent/emergent cesarean delivery, use of an intravenous opioid patient-controlled analgesia (PCA) device • Measured Outcome: Cumulative 72-hr oral MME consumption following cesarean delivery • Baseline Comparability Demographics: Age, ASA, BMI, gravida/parity, weeks gestation, prior cesarean delivery, multiple birth, estimated blood loss, etc. (table 1) • Statistical Analysis: • A Priori Power Analysis: n=670 (n=335 per group) participants for adequate power (α=0.5, β=0.2) • Bivariate Analysis: Independent Samples T-Test (symmetrical data) and Mann Whitney U Test (skewed data) • Multivariate Analysis: An interrupted time series was conducted for comparison of oral median MME over time • Split File Analysis conduced to confirm accuracy of findings
Discussion The implementation of ERAS and use of multimodal analgesia led to a sustained MME decrease among women utilizing opioids post scheduled cesarean delivery. The pre-implementation group (n=464) utilized a median of 90 [IQR 37.5-165] oral MME while the post-implementation group (n=514) used 71.3 [IQR 30-127.5] median oral MME (p<0.01). This was a difference of 18.7 oral MME, or a 21% reduction. The use of multimodal analgesia following scheduled cesarean delivery is an effective means of managing postoperative pain while also reducing the need for opioids.
-

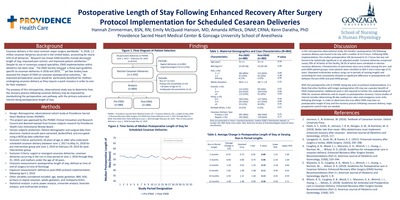
Postoperative Length of Stay Following Enhanced Recovery After Surgery Protocol Implementation for Scheduled Cesarean Deliveries
Hannah Zimmerman, Emily L. McQuaid-Hanson, Amanda Affleck, and Kenn B Daratha
Background Cesarean delivery is the most common major surgery worldwide. 1 In 2018, 1.2 million cesarean deliveries occurred in the United States, accounting for nearly 32% of all deliveries.2 Research has shown ERAS benefits include decreased length of stay, improved pain control, and improved patient satisfaction.2,3 Despite its use in numerous surgical specialties, ERAS implementation within obstetrics has been slow.2 The ERAS Society released a three-part guideline specific to cesarean deliveries in 2018 and 2019,4,5,6 yet few studies have assessed the impact of ERAS on cesarean postoperative outcomes.2 An improved perioperative course would be particularly beneficial for mothers undergoing cesarean delivery as they require a quick recovery in order to care for their newborn. The purpose of this retrospective, observational study was to determine how the recovery process following cesarean delivery may be improved by standardizing the perioperative care pathway, with the primary outcome of interest being postoperative length of stay.
Methods • Design: Retrospective, observational cohort study at Providence Sacred Heart Medical Center (PSHMC) • This project was approved by the PSHMC Clinical Innovation and Research Council and deemed exempt from human subjects research by Providence Health Care Institutional Review Board. • Human subjects protection: Patient demographic and surgical data from electronic medical records were extracted, deidentified, and encrypted using a REDCap data collection tool • Inclusion Criteria: parturients 18 years of age or older who underwent scheduled cesarean delivery between June 1, 2017 to May 31, 2018 for pre-intervention group and June 1, 2019 to February 29, 2019 for postintervention group. • Exclusion Criteria: urgent or emergent cesarean deliveries, cesarean deliveries occurring in the run-in time period of June 1, 2018 through May 31, 2019, and mothers under the age of 18 years. • Outcome measurement: postoperative length of stay, defined as time of end of surgery to time of discharge • Exposure measurement: defined as post-ERAS protocol implementation following April 1, 2019. • Other variables considered included: age, weeks gestation, BMI, ASA, primary vs repeat cesarean, weeks gestation, and multiparty births. • Statistical analysis: a-prior power analysis, univariate analysis, bivariate analysis, and multivariate analysis
Discussion In this retrospective observational study, this facility’s postoperative LOS following cesarean delivery was found to be low, with a median of 52.4 hours. Following ERAS implementation, the median postoperative LOS decreased to 51.2 hours but was not found to be statistically significant in an adjusted model. Cesarean deliveries comprised nearly 29% of all births at this facility, 58.5% of which were scheduled or elective cesarean deliveries. Characteristics of parturients were very similar among the pre- and post-ERAS patient groups; most patients were classified as ASA 2 and a mean age of 31 years. Repeated multivariate analysis using run-in periods of varying lengths and controlling for time consistently showed no significant difference in postoperative LOS between the pre-ERAS and post-ERAS groups. With the postoperative LOS at PSHMC being low prior to protocol implementation, it is likely that other facilities with longer postoperative LOS may see a greater benefit of ERAS implementation. Additional work is still required to further the understanding of ERAS for cesarean deliveries and its impact on postoperative recovery. Future studies of interest includes determining 30-day readmission rates and emergency room visits following discharge. In order to determine the true effect ERAS may have on postoperative length of stay and the recovery process following cesarean delivery, large prospective control trials are needed.
-

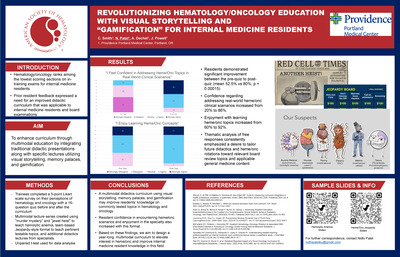
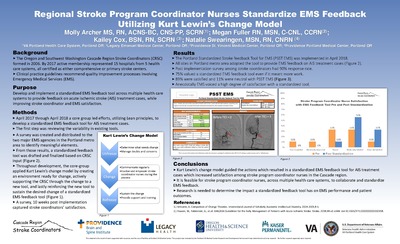
Regional Stroke Program Coordinator Nurses Standardize EMS Feedback Utilizing Kurt Lewin’s Change Model
Molly Archer, Megan Fuller, Kailey Cox, and Natalie Swearingen
-
 ≤ 5 Treated with Endovascular Thrombectomy vs Medical Management by Steven Augustine, Lindsay Lucas, Elizabeth Baraban, and Jason Tarpley")
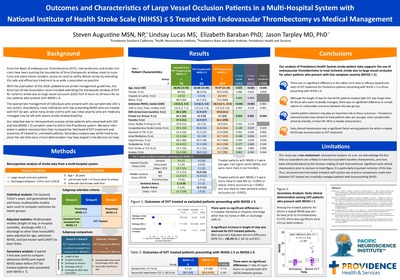
Outcomes and Characteristics of Large Vessel Occlusion Patients in a Multi-Hospital System with National Institute of Health Stroke Scale (NIHSS) ≤ 5 Treated with Endovascular Thrombectomy vs Medical Management
Steven Augustine, Lindsay Lucas, Elizabeth Baraban, and Jason Tarpley
-

Fast and Furious: Stroke Update 2019
Mary Kay Bader
This lecture focuses on the AHA guidelines and how the Acute Stroke Team focuses the efforts in the first few hours after presentation. Audience will be made up of physicians, nurses and EMT/EMS personnel. The aims of the event include providing a couple ‘cutting edge’ key note speakers with varying expertise from different parts of the acute stroke care continuum.
-

Managing Severe TBI in the ICU Setting using a Three Tier Approach
Mary Kay Bader
Objectives:
- Assess the effects of injury to the brain in the neurologic injured patient and implement a tiered approach to manage severe TBI
- Evaluate TBI patients using multimodality monitoring
- Apply interventions to manage brain injury & integrate the complex multi-system issues and manage these patients using an actual case study.
-

Practice with Purpose & Passion
Mary Kay Bader
Objectives:
- Integrate the components of clinical practice in an ICU environment including elements of team membership/performance, teamwork, shared decision making, communication and collaboration
- Demonstrate passion in delivering care in the ICU environment by reflecting on the meaning of nursing care and generating fuel to inspire the clinical team in the work environment
-

Technology: Inside the Black Box -- Managing Neuro Patients
Mary Kay Bader
Objectives:
- Identify the pathophysiology and cellular processes related to brain injury responses
- Describe the indications, functions, data analysis, and suggested interventions with various monitors of the brain
- Apply this technology to the care of the critically injured neuro patient using evidenced based protocols
-

Temperature Management: All Shook Up! Managing Shivering In Normothermia
Mary Kay Bader
Objectives:
- Identify key factors related to maintaining normothermia
- Describe the use of the Bedside Shivering Assessment Scale
- Provide interventions to manage shivering in the Neuro patient population
-

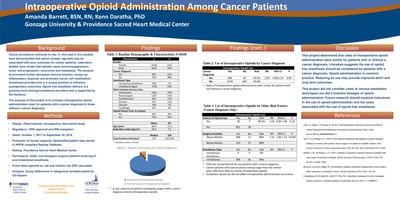
Intraoperative Opioid Administration Among Cancer Patients
Amanda Barrett and Kenn B Daratha
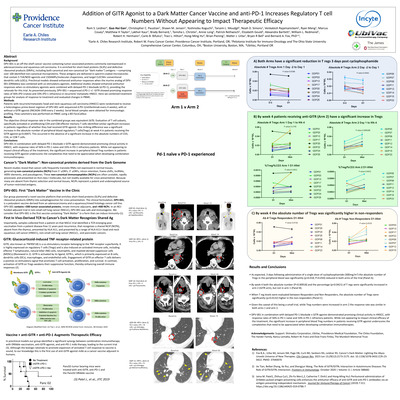
Background Cancer prevalence continues to rise. In vitro and in vivo studies have demonstrated that opioid receptor agonists may be associated with poor outcomes for cancer patients. Laboratory studies have shown that opioids cause immunosuppression; tumor cell progression, recurrence and metastasis. The surgical environment further decreases immune function, causes an inflammatory response and promotes cancer cell mobilization. Anesthesia providers are in a unique position to influence postoperative outcomes. Opioid free anesthetic delivery is a growing trend amongst anesthesia providers and is supported by the literature. The purpose of this project is to compare intraoperative opioid administration rates for patients with a cancer diagnosis to those without a cancer diagnosis.
Methods • Design: Observational, retrospective, descriptive study • Regulatory: CIRC approval and IRB exemption • Dates: October 1, 2017 to September 30, 2018 • Protection of human subjects: Deidentified patient data stored in HIPPA compliant Redcap Database • Setting: Providence Sacred Heart Medical Center • Participants: Adult, non-emergent surgical patients receiving IV and inhalational anesthesia • Event rates reported as risk and relative risk (RR) calculated • Analysis: Group differences in categorical variables tested by Chi-Square
Discussion This project determined that rates of intraoperative opioid administration were similar for patients with or without a cancer diagnosis. Literature suggests the use of opioid free anesthesia should be considered for patients with a cancer diagnosis. Opioid administration is common practice. Reducing its use may provide improved short and long term outcomes. This project did not consider costs of various anesthesia techniques nor did it examine dosages of opioid administration. Future research should examine reductions in the use of opioid administration and the costs associated with the use of opioid free anesthesia
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.










{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}