
-

Revolutionizing hematology/oncology education with visual storytelling and “Gamification” for internal medicine residents
N Smith1, A Patel1, J Dechet, and C Powell
Introduction: Hematology/oncology ranks among the lowest scoring sections on in-training exams for internal medicine residents. Prior resident feedback expressed a need for an improved didactic curriculum that was applicable to internal medicine residents and board examinations Aim: To enhance curriculum through multimodal education by integrating traditional didactic presentations along with specific lectures utilizing visual storytelling, memory palaces, and gamification. Methods: Trainees completed a 5-point Likert scale survey on their perceptions of hematology and oncology with a 16-question quiz before and after the curriculum. Multimodal lecture series created using "murder mystery" and "jewel heist" to teach hemolytic anemia, team-based Jeopardy-style format to teach pertinent testable topics, and additional didactics lectures from specialists. Unpaired t-test used for data analysis Conclusions: A multimodal didactics curriculum using visual storytelling, memory palaces, and gamification may improve residents' knowledge on commonly tested topics in hematology and oncology. Resident confidence in encountering heme/onc scenarios and enjoyment in the specialty also increased with this format. Based on these findings, we aim to design a year-long, multimodal curriculum to elevate interest in heme/onc and improve internal medicine resident knowledge in this field.
-

Puzzling Papules: Uncovering the Etiology of a Rash in a Returning Traveler
Lisa Stampke, MD and Shahana Baig-Lewis, MD
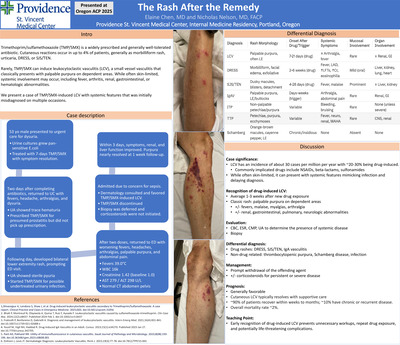
Introduction: There are an estimated 1.8 billion people that travel internationally every year [1]. Approximately 22-64% of those acquire an infectious disease during or after returning home that is not endemic to their home country [1]. This is especially concerning in our current political climate and declining vaccination rates in the United States which places more patients at risk for preventable diseases [2]. These factors present a unique challenge in diagnosing and treating a symptomatic returning traveler. Case Description: A 25-year-old incompletely vaccinated male returned from Kenya after volunteering for 5-weeks in a rural hospital. He was in his usual state of health until two days prior to admission when he developed fever, malaise, throat pain and dry cough. He boarded the airplane from Kenya and arrived in Oregon the day prior to admission with worsening symptoms and a new rash on his back. Denied abdominal pain, nausea, vomiting, diarrhea. While in Kenya, he was in a patient facing role while volunteering at a local hospital but denied sick contacts or traveling companions. No exposure to contaminated food or water. No sexual contacts. Prior to his trip he received Doxycycline for malaria prophylaxis, Hepatitis A and oral typhoid vaccines. Upon review of vaccination records, he did not receive the MMR vaccine as a child due to an adverse reaction in a relative. In the ED, he was placed in airborne precautions with vital signs notable for a fever of 39.3C and tachycardia. Physical exam with diffuse maculopapular, non-pruritic rash over back that was starting to coalesce and spread to the trunk, face and arms; sparing palms and soles. Noted to also have subtle bilateral injected conjunctiva and ulcerated oral lesions over the buccal mucosa. Workup revealed leukopenia and mild transaminase elevation. Negative blood cultures. Limited infectious workup initiated which later resulted positive for Rubeola. The patient was treated supportively and discharged home in good condition. Discussion: Measles, one of the most contagious infectious diseases, affects approximately 10.3 million people worldwide [2]. While measles is considered “eliminated” in the United States, rates continue to rise. In 2025, there has been a total of 1356 cases of Measles in the United States with 34% above the age of 20 and 13% requiring hospitalization [3]. Outbreaks often stem from unvaccinated international travelers [2]. This case highlights the importance of collecting a thorough vaccination history in this population to streamline infectious workup and reduce healthcare costs. Furthermore, this case underscores the critical need for continued vaccination advocacy in primary care to prevent resurgence of measles and other similar communicable and vaccine preventable illnesses.
-

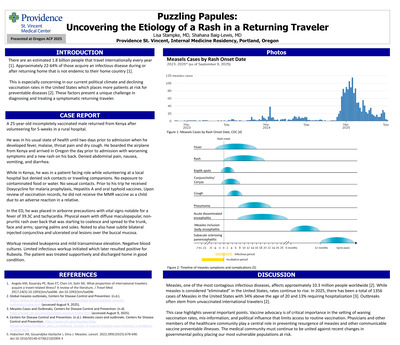
Hypercalcemic Crisis After Open Mitral Valve Replacement
Andrew Sunwood, DO and Jason Heino
59. Hypercalcemic Crisis After Open Mitral Valve Replacement Andrew Sunwood, DO Background: Hypercalcemic crisis is a rare manifestation of primary hyperparathyroidism characterized by a sudden increase in serum calcium levels to >14 mg/dL with symptoms of hypercalcemia including adverse gastrointestinal symptoms, abdominal pain, and even predisposition to cardiac arrhythmias. There is only one other documented case of hypercalcemic crisis occurring after open heart surgery. Case information: 69-year-old female with a history of primary osteoporosis on alendronate and valvular heart failure presented for mitral valve replacement. Preoperative lab work did not show evidence of electrolyte abnormalities. She under- went open bioprosthetic mitral valve replacement with tricuspid valve annuloplasty. She was taken to the cardiac intensive care unit for routine post-operative management and placed on dobutamine and furosemide infusions. Amiodarone was also started for post-operative atrial fibrillation/flutter. Post-operative day 3 (POD3), calcium levels were noted to rise to 10.5 mg/dL (normal 8.7-10.2 mg/dL). POD4, furosemide infusion was discontinued and calcium levels continued to rise to 11.2 mg/dL. The patient reported symptoms including increased sleepiness, brain fog, mild nausea, and decreased appetite. Further workup showed elevated intact parathyroid hormone 1310 pg/mL (normal 18-88 pg/mL), 25-hydroxyvitamin D 15.1 ng/mL (normal 20-50 ng/mL), and a negative parathyroid hormone-related peptide. Electrocardiogram showed sinus rhythm with a 1st degree AV block and QTc of 453 ms. A thyroid ultrasound demonstrated a 3 x 1.5 cm lesion on the left thyroid lobe, suspected parathyroid adenoma. Management included cinacalcet, normal saline infusion with IV furosemide for volume management, and zoledronic acid. Calcitonin was considered but was not on the hospital formulary. Serum calcium levels peaked on POD7 at 15.7 mg/dL with an ionized calcium of 2.15 mmol/L (normal 1.12-1.40 mmol/L). There was no evidence of arrhythmia apart from atrial fibrillation. She underwent parathyroidectomy revealing a left inferior parathyroid adenoma with immediate intraoperative normalization of parathyroid hormone levels post-resection. Serum calcium levels remained within normal limits for the remainder of her hospitalization, and she was discharged with vitamin D and calcium citrate. Discussion: Hypercalcemic crisis is a rare manifestation of hyperparathyroidism resulting in albumin-corrected calcium levels >14 mg/dL. This case illustrates hypercalcemic crisis in a patient likely with a longstanding parathyroid adenoma but without prior evidence of hypercalcemia. The sternotomy is the suspected trigger for the hypercalcemic crisis, whether from trauma and localized inflammation or related to cardiopulmonary bypass, with only one other documented case after coronary artery bypass grafting in a previously normocalcemic patient found to have a parathyroid adenoma. Management of hypercalcemic crisis includes stabilization through normal saline infusions and reduction of serum calcium levels with +cinacalcet, bisphosphonates, and calcitonin, if possible; and definitive treatment with parathyroidectomy. Post-valvular surgery patients especially require close moni- toring for signs of cardiac arrhythmias given the heightened risk post-operation.
-

Financial impact of hepatitis B screening for subsequent chemotherapy
Shaye Suzuki, PharmD and Shuntao Cai, PharmD, BCOP
Abstract: The American Society of Clinical Oncology (ASCO) released an opinion that all patients on systemic anticancer therapy should be tested for hepatitis B virus (HBV) but gave no formal guidance on additional HBV testing if the initial HBV test is negative. It is unknown whether performing these tests is resulting in significant costs. The aim of this retrospective chart review is to determine the cost associated with HBV testing through various definitions of “unnecessary testing”. The rates of new potentially actionable HBV tests during retesting defined by HBV core antibody and surface antigen positive will also be determined. This is a multi-center, retrospective chart review that was performed across 4 Providence Health Plan oncology clinics in Oregon. Electronic medical records of patients with a chemotherapy treatment plan between May 2025-July 2025 were reviewed. The data collected were demographics (age, gender, ethnicity, type of cancer), HBV test results (for all tests performed), line of treatment (1st, 2nd, 3rd , etc), time each test was taken, and the use of a CD20 chemotherapy medication. For the results, the cost per test was multiplied by the number of tests that were determined to be unnecessary, through various definitions, and compared to the cost of all tests performed. Rates of new potentially actionable HBV tests were also calculated. A total of 565 patient charts were reviewed, and there were 265 new hepatitis B tests performed. This correlates to a cost of $25,600. On average, the time between treatments, when a new test was performed, was about 25 months compared to about 10 months between treatments when new tests were not done. When looking at patients who had a potentially actionable hepatitis B test result, there were 5 total patients (< 1%) who were not on CD20 therapy that had a new potentially actionable HBV test. Of these 5 patients, there were no consistent patterns in patient demographics, chemotherapy regimen, or type of cancer that would increase one’s risk of having a new potentially actionable HBV result. From this data, we cannot recommend changing the current practice regarding repeating hepatitis B testing. The inherent risk of having a new potentially actionable hepatitis B result still exists for all patients, on CD20 therapy or not. The monetary cost of missing a new potentially actionable result and the complications that may arise leading to a hospital admission outweigh the cost of our current practice for repeat HBV testing. (IRB exempt) Learning Objectives: Determine the financial impact of subsequent HBV testing through various definitions of “unnecessary testing”. Presentation Category: Medication Safety/Quality Improvement
-

Sepsis Transitional Care Management: A Phone Call to Reduce Readmission Health Inequity
Linh Tang Taylor, MD; Erica Leser, MS; Alyssa Nelson; and Michelle Schopeflin Sanders, MD
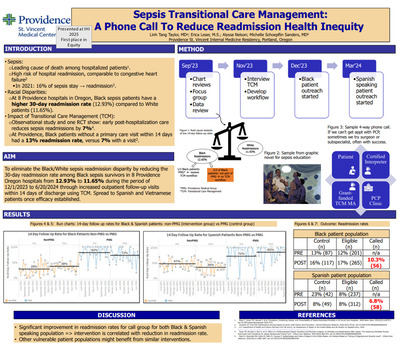
Introduction: Sepsis accounts for 52% of hospital admissions in the United States and is the leading cause of death among hospitalized patients1 . However, disparity exists among sepsis survivors with race being reported as a determinant of recovery2 . Such disparity exists in Providence Oregon 8 hospitals: Providence Black patients have higher sepsis readmission rates than White (12.93% vs 11.65%). Using modified community-based participatory research, data analysis, and stakeholder interviews, we identified one potential root cause of the disparity: Black patients being readmitted are not receiving our system's Transitional Care Management (TCM) services. We aim to eliminate the Black/White sepsis readmission disparity by reducing the 30-day readmission rate among Black sepsis survivors in 8 Providence Oregon hospitals from 12.93% to 11.65% during the period of 12/1/2023 to 6/20/2024 through increased outpatient follow-up visits within 14 days of discharge by delivering TCM intervention to those who are not eligible for one with our health system. Methods: In PDSA 1, a resident physician & nurse coordinator delivered TCM phone call intervention for Black sepsis patients who don’t qualify for the system TCM intervention due to insurance status. With these phone calls, patients are reminded to follow up with their PCP, finish their antibiotics, and given sepsis education material via either MyChart or mail delivery. If patient doesn’t have a PCP, we referred them to a federally qualified health center to get established, or to a free clinic. In PDSA 2, 1 medical student and 1 Spanish-speaking grant-funded medical assistant are added to the team to continue delivering intervention to Black sepsis patients. With Spanish-speaking patients, we helped them navigate complex phone trees of clinic that are sometimes only in English. Results: Results showed improvement in 14-day follow up rates for Black patients population (up to 38% from 28%) but not for Spanish-speaking patient population (down to 36% from 47%). Readmission rate increased significantly for both groups: readmission rates for the intervention group for Black patients decreased to 10.3% from 16%. Readmission rate for the intervened group for Spanish-speaking patients decreased to 6.8% from 8%. Conclusion: Promising results in reducing sepsis readmission rates for both Black and Spanish-speaking patients is an indication that TCM intervention may be correlated with reducing sepsis readmission health inequity.
-

Hydroxocobalamin in Septic Shock Management – Should It Be Introduced Sooner?
Linh Tang Taylor, MD; Cameron Miles Long, MD; and Omar Pandhair
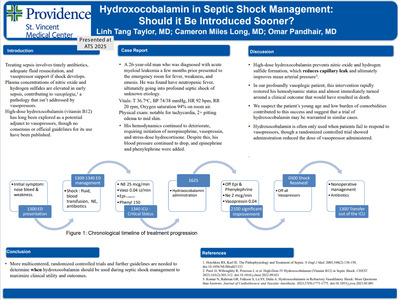
Introduction: Treating sepsis involves timely antibiotics, adequate fluid resuscitation, and vasopressor support if shock develops. Plasma concentrations of nitric oxide and hydrogen sulfides are elevated in early sepsis, contributing to vasoplegia,1 a pathology that isn’t addressed by vasopressors. High-dose hydroxocobalamin (vitamin B12) does, and therefore, has long been explored as a potential adjunct to vasopressors, though no consensus or official guidelines for its use have been published. Case Report: A 26-year-old man who was diagnosed with acute myeloid leukemia a few months prior presented to the emergency room for fever, weakness, and emesis. He was found to be profoundly hypotensive and was treated with aggressive fluid resuscitation and broad-spectrum antibiotics. His hemodynamics continued to deteriorate, requiring initiation of norepinephrine, vasopressin, and stress-dose hydrocortisone. Despite this, his mean arterial pressure continued to drop, and epinephrine and phenylephrine were added, with fleeting benefits. Ultimately, 5 g of hydroxocobalamin was administered intravenously. Within a few hours, vasopressor doses were able to be reduced significantly, and he was stable enough for abdominal imaging, which showed a perforated sigmoid colon abscess. Surgical intervention was deferred due to the extremely high risk of morbidity and death due to profound pancytopenia and the severity of septic shock. Within 15 hours, his shock improved with down titration of all vasopressors and normalization of lactate levels. He was transferred out of the ICU 21 hours after hydroxocobalamin administration and discharged home a week later Discussion: High-dose hydroxocobalamin prevents nitric oxide and hydrogen sulfide formation, which reduces capillary leak and ultimately improves mean arterial pressure3 . In our profoundly vasoplegic patient, this intervention rapidly restored his hemodynamic status and almost immediately turned around a clinical outcome that most likely would have resulted in death. We suspect the patient’s young age and low burden of comorbidities contributed to this success and suggest that a trial of hydroxocobalamin may be warranted in similar cases. Hydroxocobalamin is often only used when patients fail to respond to vasopressors, though a randomized controlled trial showed administration reduced the dose of vasopressor administered2 . More multicentered, randomized controlled trials and further guidelines are needed to determine when hydroxocobalamin should be used during septic shock management to maximize clinical utility and outcomes.
-

The Power of Two Questions: A Simplified Approach to Delirium Detection
Dalton VanderPol, MD; Laura Perry; and Shelley Schoepflin Sanders
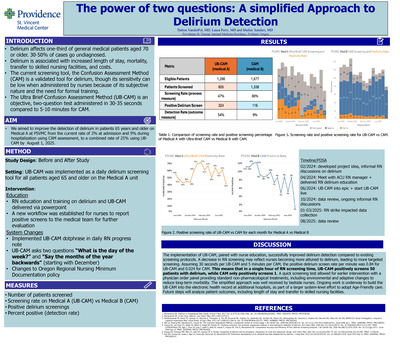
Background: Delirium affects one-third of general medical patients aged 70 or older. Patients with older age, preexisting dementia, or cognitive impairment are at increased risk of developing delirium. Delirium is associated with increased length of stay, mortality, transfer to skilled nursing facilities, and costs. Although the Confusion Assessment Method (CAM) is a validated tool for delirium, its sensitivity can be low when administered by nurses because of its subjective nature and the need for formal training. The Ultra Brief Confusion Assessment Method (UB-CAM) is an objective, two-question test administered in 30-35 seconds compared to 5-10 minutes for CAM. The objective was to increase the combined delirium detection rate from 12% to 25% by July 1, 2025. Methods: The UB-CAM was implemented as a daily delirium screening tool for all patients aged 65 and older on the Medical A unit. Nurses on Medical A received training on delirium recognition and the proper use of the UB-CAM. A new workflow was established for nurses to report positive screens to the medical team for further evaluation. The primary outcome was measured by the percentage of patients on Medical A who had a positive delirium screen, which was assessed at admission and daily by RNs using the UB-CAM. Results: 605 adults aged 65 and over were screened out of 1,286 eligible for a screening rate of 47%. The UB-CAM combined positive rate on Medical A from June 2024 to July 1, 2025, was 54% (324/605). On a comparable unit (Medical B) during the same time, 1338 adults age 65 and over were screened with the CAM out of 1,677 eligible for a screening rate of 80%. Of those screened, 9% (116/1338) screened positive. Conclusion: The implementation of UB-CAM, paired with nurse education, successfully improved delirium detection compared to existing screening protocols. A decrease in RN screening may reflect nurses becoming more attuned to delirium, leading to more targeted screening. Assuming 30 seconds per UB-CAM and 5 minutes per CAM, the positive delirium screen rate per minute was 0.84 for UB-CAM and 0.024 for CAM. This means that in a single hour of RN screening time, UB-CAM positively screens 50 patients with delirium, while CAM only positively screens 1. A quick screening test allowed for earlier intervention with a physician order panel providing standard non-pharmacological treatments, including environmental and adaptive changes to reduce long-term morbidity. The simplified approach was well received by bedside nurses. Ongoing work is underway to build the UB-CAM into the electronic health record at four additional units at two hospitals, as part of a larger system-level effort to adopt Age-Friendly care. Future steps will analyze patient outcomes, including length of stay and transfer to skilled nursing facilities.
-
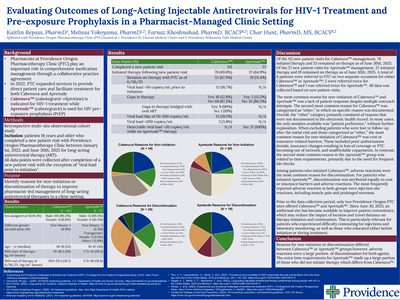
Evaluation of patient outcomes after implementation of remdesivir restriction criteria
Evonie Claire Villarete, PharmD; Emily Fox, PharmD, BCIDP; and Gregory B. Tallman, PharmD, BCPS, BC
Abstract: Remdesivir has demonstrated inconsistent clinical benefit in randomized trials, with the greatest efficacy observed in hospitalized patients requiring low-flow oxygen and no clear mortality benefit in patients requiring invasive mechanical ventilation. In the era of widespread SARS-CoV-2 immunity, evolving viral variants, and reduced disease severity, the role of routine remdesivir use remains uncertain. Continued prescribing may expose patients to unnecessary therapy, prolong hospitalization, and increase healthcare costs without clear incremental benefit. In June 2025, Providence Oregon hospitals implemented restriction criteria limiting remdesivir use to selected high-risk populations, including elderly, immunocompromised, or critically ill patients presenting within seven days of symptom onset. The purpose of this study is to evaluate the clinical and financial impact of implementing remdesivir restriction criteria across Providence Oregon hospitals. This study is a multi-center retrospective cohort analysis of adult patients hospitalized with nasopharyngeal PCR confirmed SARS-CoV-2 identified through the electronic medical record. Patients hospitalized at one of eight Providence Oregon hospitals between July 15, 2024 and October 15, 2024 (pre-restriction period) and July 15, 2025 and October 15, 2025 (post restriction period) were included to allow comparison of outcomes before and after the intervention. Demographic, clinical, and treatment data were collected through chart review. Variables collected include age, sex, body mass index, race or ethnicity, oxygen saturation, oxygen device, baseline vital signs, immunocompromised status, comorbidities, days from symptom onset, intensive care unit admission status, medications (corticosteroids, remdesivir, and antibiotics), vaccination status, prior SARS-CoV-2 infection, and presence of sepsis at admission. The primary outcome is the need for supplemental oxygen or escalation in home oxygen therapy requirements. Secondary outcomes include hospital length of stay, intensive care unit admission, mechanical ventilation, 30-day readmission, in-hospital mortality, adherence to the restriction policy, and financial impact associated with remdesivir utilization. Continuous variables will be analyzed using Student’s t-test or Mann-Whitney U test, and categorical variables will be analyzed using chi-square or Fisher’s exact tests as appropriate. Results and conclusions will be shared when the project is completed. (IRB exempt) Learning Objective: Assess the clinical and financial impact of recently implemented remdesivir restriction criteria. Presentation Category: Infectious Diseases
-

Increasing Structured Inpatient Teaching in a Family Medicine Residency
Eric Waelbroeck and MH Choe
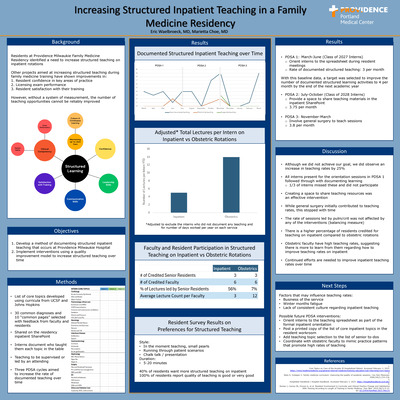
Background: What is not measured cannot be improved. Residents at Providence Milwaukie Family Medicine Residency identified a need to increase structured teaching on inpatient rotations. Other projects aimed at increasing structured teaching during family medicine training have demonstrated improvements in resident confidence in key areas of practice, licensing exam performance, and resident satisfaction with their training. However, without a system of measurement, the number of teaching opportunities cannot be reliably improved. Objectives: Develop a method of documenting structured inpatient teaching that occurs at Providence Milwaukie Hospital. Then, implement interventions using a quality improvement model to increase structured teaching over time. Methods: A list of inpatient topics was developed referencing inpatient curricula from UCSF and Johns Hopkins. This list was narrowed down to 30 common admitting diagnoses and 10 “common pages” using feedback from the residency inpatient committee. A table was shared on the residency inpatient SharePoint where interns could document who taught them each topic. Then, three PDSA cycles each lasting 4 months aimed to increase the rate of documented teaching over time. Results: The baseline rate of intern-documented structured learning activities during inpatient rotations over the final 4 months of the class of 2027 intern year was 3 per month. This includes the first PDSA, where interns were oriented to the spreadsheet during resident meetings. With this baseline data, a target was selected to improve the number of documented structured learning activities to 4 per month by the end of the subsequent academic year. After providing a space to share teaching materials in the SharePoint, the rate of teaching for the first 4 months of the class of 2028 intern year increased to 3.75 per month. After asking general surgery to teach sessions, the rate of teaching for the subsequent 4 months remained stable at 3.8 per month. Discussion/Conclusions/Next Steps: This project was successful in producing a method of documenting structured inpatient teaching that interns receive in a family medicine residency. Quality improvement efforts were successful in generating a ~25% increase in teaching rates, with the most effective intervention being sharing a space for teaching resources. Comparing adjusted teaching rates on inpatient to obstetric rotations demonstrates a continued discrepancy (5.5 vs 14 per month). This highlights the imbalance that residents experience in their education and reaffirms the need for continued efforts at improving structured learning in the inpatient setting. Future efforts could consider posting the list of teaching topics in the resident workroom, adding teaching topic selection to the list of to-dos on the senior inpatient guide, and engaging faculty to improve teaching rates.
-

A Fatal ‘Sepsis’: Intravascular Large B-Cell Lymphoma in Disguise
Jennifer L. Wong, DO1; Jared A. Shipley, MD2; and Christine Johnson, MD3
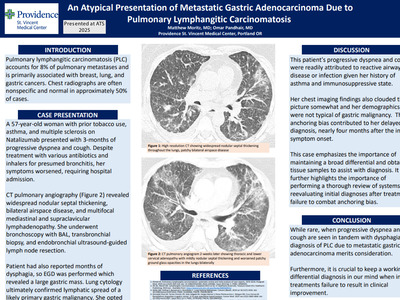
Introduction: Intravascular large B-cell lymphoma (IVLBCL) is a rare, aggressive subtype of non-Hodgkin lymphoma characterized by selective proliferation of neoplastic cells within small vessel lumina. Cases in Western countries more commonly involve the central nervous system or skin, whereas patients in Eastern regions often present with hemophagocytic syndrome or medullary disease. The absence of lymphadenopathy, low circulating tumor burden, and subtlety of morphologic clues contribute to delays in diagnosis. By presentation, most have advanced disease, and a substantial proportion are diagnosed only at autopsy. We report a unique case with mixed features who manifested respiratory involvement and ultimately suffered cardiovascular collapse. Case Presentation: A 55-year-old man with six months of fatigue and unintentional weight loss presented with progressive dyspnea and cough. Laboratory results revealed mild thrombocytopenia with elevated D-dimer, but imaging was negative for pulmonary embolism. There were ground-glass opacities concerning for early pneumonia and splenomegaly up to 17 cm. He tested positive for COVID, received fluids, and was discharged from the Emergency Department. His symptoms worsened with associated fevers and altered mentation, prompting hospital admission two weeks later. He was treated for sepsis of unclear source with empiric antibiotics and steroids without improvement. Follow up imaging showed further enlargement of the spleen to 24 cm, now with wedge-shaped parenchymal hypodensity consistent with infarct, but no significant lymphadenopathy. He acutely decompensated with escalating oxygen needs and was transferred to the intensive care unit, where he suffered a PEA cardiac arrest. He died despite prolonged resuscitative efforts. Autopsy revealed a markedly enlarged spleen, weighing 3 kg, ten times the size of normal. Immunohistochemistry demonstrated diffuse large B-cell lymphoma with extensive intravascular involvement across sampled organs, presumably causing respiratory failure through pulmonary vascular infiltration. Discussion: This case highlights how IVLBCL may mimic a routine infectious pulmonary process with unrevealing early diagnostics. Rapid clinical decline and lack of an optimal biopsy target make timely diagnosis and therapy difficult. Cutaneous variants grant an earlier opportunity for biopsy and therefore carry a better prognosis, but diagnosis can still often be delayed. Therefore, in patients with splenomegaly without localized lymphadenopathy and lack of response to standard infectious therapies, suspicion should be raised for an underlying hematologic malignancy.
-

When Jaundice Isn’t Just the Liver’s Fault: A Chilly Case of Cold Autoimmune Hemolytic Anemia
Jennifer Wong, DO and Shahana Baig-Lewis, MD, MPH
Introduction: Cold agglutinin disease (CAD), a subtype of autoimmune hemolytic anemia (AIHA), is characterized by IgM autoantibodies that target red blood cell antigens at low temperatures, leading to agglutination in cooler peripheral tissues and hemolysis. Predominately directed against the “I” or “i” antigens, cold agglutinins are commonly associated with Mycoplasma pneumoniae and infectious mononucleosis. Distinguishing warm AIHA from CAD can be challenging. Definitive diagnosis relies on antibody testing, with warm AIHA primarily involving IgG and CAD involving IgM. We report a case of CAD initially misattributed to drug-induced liver injury in the setting of a viral upper respiratory infection. Case Presentation: A 39-year-old woman with no significant past medical history presented with acute weakness and fevers. Symptoms were initially attributed to a viral illness and self-treated with Acetaminophen and Ibuprofen, achieving only partial relief. She visited her primary care provider the day prior to admission with new onset dark urine and jaundice. Concern for acute hepatitis prompted referral to the emergency department (ED). Initial evaluation revealed marked hyperbilirubinemia, elevated transaminases, and an echogenic liver on ultrasound, suggestive of fatty infiltration or chronic hepatocellular disease. She was admitted with presumed acetaminophen-induced acute hepatitis. Concurrently, a 4.6 g/dL drop in hemoglobin and positive antibody screen (Direct antiglobulin testing (DAT) positive for both IgG and C3), led to presumptive diagnosis of warm AIHA. Further workup revealed Epstein-Barr virus infection, confirming CAD. She was managed with supportive measures, counseled on avoidance of cold exposure, and discharged with close hematology follow-up. Discussion: CAD accounts for 20–25% of AIHA cases and may present insidiously or acutely in association with infections. Primary management includes avoidance of cold exposure, warming of intravenous fluids and transfusions, and treatment of underlying triggers. In severe cases, plasmapheresis may provide temporary benefit, and Rituximab-containing regimens are considered for primary CAD. This case highlights how initial anchoring to a presumed diagnosis of acute hepatitis delayed recognition of hemolysis. Cognitive biases—including premature closure, authority bias, framing bias, and availability bias—contributed to the initial misdiagnosis. Detailed history, attention to evolving data, and re-evaluation of the working diagnosis were essential in identifying CAD and implementing appropriate management.
-

Eosinophilic Fasciitis Masquerading as Myositis: A Diagnostic Challenge
Jennifer L. Wong, DO; Elizabeth S. Ballner, DO; and Mary Elizabeth Swift-Taylor
Introduction: Eosinophilic fasciitis (EF), or Shulman’s disease, is a rare disorder of unknown etiology and poorly understood pathogenesis. It is characterized by fibroblast activation and interleukin-driven eosinophilia. Early clinical features include limb or trunk erythema, non-pitting edema, and progressive fascial thickening, often producing an “orange peel” appearance. Eosinophilia is a prominent laboratory finding in the early phase, but diagnosis often requires a full-thickness skin-to-muscle biopsy. Systemic corticosteroids are first-line therapy, with methotrexate as the steroid -sparing agent for refractory disease. We present a unique and diagnostically challenging case of EF confirmed by histopathology. Case Presentation: A 56-year-old man presented with two-months of progressive right forearm pain, edema, and erythema refractory to conservative therapy and empiric antibiotics for presumed cellulitis. An outpatient ultrasound excluded deep vein thrombosis (DVT) and worsening symptoms prompted hospital admission. Examination revealed non-pitting edema and induration of the right forearm; inflammatory markers were normal and mild peripheral eosinophilia (1.5 times the upper limit of normal) was noted. CT showed diffuse subcutaneous edema along the volar aspect of his right forearm. Necrotizing fasciitis and compartment syndrome were considered but deemed unlikely given benign clinical findings by General and Orthopedic Surgery. His workup included evaluation for myositis, eosinophilic fasciitis, and scleroderma, among other diagnoses. MRI demonstrated fascial edema and thickening, resulting in a muscle biopsy and single compartment fasciotomy with evidence of immediate bulging of healthy underlying muscle tissue. Histology showed dense mixed inflammation in perimysial connective tissue with prominent eosinophils, confirming EF. Lastly, his myositis panel returned positive for PM-SCL antibodies. The patient improved on a prednisone taper and was discharged with close Rheumatology follow-up. Discussion: Though the etiology of EF is unknown, it is associated with triggers such as strenuous exercise, infections, autoimmune diseases, medications, and physical stressors. Autoimmune thyroid disease, Sjogren’s, lupus, rheumatoid arthritis, and scleroderma are the most associated autoimmune diseases to EF. Cutaneous involvement, neuropathies, and myalgias are common, though visceral involvement and arthropathies may occur. Laboratory findings typically include early peripheral eosinophilia, elevated inflammatory markers, and polyclonal hypergammaglobuline mia. This case highlights EF’s ability to mimic urgent, localized limb etiologies including cellulitis, DVTs, necrotizing fasciitis, and compartment syndrome. Additional etiologies should be considered when symptoms persist despite standard management, including rare rheumatologic causes. Detailed history, attention to evolving data, and iterative diagnostic reassessment were essential in the management of this complex rare condition.
-

Cloudy Consequences: Exploring Vaping-Induced Pulmonary Alveolar Proteinosis
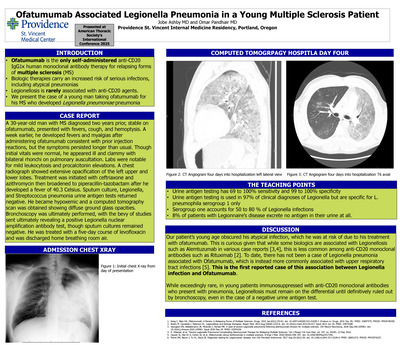
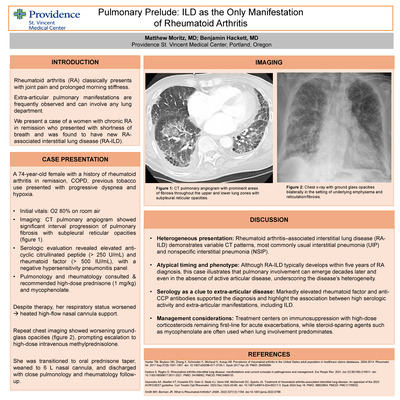
Jennifer Wong, DO; Omar Pandhair; Abby Lindseth, MD; and Cameron Miles Long, MD
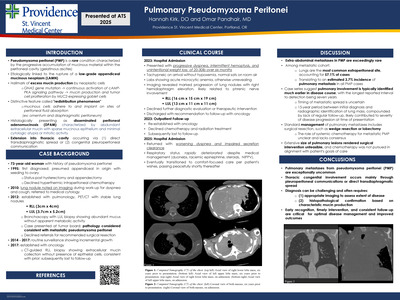
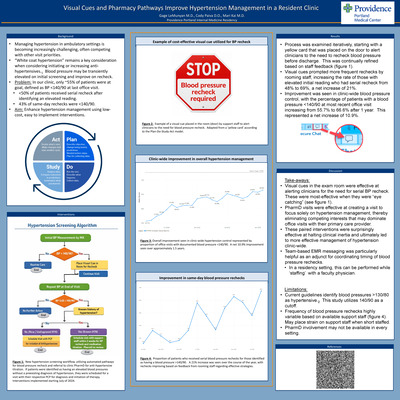
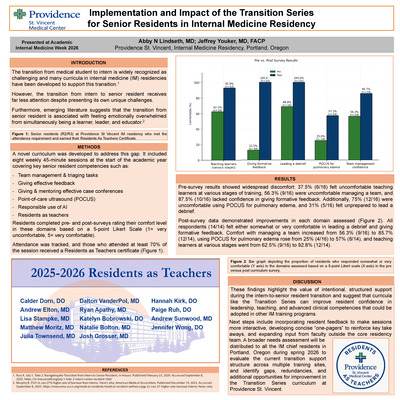
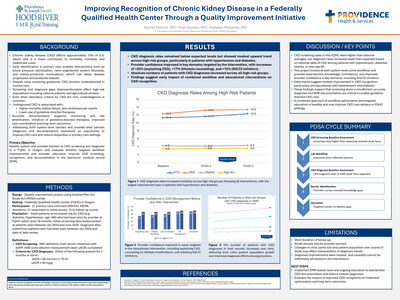
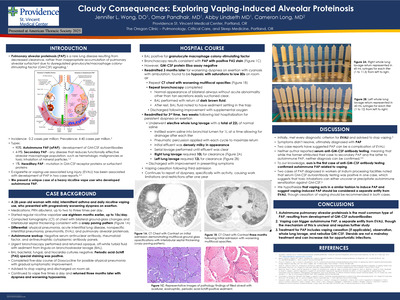
Abstract: Pulmonary alveolar proteinosis (PAP) is a rare disease caused by abnormal accumulation of surfactant within alveoli. Vaping of electronic cigarette smoke has recently been described as a cause of pulmonary alveolar proteinosis in two case reports. We add to this rare literature by describing a case of pulmonary alveolar proteinosis induced from vaping in a young woman with confirmed granulocyte/macrophage colony-stimulating factor (GM-CSF) autoantibodies as the proposed mechanism. Introduction: Pulmonary alveolar proteinosis (PAP) results from inappropriate accumulation of pulmonary alveolar surfactant due to dysregulated granulocyte/ macrophage colony-stimulating factor (GM-CSF) signaling.1 Its incidence is approximately 0.2 cases per million with a prevalence between 4 and 40 cases per million.2 Autoimmune PAP (aPAP) due to development of anti-GM-CSF antibodies accounts for 90% of cases and the remaining 10% arise mainly from secondary causes such as hematologic malignancies or toxic inhalation of mineral particles.1,2 E-cigarette or vaping-use associated lung injury (EVALI) has been associated with development of PAP in two case reports.3,4 We present a unique case of a heavy nicotine vape user who developed autoimmune PAP. Case Presentation: A 28-year-old woman with mild, intermittent asthma presented to emergency department with subacute cough, dyspnea, and mild hypoxemia. Eighteen months earlier, she began regularly using a nicotine vaporizer fifteen times daily. She was mildly tachycardic with diffuse crackles on pulmonary auscultation. A computed tomography (CT) scan of the chest revealed bilateral ground-glass changes and interlobular septal thickening consistent with a crazy paving pattern (Fig. 1A). The initial differential diagnosis included atypical pneumonia, acute interstitial lung disease, pneumonitis, EVALI, and pulmonary alveolar proteinosis. Autoimmune workup including serum antinuclear antibody, rheumatoid factor, and antineutrophilic cytoplasmic antibody panels were negative. Urgent bronchoscopy was performed and was notable for the return of opaque, off-white fluid on bronchoalveolar lavage (BAL). While BAL bacterial, fungal, and Nocardia cultures returned negative, periodic acid-Schiff (PAS) special staining was positive. She finished a five-day course of Doxycycline for possible atypical pneumonia with gradual symptomatic improvement. She was advised to stop vaping and discharged on room air. The patient continued to vape five times a day and returned three months later with dyspnea and worsening hypoxemia. A repeat CT scan showed worsening multifocal opacities and increased septal thickening (Fig. 1B). She underwent repeat BAL and transbronchial biopsy with pathology and cytology confirming the diagnosis of PAP. Serum GM-CSF was low (Mayo Clinic Laboratories) and serum anti-GM-CSF autoantibodies (National Jewish Laboratories) returned elevated, consistent with autoimmune PAP. She was discharged on supplemental oxygen with exertion and underwent whole lung lavage two weeks later. The lungs were sequentially lavaged (right then left) with 0.9% warm saline (37 degrees Celsius) 1 L at time and allowing gravity to drain. Drainage was aided by a manual chest percussion device. The right lung was lavaged with 12 L and the left lung was lavage with 11.5 L. The lavage effluent progressively became more translucent with each lavage for both lungs (Fig. 2). She was monitored in the ICU overnight and discharged the next morning. Discussion: Initially, our patient met every diagnostic criterion for EVALI and was advised to stop vaping.5 Her symptoms did not resolve and she was ultimately diagnosed with PAP. Two case reports have suggested PAP can be a complication of EVALI. Unfortunately, neither author reported serum anti-GM-CSF antibody testing (National Jewish Laboratories), meaning that while the former attributed their case to secondary PAP and the latter to autoimmune PAP, neither diagnosis can be confirmed.3,4 Israel, AK et.al. 2020 suggested that vape inhalation acts like a toxic inhalation causing direct damage to macrophages, while Chua, TH et. al. 2021 posited that “vaping products ... incite self-reactivity,” to trigger aPAP. To our knowledge, ours is the first case of anti-GM-CSF antibody testing confirmed autoimmune PAP related to vaping. Interestingly, two cases of PAP diagnosed in workers at indium processing facilities noted that serum GM-CSF autoantibody testing was positive in one case, which suggests that toxic inhalations can either uncover or precipitate autoimmune sensitization against GM-CSF.6 We hypothesize that vaping acts in a similar fashion to induce PAP and suggest vaping-induced PAP should be considered a separate entity from EVALI, though cessation of vaping should be recommended in both cases. Treatment for PAP can involve observation, whole lung lavage, and nebulized GM-CSF.7 Steroids have not been proven effective and can increase the risk of opportunistic infections. Given the patient’s initial improvement, vaping cessation alone was recommended. A steroid trial was considered as it seemed possible that she could have both EVALI and pulmonary alveolar proteinosis, but this was not initiated. The patient continued to vape and had further deterioration of her lung function which ultimately led to the whole lung lavage. The patient stopped vaping after the whole lung lavage and was started on nebulized GM-CSF.
-

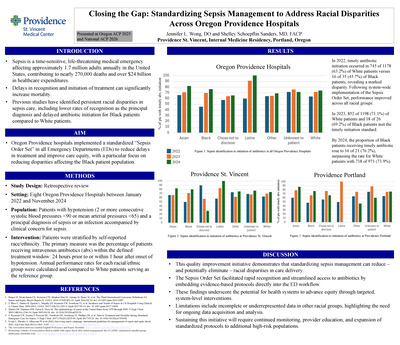
Closing the Gap: Standardizing Sepsis Management to Address Racial Disparities Across Oregon Providence Hospitals
Jennifer Wong, DO and Shelley Schoepflin Sanders, MD, FACP
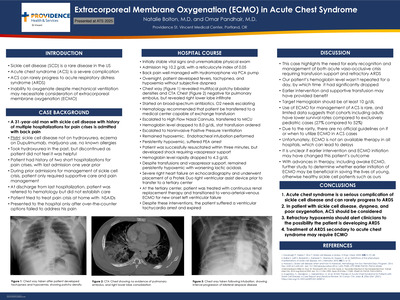
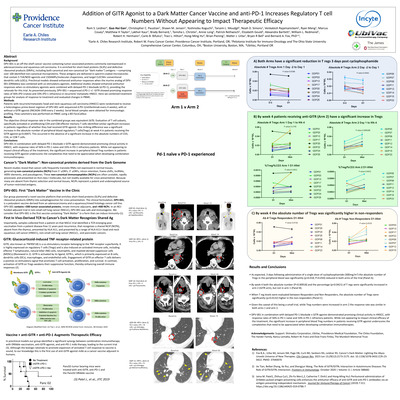
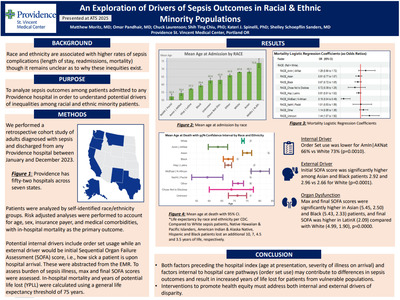
Introduction: Sepsis is a time-sensitive, life-threatening medical emergency affecting approximately 1.7 million adults annually in the United States, contributing to nearly 270,000 deaths and over $24 billion in healthcare expenditures. Delays in recognition and initiation of treatment can significantly increase mortality. Previous studies have identified persistent racial disparities in sepsis care, including lower rates of recognition as the principal diagnosis and delayed antibiotic initiation for Black patients compared with White patients. In alignment with Providence’s mission to provide compassionate, equitable care, Oregon Providence hospitals implemented a standardized “Sepsis Order Set” in all Emergency Departments (ED) to reduce treatment delays and improve care equity, with a particular focus on reducing disparities affecting the Black patient population. Methods: A retrospective review was conducted using ED encounter data from eight Oregon Providence hospitals between January 2022 and November 2024. Eligible encounters included patients with a principal diagnosis of sepsis or an infection accompanied by clinical concern for sepsis. Patients were stratified by self reported race/ethnicity. The primary measure was the percentage of patients receiving intravenous (IV) antibiotics within the defined timely treatment window: 24 hours prior to or within 1 hour after onset of hypotension. Annual performance rates for each racial/ethnic group were calculated and compared, with White patients serving as the reference group. Results: In 2022, timely antibiotic initiation occurred in 63.2% of White patients versus 45.7% of Black patients, revealing a marked disparity. Following system wide implementation of the Sepsis Order Set, performance improved across all racial groups. In 2023, 71.1% of White patients and 69.2% of Black patients met the timely initiation standard. By 2024, the proportion of Black patients receiving timely antibiotics rose to 76.2%, surpassing the rate for White patients, 73.9%. Discussion: This quality improvement initiative demonstrates that standardizing sepsis management can reduce—and potentially eliminate—racial disparities in care delivery. The Sepsis Order Set facilitated rapid recognition and streamlined delivery of antibiotics by embedding evidence-based protocols directly into the ED workflow. These findings underscore the potential for health systems to advance equity through targeted, system-level interventions. Limitations include incomplete or underrepresented data for Latinx and “Other” racial groups, highlighting the need for ongoing data quality improvement and further analysis. Sustaining these gains will require continued monitoring, provider education, and expansion of standardized protocols to additional high-risk populations.
-
Assessment of medication adherence and clinical outcomes in diabetes patients After enrollment in a health-system medication assistance program
Joshua Wood, PharmD
Background: Prescription drug cost prices have continued to rise in recent years, putting patients under significant financial pressure. This can result in patients with limited resources being unable to access and afford life-saving medications. Despite the growing need for financial assistance, most health systems do not offer a coordinated medication assistance service to patients. Patients, in these cases, are often forced to “go it alone.” However, accessing drug manufacturer assistance programs requires knowledge about which drugs have assistance programs available, the manufacturers involved, and qualification requirements. In addition, eligibility requirements may differ from one manufacturer to another and can change with little forewarning. The entire process can be very overwhelming for patients who may be sick, elderly, or confused about how to identify what resources are available to them. In response to these challenges, our health-system medication assistance program (MAP) was developed to help patients obtain much needed medication at little to no cost. Our MAP service helps alleviate the financial burden of patients who are struggling to afford their medications due to limited insurance coverage, high copayments, or other financial constraints, thereby playing a critical role in the healthcare safety net. In the case of diabetic patients, our MAP service allows patients, who otherwise cannot afford insulins, GLP-1 agonists, and SLGT-2 inhibitors, access to these medications. This can provide cost savings, increased adherence, and better patient outcomes--saving patients thousands of dollars a year in addition to the glycemic control these medications can provide. Objective: To track adherence and clinical outcomes for diabetes patients enrolled in our MAP program Methods: A retrospective cohort analysis of patients with diabetes was performed for patients enrolled in our health-system MAP program (on MAP medications: insulins, GLP1s, SGLT2s) versus patients who filled antihyperglycemic medication prescriptions before receiving MAP assistance. Modified medication possession ratios (mMPR) were calculated for patients using insulin fill history data to assess adherence. Glycemic control was determined through comparison of A1c values in the electronic health record (EHR) before and after MAP enrollment to assess clinical outcomes. Results: Data analysis for this study is ongoing. ConclusionData analysis for this study is ongoing.
-
Analysis of Hospital Readmission among PACE Participants in Oregon
Hanna Yoon, PharmD; Sharon Leigh, PharmD, BCPS; and Alyson Bell, PharmD
Introduction: Older adults face an elevated risk of hospitalization-associated harms, including falls, cognitive decline, and functional loss. Unplanned readmissions affect 15%–30% of Medicare beneficiaries annually and contribute an estimated $12 billion in potentially preventable costs. For programs of All-Inclusive Care for the Elderly (PACE), understanding factors that contribute to repeat or medication-related hospitalizations is critical for improving patient care, and informing pharmacist-led interventions aimed at reducing avoidable admissions. Objective: This project seeks to identify trends and potentially preventable causes of hospital readmissions among PACE participants and to evaluate opportunities for targeted interventions. Methods: A retrospective chart review was conducted using data from EPIC and PACE internal systems. The study included Oregon PACE participants with more than one hospitalization between January 1 and December 31, 2024. Hospitalizations occurring before PACE enrollment and elective admissions were excluded. Results: A total of 583 admissions involving patients more than one hospitalization were initially identified. After applying exclusion criteria, 449 admissions among 160 patients were included. The mean age was 74 years, 107 (66.9%) were female, 63 (39.4%) resided in adult family homes, and 16 (10.0%) were receiving palliative care. Urinary tract infection was the most common discharge diagnosis (75 admissions, 16.7%), followed by heart failure (61 admissions, 13.6%). Medication-related causes accounted for 56 admissions (12.5%), most frequently involving central nervous system agents (16 admissions, 28.6%) and opioids (10 admissions, 17.9%). Admissions were evenly distributed by month with an average of 37 admissions per month; July had the highest number (45). Among the 449 admissions, 29 (6.5%) involved a fall prior to admission, 113 (25.2%) were 30-day readmissions, and 326 (72.6%) had at least one PACE encounter within 3 days prior to admission. The estimated total cost of hospitalization for these admissions was $7,237,500. Conclusion: Pharmacist-led interventions targeting urinary tract infection prevention, central nerve system medication optimization, and close follow-up may reduce preventable readmissions in PACE participants.
-
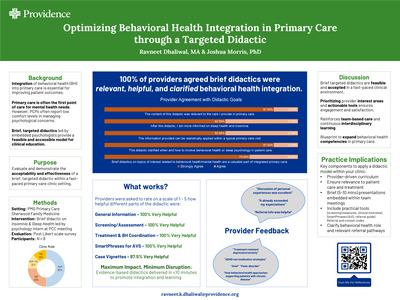
Developing an Adaptable Intake Form for the Lifespan to Optimize Efficiency of The Initial Behavioral Health Session in Primary Care
Helen Youssef, MA
Behavioral health intake forms play a key role in collecting background information necessary for comprehensive assessment and successful treatment planning. However, at Providence Gateway Family Medicine, a standardized behavioral health intake form is not currently in use because available forms are not developmentally appropriate for child populations and do not adequately capture developmental information for children and adolescents. As a result, clinicians rely on in‑session questioning to obtain essential background details, which may limit efficiency and reduce the time available to address presenting concerns. This quality improvement project seeks to address this gap via adapting a behavioral health intake form to be effective across the lifespan, with particular attention to the needs of children and adolescents. The revised intake form includes an additional section that further explores child development, school status, and family dynamics. The goal is to create a standardized intake tool that supports both behavioral health providers in delivering developmentally informed patient care. To evaluate the adapted intake form, two behavioral health clinicians at the Providence Gateway Family Medicine clinic will pilot it during new intake sessions with patients aged 17 years or younger. The clinicians will evaluate the form's productivity and clinical effectiveness. That evaluation will consider the intake form’s usefulness in gathering pertinent background information, its impact on session efficiency, and its ability to support meaningful clinical discussions. The clinicians' feedback will guide evaluation of the form’s effectiveness and inform possible improvements prior to wider implementation. This project aims to improve the intake workflow, enhance cross-disciplinary collaboration, and support high‑quality behavioral health care for children and families at the Gateway clinic.
-

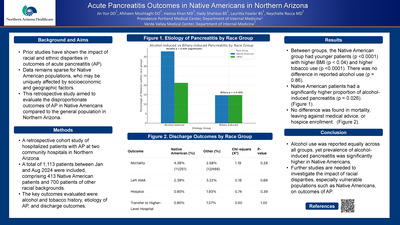
Acute Pancreatitis Outcomes in Native Americans in Northern Arizona
Jin Yun DO1; Afsheen Moshtaghi DO2; Hamza Khan, MD2; Hady Shahbaz BS2; Yoshinobu Koguchi; Tarsem L. Moudgil; Noah D. Simons; and Venkatesh Rajamanickam
Background and Aims: Prior studies have shown the impact of racial and ethnic disparities in outcomes of acute pancreatitis (AP). Data remains sparse for Native American populations, who may be uniquely affected by socioeconomic and geographic factors. This retrospective study aimed to evaluate the disproportionate outcomes of AP in Native Americans compared to the general population in Northern Arizona. Methods: A retrospective cohort study of hospitalized patients with AP at two community hospitals in Northern Arizona. A total of 1,113 patients between Jan and Aug 2024 were included, comprising 413 Native American patients and 700 patients of other racial backgrounds. The key outcomes evaluated were alcohol and tobacco history, etiology of AP, and discharge outcomes. Results: Between groups, the Native American group had younger patients (p < 0.0001) with higher BMI (p < 0.04) and higher tobacco use (p < 0.0001). There was no difference in reported alcohol use (p = 0.86). Native American patients had a significantly higher proportion of alcohol-induced pancreatitis (p = 0.026). No difference was found in mortality, leaving against medical advice, or hospice enrollment. Conclusion: Alcohol use was reported equally across all groups, yet prevalence of alcohol-induced pancreatitis was significantly higher in Native Americans. Further studies are needed to investigate the impact of racial disparities, especially vulnerable populations such as Native Americans, on outcomes of AP.
-

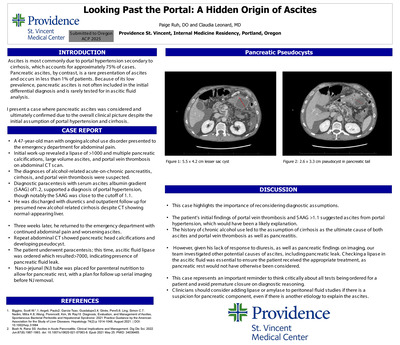
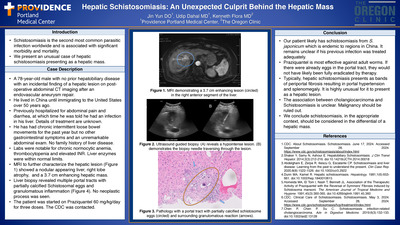
Hepatic Schistosomiasis: An Unexpected Culprit Behind the Hepatic Mass
Jin Yun DO; Udip Dahal MD; and Kenneth Flora, MD
Introduction: Schistosomiasis is the second most common parasitic infection worldwide and is associated with significant morbidity and mortality. We present an unusual case of hepatic schistosomiasis presenting as a hepatic mass. Case Description: A 78-year-old male with no prior hepatobiliary disease with an incidental finding of a hepatic lesion on postoperative abdominal CT imaging after an endovascular aneurysm repair. He lived in China until immigrating to the United States over 50 years ago. Previously hospitalized for abdominal pain and diarrhea, at which time he was told he had an infection in his liver. Details of treatment are unknown. He has had chronic intermittent loose bowel movements for the past year but no other gastrointestinal symptoms and an unremarkable abdominal exam. No family history of liver disease. Labs were notable for chronic normocytic anemia, thrombocytopenia and elevated INR. Liver enzymes were within normal limits. MRI to further characterize the hepatic lesion showed a nodular appearing liver, right lobe atrophy, and a 3.7 cm enhancing hepatic mass. Liver biopsy revealed multiple portal tracts with partially calcified Schistosomal eggs and granulomatous inflammation. No Neoplastic process was seen. The patient was started on Praziquantel 60 mg/kg/ day for three doses. The CDC was contacted. Conclusion: Our patient likely has schistosomiasis from S. japonicum which is endemic to regions in China. It remains unclear if his previous infection was treated adequately. Praziquantel is most effective against adult worms. If there were already eggs in the portal tract, they would not have likely been fully eradicated by therapy. Typically, hepatic schistosomiasis presents as bands of periportal fibrosis resulting in portal hypertension and splenomegaly. It is highly unusual for it to present as a hepatic lesion. The association between cholangiocarcinoma and Schistosomiasis is unclear. Malignancy should be ruled out. We conclude schistosomiasis, in the appropriate context, should be considered in the differential of a hepatic mass.
-
Suicide Risk Assessment and Safety Planning: Exploring Provider Perceptions of a New Suicide Screening Process in a Pediatric Healthcare Setting
Darcy Gist Zornes, PsyD and Tyson Payne, PsyD
In the United States, suicide is the 2nd leading cause of death for youth ages 10 to 24, and suicide attempts and suicidal thoughts are even more common. Early detection is key to prevention, and given that the majority of people who die by suicide visit a healthcare provider months before their death, healthcare settings play an important role in early detection and prevention efforts. In 2026, Providence Children's Development Program introduced a suicide risk screening process to help identify youth who are at risk for suicide and to systematically guide providers in supporting youth and their families through safety planning and crisis interventions. The present project will explore provider perceptions of this new suicide screening protocol with the aims of (1) identifying strengths and limitations of the current workflow and (2) informing potential changes for improvement as well as applications for adaptation to other pediatric healthcare settings
-

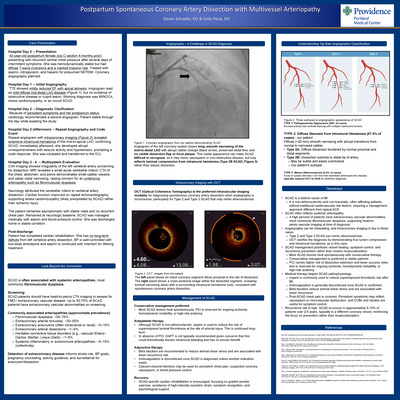
Intratracheal Lidocaine and Postoperative Sore Throat at Providence Sacred Heart Medical Center and Providence Holy Family Hospital
Jennifer Cowgill, Scot Pettey, and Kenn B Daratha
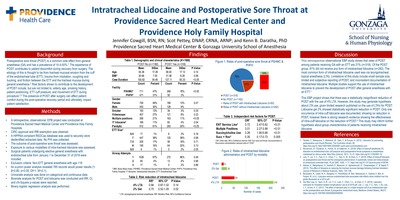
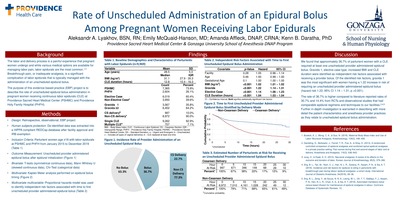
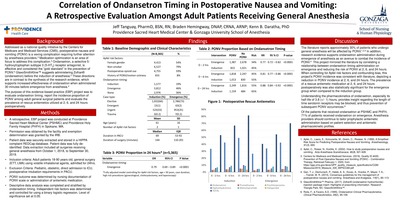
Background Postoperative sore throat (POST) is a common side effect from general anesthesia (GA) and has a prevalence of 14.4-50%.1 The experience of POST contributes to patient discomfort during recovery from surgery. The etiology of this is thought to be from tracheal mucosal erosion from the cuff of the endotracheal tube (ETT), trauma from intubation, coughing and bucking, and friction between the ETT and the tracheal mucosa during general anesthesia.2 Risk factors shown to contribute to the development of POST include, but are not limited to, elderly age, smoking history, patient positioning, ETT cuff pressure, and movement of ETT during procedure.2,3 The presence of POST after surgery can affect patient comfort during the post-operative recovery period and ultimately, impact patient satisfaction.
Methods • A retrospective, observational, EPB project was conducted at Providence Sacred Heart Medical Center and Providence Holy Family Hospitals. • CIRC approval and IRB exemption was obtained. • A HIPPAA compliant REDCap database was used to securely store deidentified extracted data. No PHI was collected. • The outcome of post-operative sore throat was assessed. • Exposure to various modalities of intra-tracheal lidocaine was assessed. • Surgical patients undergoing elective general anesthesia with endotracheal tube from January 1 to December 31 of 2019 were included. • Exclusion criteria: Non-ETT general anesthesia with age• An a-priori power analysis revealed 785 records would power results (1- β=0.80, α=0.05, Df=1, W=0.1). • Univariate analysis was done on categorical and continuous data. • Bivariate analysis for POST and lidocaine was conducted and RR, CI, and chi-Square p-values were reported. • Binary logistic regression analysis was performed.
Discussion This retrospective observational EBP study shows that rates of POST among patients receiving GA with an ETT are 21% (n=318). Of the POST group, 81% did not receive any form of intratracheal lidocaine (n=282). The most common form of intratracheal lidocaine used was via laryngotracheal topical anesthesia (LTA). Limitations of this study include small sample size, limited and subjective reporting of POST, and inconsistent documentation of intratracheal lidocaine. Multiple studies support the use of intratracheal lidocaine to prevent the development of POST after general anesthesia with an ETT.1 This EBP project shows that there was a statistically insignificant reduction of POST with the use of 4% LTA. However, this study may generate hypothesis about LTA use, given limited research published on the use of LTA’s for POST. Lidocaine gel 2% showed statistically significant reduction in POST. Only one occurrence of intra-cuff lidocaine was documented, showing no reduction in POST, however there is strong research evidence showing the effectiveness of intra-cuff lidocaine on the reduction of POST. 4 This study may inform further hypothesis about group characteristics of patients receiving intratracheal lidocaine.
-

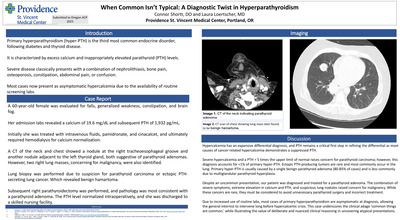
Intraoperative Hypotension and Acute Kidney Injury in Non-Cardiac Surgery at Providence Sacred Heart Medical Center
Elizabeth Davison, Amanda Affleck, and Kenn B Daratha
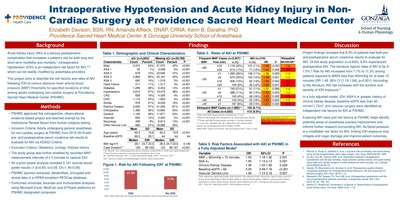
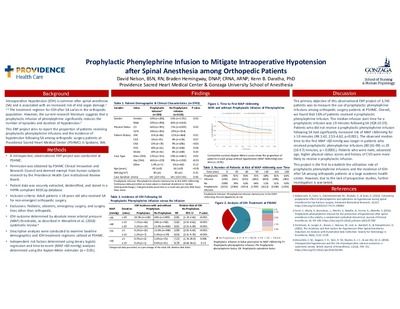
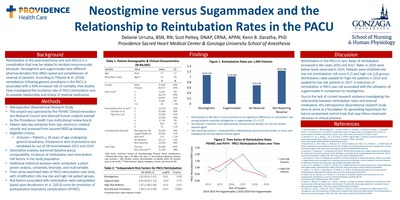
Background Acute kidney injury (AKI) is a serious postoperative complication that increases a patient’s risk for both long and short-term morbidity and mortality.1 Intraoperative hypotension (IOH) is an independent risk factor for AKI,2-5 which can be readily modified by anesthesia providers. This project aims to describe the risk factors and rates of AKI following IOH at various absolute mean arterial blood pressure (MAP) thresholds for specified durations of time among adults undergoing non-cardiac surgery at Providence Sacred Heart Medical Center (PSHMC).
Methods PSHMC approved this retrospective, observational evidence-based project and deemed the project exempt by the Institutional Review Board from human subjects testing. Project inclusion criteria consisted of adults undergoing general anesthesia for non-cardiac surgery at PSHMC from 2015-2019 with pre- and postoperative serum creatinine lab results to evaluate for AKI via the KDIGO Criteria. Obstetrics, urology, dialysis history and records with missing serum creatinine values were excluded. The study group was further stratified by recorded MAP measurement intervals of ≤ 5 minutes to capture IOH. An a-priori power analysis revealed 2,181 records would power results (1-β=0.80, α=0.05, Df=1, W=0.06). PSHMC sponsor extracted, deidentified, encrypted and stored data in a HIPAA compliant REDCap database. Project team members performed univariate, bivariate and multivariable analyses using Microsoft Excel, MedCalc and G*Power platforms on PSHMC designated computers.
Discussion Project findings revealed that 8.3% of patients had both pre- and postoperative serum creatinine results to evaluate for AKI. Of this study population (n=4,603), 8.9% experienced postoperative AKI. The literature reports rates of AKI to be 5- 7.5%. 5 Risk for AKI increased from 7.7% to 11.3% among patients exposed to MAPs less than 60mmHg for at least 10 minutes (RR 1.48, 95% CI [1.19-1.84], p<0.001). According to the literature, AKI risk increases with the duration and severity of IOH exposure. 5 In a fully adjusted model, IOH, ASA 4 or greater, history of chronic kidney disease, baseline eGFR less than 60 ml/min/1.73m2 , and vascular surgery were identified as independent risk factors for AKI at PSHMC. Exploring AKI rates and risk factors at PSHMC helps identify potential areas of anesthesia practice improvement and informs further research surrounding AKI. As blood pressure is a modifiable risk factor for AKI, limiting IOH exposure may mitigate end organ damage and improve patient outcomes.
-

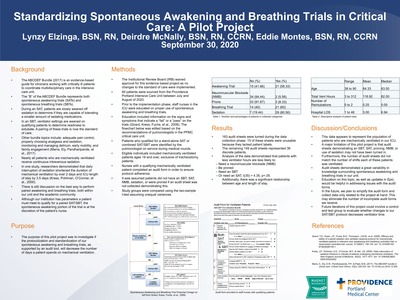
Standardizing Spontaneous Awakening and Breathing Trials in Critical Care: A Pilot Project
Lynzy Elzinga, Deirdre McNally, and Eddie Montes
-
 Reduction Technique by Amanda Grimes and Rebecca Choma")
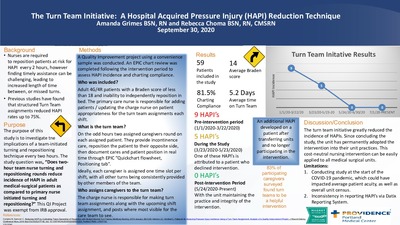
The Turn Team Initiative: A Hospital Acquired Pressure Injury (HAPI) Reduction Technique
Amanda Grimes and Rebecca Choma
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}