
-

Axial Spondyloarthritis
Philip Mease and Muhammad Asim Khan
From the Publisher:
Focusing on the key essentials you need to know, Axial Spondyloarthritis provides a quick, expert overview of axSpA from a clinical perspective. This concise resource by Drs. Philip Mease and Muhammad Khan presents practical recommendations and guidelines for the diagnosis, management, and treatment of spondyloarthritis impacting the axial skeleton alongside an overview of epidemiology, special populations, and patient education.
Key Features
- Discusses key information on genetic factors and disease biomarkers.
- Presents an overview of clinical features, classification criteria, and imaging to aid in diagnosis.
- Covers management and treatment guidelines, including non-pharmacologic management and the use of biologics.
- Consolidates essential information on this timely topic into a single, convenient resource.
-

Biologic Treatment of Axial Spondyloarthritis
Philip Mease and F. Van den Bosch
From the Publisher:
Focusing on the key essentials you need to know, Axial Spondyloarthritis provides a quick, expert overview of axSpA from a clinical perspective. This concise resource by Drs. Philip Mease and Muhammad Khan presents practical recommendations and guidelines for the diagnosis, management, and treatment of spondyloarthritis impacting the axial skeleton alongside an overview of epidemiology, special populations, and patient education.
Key Features- Discusses key information on genetic factors and disease biomarkers.
- Presents an overview of clinical features, classification criteria, and imaging to aid in diagnosis.
- Covers management and treatment guidelines, including non-pharmacologic management and the use of biologics.
- Consolidates essential information on this timely topic into a single, convenient resource.
-

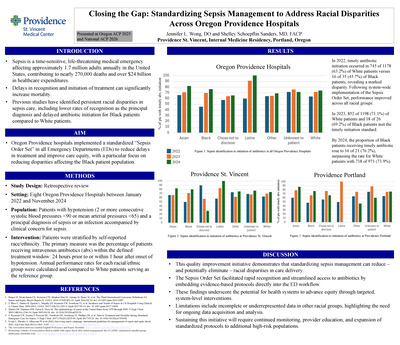
2018 In Review & What to Look Forward to in 2019
Pacific Neuroscience Institute
2018 flew by and was another amazing year of growth and transformation for Pacific Neuroscience Institute. Already in the first quarter of 2019 our multiple clinical and research projects are moving full steam ahead, and we look forward to further expanding our offerings, bringing world-class care to more patients. We are excited to be a cohesive, collaborative group of physicians and researchers with tremendous support from Saint John’s Health Center Foundation, Saint John’s Health Center and Providence Saint Joseph’s Health, allowing us to serve more people in need and to advance clinical care with active participation in the development of new diagnostics and therapeutics, both surgically and medically.
Here are HIGHLIGHTS of our accomplishments in 2018 and a look at what we have planned for 2019.
-

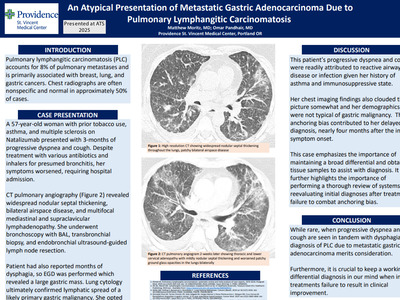
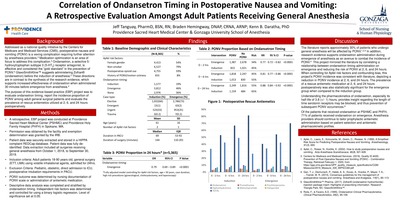
Comparison of Ondansetron, Dexamethasone, and its Combination in the Prevention of Postoperative Nausea and Vomiting
Alina Palanchuk and Kenn B Daratha
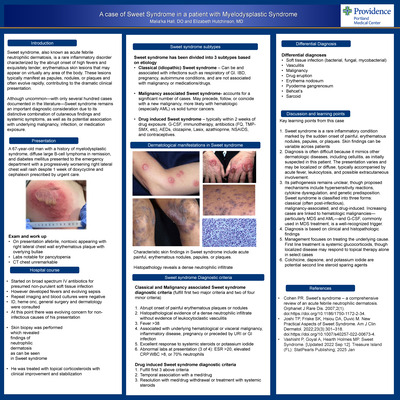
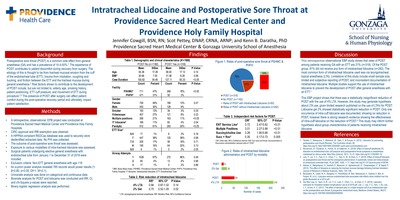
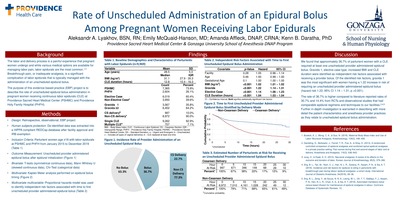
Background Postoperative nausea and vomiting remains a common and unpleasant side effect for patients following surgery. Uncontrolled PONV can result in prolonged hospital stays, unanticipated hospital readmissions, and decreased patient satisfaction. The Apfel score identifies and counts independent risk factors for PONV; females, non-smokers, postoperative opioid use, and history of PONV or motion sickness. Rates of PONV increases as the number of risk factors increase. The primary intervention to decrease PONV is administration of prophylactic antiemetics. Research supports the use of combination antiemetic therapy for patients with a high number of risk factors. The purpose of this evidence based practice (EBP) project was to report the rate of PONV among surgical patients who received general anesthesia, comparing combination prophylactic antiemetics of ondansetron and dexamethasone to single antiemetic administration.
Methods A retrospective, EBP project was conducted at Providence Sacred Heart Medical Center (PSHMC) in Spokane, WA. • Permission was obtained by the facility and exemption determination was granted by the IRB. • Patient data was securely extracted and stored in a HIPPA compliant REDCap database. Patient data was fully de-identified. Data extraction included all surgeries in the 2018 calendar year. • Inclusion criteria: Adult patients > 18 years old, non-emergent surgery, general anesthesia (ETT, LMA) using volatile inhalational agents or total intravenous anesthesia. • Exclusion criteria: Pediatric, obstetric, emergency surgery, direct admission to ICU. • PONV outcome determined by nursing documentation of PONV scale, intervention, reassessment or signs/symptoms or administration of antiemetic medication. • Descriptive data analysis completed and stratified by the number of Apfel risk factors. Independent risk factors determined using binary logistic regression. Level of significance set at 0.05.
Discussion CONCLUSION When controlling for all literature reported PONV risk factors, this EBP project demonstrated that the odds of PONV reduction were similar for combination and individual antiemetic therapy. Similar to current research evidence, the identified independent risk factors for PONV were female gender, history of PONV or motion sickness, postoperative opioid administration, younger age, high risk procedures, and increased case duration. Non-smoking status and nitrous oxide use were not observed to be independent risk factors. As Apfel reported, this project similarly reported an increase rate in PONV as the number of PONV risk factors increased. The observed risk of PONV decreased among patients with at least one Apfel risk factor following prophylactic antiemetic administration. IMPLICATIONS Practice at PSHMC is demonstrating that combination prophylactic treatment is being used for patients with higher PONV risk factors. Practice is following current research evidence. Anesthetists should continue to tailor prophylactic antiemetic administration to patients based on presenting risk factors.
-
Evaluating the Efficacy and Safety of Transitioning Patients from Natalizumab to Ocrelizumab (OCTAVE)
Kyle E Smoot, Kiren Kresa-Reahl, Pavle Repovic, Jessica Craddock, Chiayi Chen, Lindsay Lucas, Tiffany Gervasi-Follmar, and Stanley Cohan
-

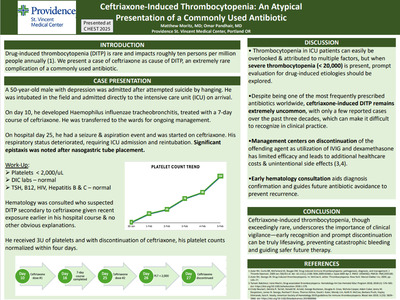
COMPARISONS OF PREOPERATIVE BLOOD PRESSURES IN SURGICAL PATIENTS
Brian Stacy and Kenn B Daratha
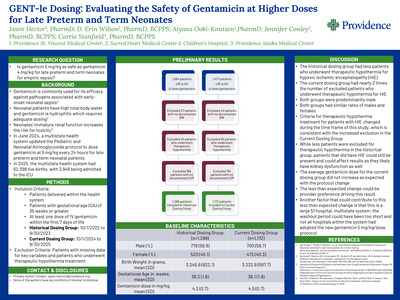
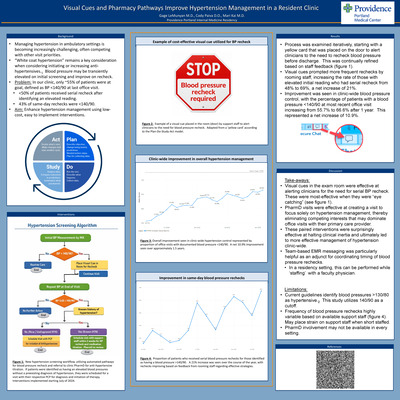
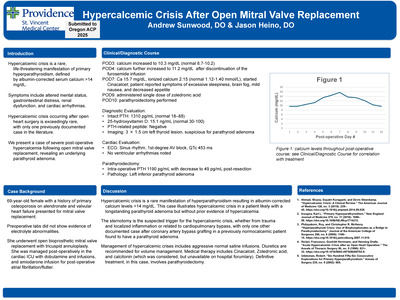
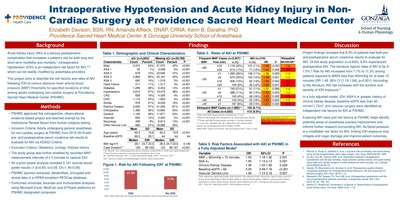
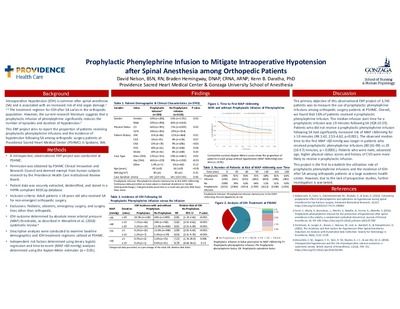
Background Surgical patients expect anesthesia providers to provide high quality care. Blood pressure variability must be mitigated by establishing the patient’s blood pressure baseline and sustaining it through surgery. A consensus has not been established on which blood pressure measurement should be used as the patient’s baseline. Blood pressures before surgery in multiple care settings have been shown to vary. This may result in differences in drug and fluid administration, depending on the blood pressure considered baseline by the anesthesia provider. The purpose of this observational evidence-based practice project was to compare mean blood pressures leading up to surgery among patients at Providence Sacred Heart Medical Center (PSHMC).
Methods Literature review identified five high quality studies to inform this project. • Institutional approval sought and obtained. IRB determined exempt research. • Data on adult, elective surgical patients receiving a general anesthetic from 09/30/2017-10/1/2018 were extracted in an anonymized fashion. • Patients characterized by demographic and clinical characteristics (table 1). • Mean blood pressures calculated from three settings: ambulatory clinics in the 12 months prior to surgery, the surgical admit unit (SAU) and the “first on table” (FOT) or first pressure recorded in the operating room. Patients without blood pressures recorded in each care setting excluded. • Repeated measures ANOVA and multiple linear regression (α=0.05).
Discussion SBP increased significantly from the pre-surgical ambulatory period to the first on table (FOT) blood pressure taken in the operating room. Changes in MAP were statistically, but not clinically, significant. A multivariable regression model revealed age, sex, heart failure, atrial fibrillation, hypertension, chronic kidney disease and peripheral vascular disease to be factors predictive of increasing FOT SBP. Our findings are consistent with current research evidence. Providence Sacred Heart Medical Center patients may experience over-treatment for hypotension if the first-ontable SBP is utilized as a baseline. This overtreatment may result in increased monetary and physical costs.
-

2018 System Library Services Visual Annual Report
Amanda Steinvall
A visual report of the 2018 activities and accomplishments by System Library Services at Providence St. Joseph Health
-

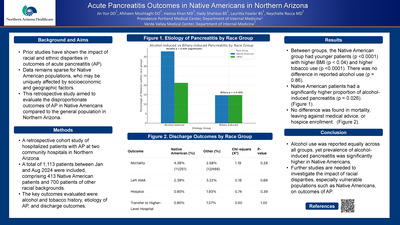
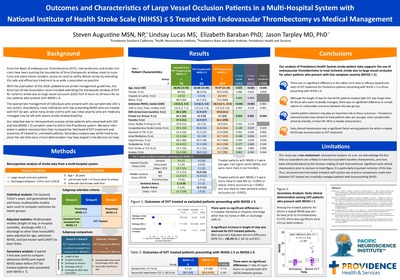
Impact of Early Mobilization on 90-Day Outcomes in Thrombectomy Patients
Tamela Stuchiner, Diane Clark, Lindsay Lucas, John Robinson, and Lisa Yanase
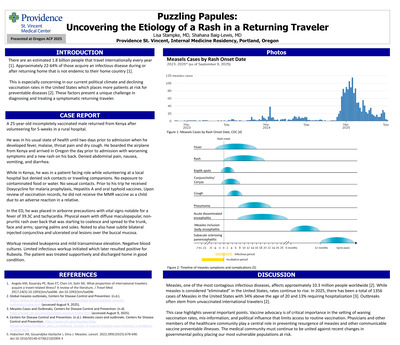
Introduction: Early mobilization of ischemic stroke patients receiving IV alteplase (tPA) did not worsen 90-day outcome at two urban stroke centers in a prior study, but there are no studies evaluating outcomes of early mobilization after thrombectomy. The mobility protocol used in the previous study was also utilized to mobilize stroke patients receiving thrombectomy treatment at these two centers, once minimum number of hours for groin precautions was complete and the groin puncture site was stable. The objective of this study was to determine for post-thrombectomy patients mobilized within 24 hours, whether earlier mobilization worsened outcomes.
Methods: Medical records of ischemic stroke patients receiving thrombectomy at two urban stroke centers between May 2013 and December 2017 were reviewed for early mobilization (within 24 hours of groin puncture). Patients who did not expire in hospital and had complete data were included in the analysis. Ordinal regression was used to determine if, with each hour delay in time first up, patients’ functional outcomes worsened at 90 days using the modified Rankin scale (mRS), adjusting for pre-symptom onset mRS, admission NIHSS, age, sex, and post-treatment thrombolysis in cerebral infarction (TICI) grade. The mRS at 90 days was categorized as no symptoms or no significant disability (0 - 1), mild or moderate disability (2 - 3), and severe disability or death (4 - 6).
Results: Of 147 patients mobilized within 24 hours, 91 patients were included in the analysis. Overall, 51% (n=46) were female, 74% (n=67) had no disability prior to their stroke, mean age was 68.0 (±14.1), mean admission NIHSS was 15.9 (±6.7), and 85% (n=78) had a post treatment TICI score of 2b or greater. Median time first mobilized was 14.1 hours [interquartile range: 9.4, 19.1]. Ordinal regression showed no evidence that earlier mobilization had an effect on patient outcomes at 90 days, patients were neither worse or better by time first mobilized within the first 24 hours (p=.706).
Conclusions: Ischemic stroke patients receiving thrombectomy were mobilized within 24 hours of groin puncture by the early mobility protocol. Patients experienced no impact on outcomes at 90 days by time first mobilized. This result may have been limited by small sample size.
-

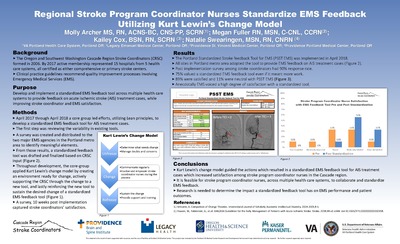
Cost Analysis of Implementing Standardized Stroke Patient Education Materials in a Large Five State Health System
Natalie Swearingen, Leslie Corless, Jessica Swann, Kailey Cox, Diane Lada, and Elizabeth Baraban
-

Large Five State Health System Standardizes Stroke Patient Education While Significantly Improving Health Literacy
Natalie Swearingen, Leslie Corless, Jessica Swann, Kailey Cox, Diane Lada, and Elizabeth Baraban
-

Evaluating Bundle Adherence in Ventilated Patients: A Quality Improvement Project
Melanie Webb and Lindsay Iverson
-

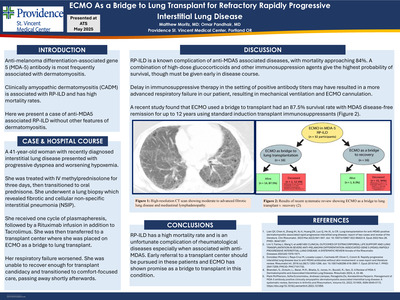
General Anesthetic Induction Sequence High Fidelity Simulation: Determining Efficacy Among Novice Student Registered Nurse Anesthetists
Alex Wilkie, Steven Urbick, and Kenn B Daratha
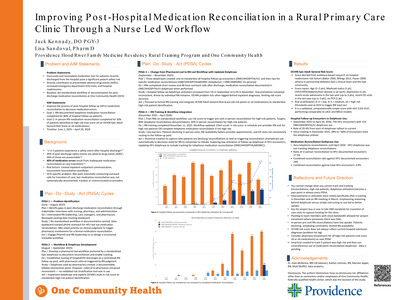
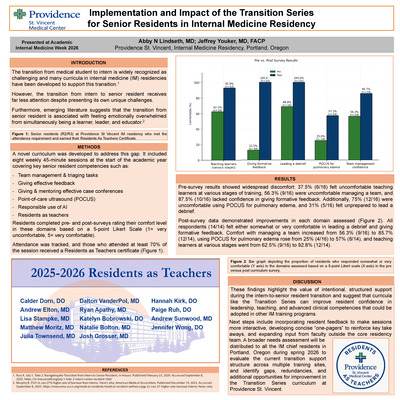
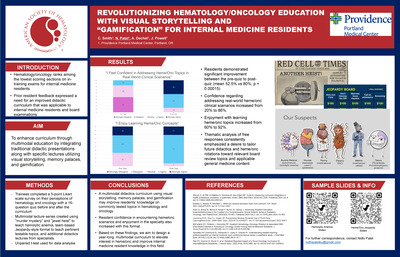
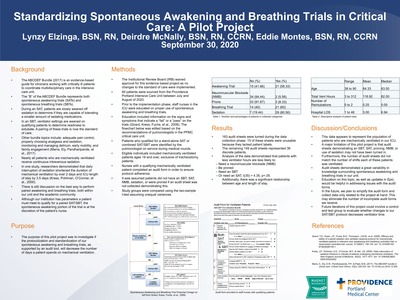
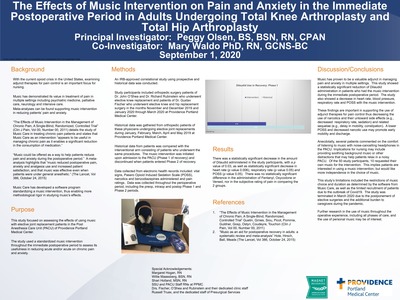
Background High Fidelity Simulation (HFS) is used across multiple health professions. Despite the wide variety of clinical experiences that Student Registered Nurse Anesthetists (SRNA) possess prior to training, the induction sequence to a General Anesthetic (GA) is a daunting task. Although the efficacy of HFS has been widely studied within undergraduate nursing programs, there are no studies published determining the efficacy of HFS on SRNA training. The purpose of this study was to determine the efficacy of simulation training amongst entry-level SRNA’s and examine any individual participant factors that may influence clinical performance within HFS.
Methods • Human subjects were protected (Spokane IRB ID: STUDY18000465) • Pilot study participants recruited from 1st semester SRNAs in the Doctorate of Nurse Anesthesia Practice (DNAP) • Full study participants recruited from prospective DNAP students • Primary endpoints: efficacy of GA induction sequence HFS • Secondary endpoints: individual participant factors that may influence clinical performance within HFS • Scoring tool developed to measure primary outcome (Figure 2) • PowerPoint and didactic lecture provided to all participants • Pretest assessment following didactic training, using scoring tool, prior to HFS • Participants guided through HFS and subsequently debriefed • Posttest assessment completed following HFS using scoring tool • Each participant allotted 60 minutes for individual HFS session • Analysis of variance utilizing a waitlisted study design • A priori confidence level (α < 0.05)
Discussion Our sufficiently powered study detected a 29.0% (mean pre-test 23.7, mean post-test 33.4) improvement in Simulation Assessment Tool scores following HFS (p < 0.001). Despite variations in pre HFS scores, post HFS scores remain homogeneous across all participants confirming the effectiveness of our training. Our study also indicated that there were no statistically significant group differences in HFS pre-test scores amongst the participants for the demographic factors we assessed; type of ICU (p=0.76), years of ICU experience (p=0.36), and age (p=0.91). GA induction sequence training using HFS was proven to be effective among novice SRNA’s. In alignment with the current research evidence, the use of HFS among SRNA’s may help to improve learning, self-efficacy, and subsequently patient safety. Doctoral nurse anesthesia programs should consider the integration of HFS throughout program curriculum.
-

Transfusion Ratios Following Activation of a Massive Transfusion Protocol: An Evidence Based Practice Project
Cody Woodbury and Kenn B Daratha
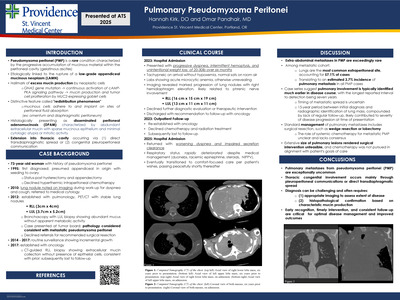
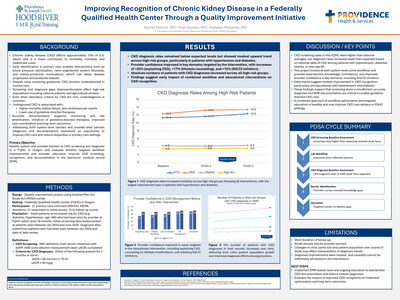
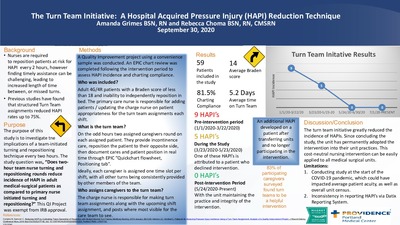
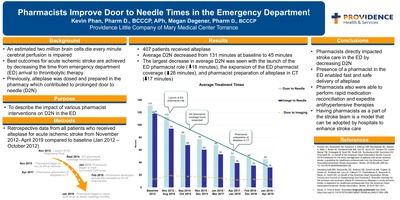
Background Accidental injury is one of the leading causes of death in the United States and worldwide. Severe hemorrhage from injury is the leading cause of preventable death. Effective management of hemorrhaging trauma patients has been evolving since the early 1900’s. Recent studies have demonstrated the benefits of using a balanced resuscitation technique, revolving around the goal of recreating whole blood. The purpose of this project was to identify what ratios of blood products are being transfused at Providence Sacred Heart Medical Center (PSHMC) and Providence Holy Family Hospital (PHFH).
Methods A literature review was performed identifying seven high quality peer-reviewed studies. • Institutional approval and IRB review for exemption determination completed. Human subjects were protected. • Registry data extraction in an anonymized fashion. • Patients who received no packed red blood cells or had no age specified were excluded. • Patients organized by demographic and clinical characteristics. • 24-hour mortality rates extracted from the electronic health record. • Post hoc power analysis was completed. • High ratio transfusion was defined as a ratio approaching or greater than 1:1 with packed red blood cells always being the denominator (i.e. FFP:PRBC, PLT:PRBC).
Discussion Massive transfusion ratios among hemorrhaging patients at PSHMC and PHFH were observed at high ratio 35% of the time, when comparing fresh frozen plasma to packed red blood cells, and 49% of the time, when comparing platelets to packed red blood cells. Trauma patients account for 39% of all massive transfusions at PSHMC and PHFH. Though some cases of massive transfusions observed in this project did achieve high transfusion ratios, it is unclear what reasons prevented high transfusion ratios. Research evidence suggest that mortality risk is higher when lower ratios are utilized during massive transfusions. However, this project was not powered to detect mortality differences by ratios.
-

Complications from IV Alteplase in Mild Stroke Patients in a Multi-state Health System
Lisa R. Yanase, Lindsay Lucas, Leslie Corless, and Elizabeth Baraban
-

Implementation of Coordinated Telestroke Program in an Urban Setting Improves Acute Stroke Care
John Zurasky, Leslie Corless, Lindsay Lucas, and Elizabeth Baraban
Purpose: Telestroke has been shown to improve acute ischemic stroke (AIS) care in rural settings, but few studies have examined the impact of telestroke in an urban setting. In an urban area, there was a planned transition from an outpatient-based acute stroke provider pool to a centralized telehealth team of neurovascular and neurocritical care providers. This study assessed the impact of this change by comparing patient outcomes during three time periods: pre-initiation (PRE), transition after initiation (TRAN) and post-transition (POST).
Methods: Data for AIS patients 18 and older from five urban hospitals were used. Outcomes were hospital length of stay (LOS) and percentage of patients who had a door-to-needle time (DTN) <45 and><60 >minutes, IV-alteplase or endovascular treatment, an IV-alteplase-related complication, and a discharge other than to home or rehab. Generalized linear and Cox proportional hazard models were used to compare outcomes for patients discharged during PRE (June 2015 - June 2016), TRAN (July 2016 – December 2016) and POST (January 2017 – March 2018) time periods adjusting for arrival mode, gender, admit NIHSS, age, and arrival time.
Results: Of 4,984 patients that met inclusion criteria, there were 2,075 treated in PRE, 1,052 in TRAN and 1,857 in POST. After adjustment, TRAN patients were 1.77 times more likely to be treated with IV-alteplase than PRE patients (p=.013). POST patients were 2.46 times more likely to receive endovascular treatment than PRE patients (p=.009) and 2.07 times as likely as those in the TRAN period (p=.007). Patients in the TRAN period were 1.63 times more likely to be treated with IV alteplase in <60 minutes>(p<.001) and 2.22 times more likely in the POST period (p=.002) compared to those in PRE. There were no significant differences in the odds of being treated in <45 minutes, LOS, or discharge disposition.
Conclusion: A transition to a specialty stroke care through a telestroke network showed improvements in treatment rates and percentage of patients with DTN less than 60 minutes.
-

Intratumoral Delivery of MDNA55, an Interleukin-4 Receptor Targeted Immunotherapy, by MRI-Guided Convective Delivery for the Treatment of Recurrent Glioblastoma
Achal Achrol, Manish Aghi, Krystof Bankiewicz, Martin Bexon, Sotirios Bisdas, Steven Brem, Andrew Brenner, Nicholas Butowski, Melissa Coello, Seunggu Jude Han, Santosh Kesari, Fahar Merchant, Dina Randazzo, Diana Roettger, Michael Vogelbaum, Frank Vrionis, Miroslaw Zabek, and John Sampson
-
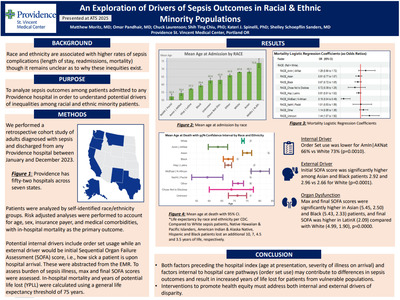
Changes in Hospital Performance and Transition-Care Measures 1-Year After Initiation of the Patient Navigator Program
Nancy M. Albert, Tyler J Gluckman, Robert McNamara, Gregg C. Fonarow, Adnan Malik, Ralph Brindis, Di Lu, Matthew Roe, Judy Tingley, Smita Negi, Lee R. Goldberg, Susan Rogers, Julie Mobayed, Shilpa Patel, Beth Pruski, Kathleen Hewitt, Zaher Fanari, and Joseph Lucas
Background
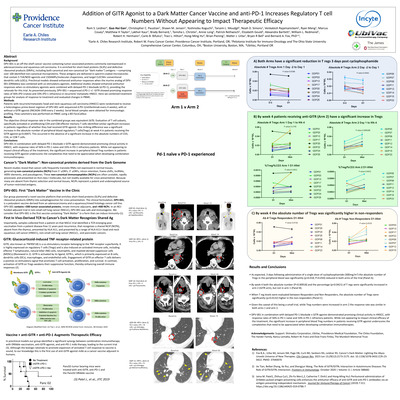
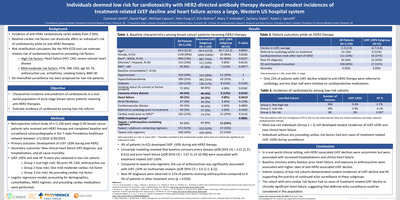
Despite high rates of early readmission in patients with acute myocardial infarction (AMI) and heart failure (HF), little data exists regarding the impact of best practices on hospital-based transition-care measures. This project sought to evaluate early changes in AMI and HF program performance after implementing the American College of Cardiology Patient Navigator Program—a transition-care improvement initiative at 35 acute care hospitals.
Methods
Baseline and 1-year post intervention data from 3860 patients with AMI or HF were analyzed using Wilcoxon signed rank test for 17 care measures related to hospital processes (8), medication reconciliation (3), education delivery/documentation (2), HF patient identification prior to discharge (1), scheduling a follow-up appointment within seven days (1), and associated 30-day unadjusted rates of AMI and HF readmission (2).
Results
Among Patient Navigator hospitals, 68.6% were urban and 77.1% were teaching. Baseline and 1-year assessments demonstrated wide variability in aherence for many measures. Compared with baseline, median (25th, 75th percentiles) performance improved for use of an evidence-based beta-blocker among patients with HF, from 91.6% (86.2%, 95.0%) to 93.8% (88.2%, 98.6%), p= 0.028; medication reconciliation at admission, discharge and both admission and discharge (all p≤ 0.05); scheduling of HF follow-up appointments (p= 0.004) and self-care education (p= 0.005). Post-AMI in-hospital mortality improved from 4.0% (4.0%, 5.0%) to 3.7% (3.3%, 4.3%), p= 0.015 and 30-day unadjusted HF readmission was non-significantly lower by 1.9%; from 19.0% (15.2%, 21.0%) to 17.1% (14.1%, 19.1%), (p= 0.09).
Conclusion
Transition-care interventions were associated with significant improvement in 6 processes of care and 1 outcome performance measure for patients with AMI or HF.
-

Diabetic Kidney Disease
Radica Alicic, Emily J Johnson, and Katherine Tuttle
From the Publisher: From basic science to practical clinical tools, Chronic Kidney Disease, Dialysis, and Transplantation, 4th Edition provides you with the up-to-date, authoritative guidance you need to safely and effectively manage patients with chronic renal disease. Covering all relevant clinical management issues, this companion volume to Brenner and Rector’s The Kidney presents the knowledge and expertise of renowned researchers and clinicians in the fields of hemodialysis, peritoneal dialysis, critical care nephrology, and transplantation – for an all-in-one, indispensable guide to every aspect of this fast-changing field.
-
Anticoagulation optimization: Capturing triple aim value in percutaneous coronary intervention within a large health system
Braden Batkoff, P Casterella, Tyler J Gluckman, and A Lee
-
 by Braden Batkoff, Tyler J Gluckman, Robert Hunter, Michael Ring, Leland Siwek, Branden Reynolds, Matthew Forrester, and Steven Thew")
Improving the Value of Transcather Aortic Valve Replacement (TAVR)
Braden Batkoff, Tyler J Gluckman, Robert Hunter, Michael Ring, Leland Siwek, Branden Reynolds, Matthew Forrester, and Steven Thew
-

Inverted L Osteotomy for Management of Severe Mandibular Deficiency with Short Posterior Face Height
R. Bryan Bell and Andrew Weeks
From the Publisher:
This trusted, three-volume resource covers the full scope of the field with up-to-date, evidence-based coverage of surgical procedures performed today - including cleft and craniofacial surgeries, oral surgery, oncologic surgery, orthognathic surgery, trauma surgery, surgical pathology, surgery of TMJ disorders, dental implants, dentoalveolar surgery, cosmetic surgery, and reconstructive surgery. More than 4,800 full-color images and illustrations serve as valuable visual references. You'll also find complete guidelines for a wide range of practice issues such as anesthesia, diagnostic imaging, treatment planning, , psychological considerations, office design and ergonomics, plus new information on implants and orthognathic surgery. It's all the information you need to perfect your oral and maxillofacial surgical techniques and provide state-of-the-art care for your patients.
-

CLABSI Rangers: A Team Approach to Extinguishing CLABSI
Alisa Bowman, Christine Bartlett, Sarah Gattis, Staci Hartmann, Eddie LeSage, Heidi Mosher, Joya Picket, and Sarah Potts
Purpose: Decrease incidence of Central line Associated Bloodstream Infection (CLABSI) in the ICU/IMCU at Swedish Medical Center by August 31st 2018, with the overall goal of zero CLABSI stemming from the ICU’s.
Synthesis of Evidence: A review of CLABSI costs, the problem as a whole, and products that help decrease CLABSI was completed. Swedish’s current CLABSI state was discussed and ways to improve existing practices investigated. Ideas to engage and educate patients, family and staff in order to bolster infection prevention practices was reviewed.
Change in practice: Based on the evidence and our protocols we began reviewing patient charts for the existence of central line flush orders and discovered they were not being ordered as they should be. We developed a way to catch missing orders by discussing saline flushes during Medical Directed Rounds (MDR’s) and later adopted the intervention. We developed a central line order-set to streamline central line orders. We trialed products making dialysis lines a closed system and educated staff regarding its use. We switched the practice of accessing dialysis catheters using betadine to utilizing alcohol due to its similar efficacy and faster dry time. Many of these changes not only effected ICU practice but the entire First Hill campus.
Implementation: Staff were educated extensively on new products brought in to create a closed dialysis system, products available for patient/family education and documentation in EPIC. We also filmed a series of four short educational videos designed to engage and educate staff. Saline flushes were added to daily rounds sheets to insure they were flushed per protocol and lastly, we required that 1:1 return demonstrations occur for nurses who access dialysis lines.
Evaluation: At nine months post implementation, the Surgical Intensive Care Unit (SICU) had incurred two CLABSI, the Medical ICU (MICU) and Intermediate Care Unit (IMCU) have remained CLABSI free. This is equivalent to an 80% reduction in CLABSI when compared to the same time period the year prior. 93% of RN’s who access dialysis lines were educated and audits of charts show an increase in patient central line education from 41-71%. Target Standardized Infection Ratio (SIR) of < 1 has been met or exceeded and the number of champions recruited has been exceeded as well. Target Standardized Utilization Ratio (SUR) has not been impacted as we had hoped.
Conclusion: Implementing a group of 4 bedside RN’s interested in improving CLABSI rates in the ICU has been effective in decreasing the incidence of CLABSI on the units. Change was affected by educating staff via short videos, posting scrub the hub signage and central line education in patient rooms, implementing saline flush orders during MDRs, the addition of new products keeping the dialysis catheter a closed system and requiring return demonstrations of proper dialysis access. Use of incentives helped to bring about compliance and rewards staff for their excellent work.
Presenting Author: Alisa Bowman RN, CCRN, Nurse Quality Leader for Infection Prevention, Swedish Medical Center, FH ICU
References
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}