
-

Pulmonary Pseudomyxoma Peritonei
Hannah Kirk, DO and Omar Pandhair
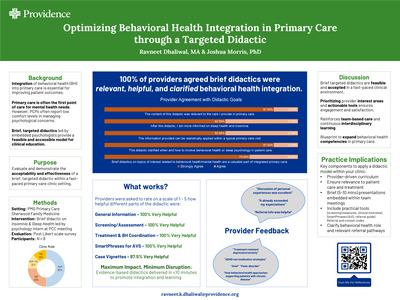
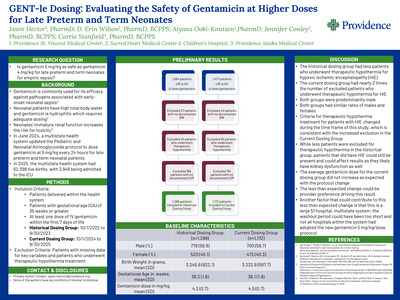
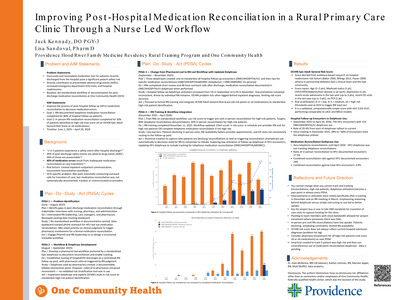
Introduction: Pseudomyxoma peritonei (PMP) is an intra -abdominal cancer occurring in one to four out of one million patients. It begins as a mucinous adenocarcinoma of the appendix that implants on other peritoneal surfaces, spreading into gelatinous ascites. Treatment consists of hyperthermic intraperitoneal chemotherapy (HIPEC) and cytoreductive surgery (CRS). Extra -abdominal metastases are rare. We present the case of a patient who underwent treatment for PMP and was found to have lung nodules over a decade later. Case Presentation: A 73 -year -old woman with pseudomyxoma peritonei presented to the emergency department with progressive dyspnea and unintentional weight loss. Twenty -eight years earlier she was found to have appendiceal pseudomyxoma peritonei with extension to her right ovary and underwent CRS, though she didn't receive HIPEC. Fifteen years later, she was noted to have lung nodules and underwent bronchoscopy with biopsy that revealed mucinous cystic lesions. Body -wide imaging was negative for recurrence or other metastases. She was monitored with serial imaging that showed stable sized nodules approximately 5 x 3.5 cm in the right lower lobe and 5 x 4 cm in the left upper lobe. She presented seven years later with twenty -pound weight loss, progressive dyspnea on exertion, and intermittent hemoptysis. She was borderline tachycardic without hypoxemia and newly anemic with a three -point hemoglobin drop to 8.9 g/dL. Computed tomography of the chest showed a right - sided mass 15.3 x 14.9 x 19 cm in size and a left -upper mass 12.9 x 11.3 x 11 cm in size with compression of adjacent bronchi and vasculature. Discussion: Extra -abdominal metastases of PMP are exceedingly rare. Within the metastatic cohort, the lungs accounted for 57.1% of cases, suggesting 3.7% of PMP cases developed pulmonary metastases. While it is unclear when our patient first developed pulmonary metastases, a case series suggests these are usually identified much earlier, with the longest time to discovery of lung metastasis being seven years. This is likely why our patient's masses grew to such a significant size, as none of the metastases identified in case series was even half the size of hers. Unfortunately, treatment of pulmonary metastases is usually accomplished with wedge resection or lobectomy, and our patient's masses had grown so large that this was unfeasible. While it is unclear whether systemic chemotherapy has a role in the treatment of metastatic PMP, the patient discussed a trial with oncology and elected to forego any further workup or treatment.
-

Addition of GITR Agonist to a Dark Matter Cancer Vaccine and anti-PD-1 Increases Regulatory T cell Numbers Without Appearing to Impact Therapeutic Efficacy
Rom S. Leidner1, Guo Hui Gan1, Christopher C. Paustian, and Shawn M. Jensen
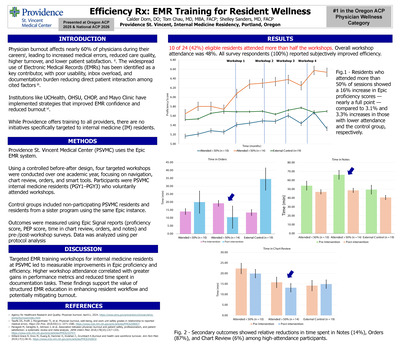
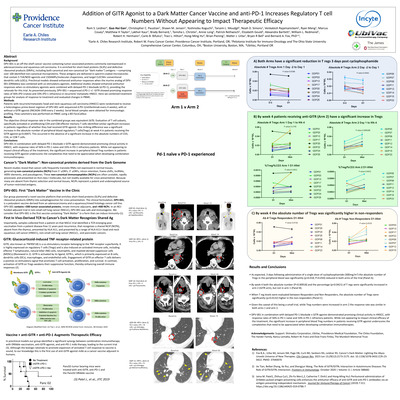
Background: DPV-001 is an off-the-shelf cancer vaccine containing tumor associated proteins commonly overexpressed in adenocarcinoma and squamous cell carcinoma. It is enriched for short-lived proteins (SLiPs) and defective ribosomal products (DRiPs), including both canonical and non-canonical (or “dark matter”) antigens —comprising over 100 identified non-canonical microproteins. These antigens are delivered in spectrin-coated microvesicles that contain 5 TLR/ NOD agonists and 15DAMPs/molecular chaperones, and target CLEC9A+ conventional dendritic cells (cDCs). Preclinical models showed enhanced antitumor responses when the murine analog of DPV-001 (DRibbles) was combined with co -stimulatory agonists. Additional studies showed enhanced antitumor responses when co-stimulatory agonists were combined with delayed PD-1 blockade (d.PD1), providing the rationale for this trial. As presented previously, DPV-001 + sequenced d.PD-1 +/- GITR showed promising response rates of 56% (PD-1naïve) and 33% (PD-1 refractory) in recurrent/ metastatic HNSCC. Here we combined treatment groups for analysis of response to treatment and evaluated changes in PBMC. Methods: Patients with recurrent/metastatic head and neck squamous cell carcinoma (HNSCC) were randomized to receive a heterologous prime-boost regimen of DPV-001 with sequenced d.PD-1(retifanlimab every 4 weeks), with or without a GITR agonist (INCAGN-1949 every 2 weeks). Serial blood samples were obtained for immunologic profiling. Flow cytometry was performed on PBMC using a BD FacsCalibur. Results: The objective clinical response rate in the combined groups was equivalent (4/9). Evaluation of T cell subsets, specifically activated or proliferating CD4 and CD8 effector memory T cells identified similar significant increases in patients regardless of whether they had received GITR agonist. One striking difference was a significant increase in the absolute number of peripheral blood regulatory T cells(Tregs) at week 4 in patients receiving the GITR agonist (p=0.0007). This occurred in the absence of a significant increase in the absolute numbers of CD3, CD4, or CD8 T cells. Conclusions: DPV-001 in combination with delayed PD-1 blockade ± GITR agonist demonstrated promising clinical activity in HNSCC, with response rates of 56% in PD-1 naïve and 33% in PD-1 refractory patients. While not appearing to impact clinical efficacy of the treatment, the significant increase in peripheral blood Treg numbers in patients receiving GITR agonist underscores the complexities that need to be appreciated when developing combination immunotherapies.
-

Visual Cues and Pharmacy Pathways Improve Hypertension Management in a Resident Clinic
Gage LeMunyan M.D.; Cody Paiva, DO; and Mari Kai, MD
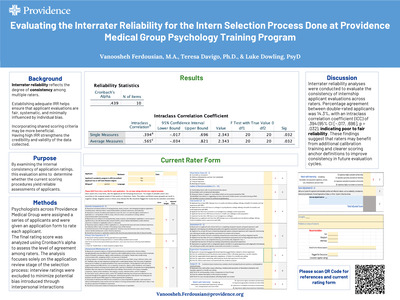
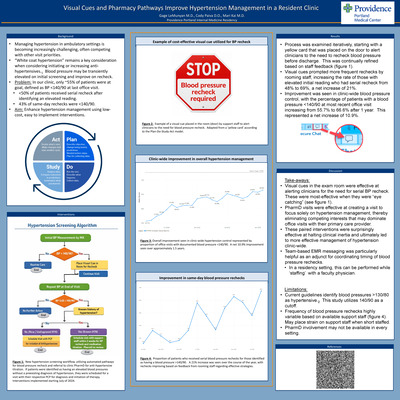
Background: Managing hypertension in ambulatory settings is becoming increasingly challenging, often competing with other visit priorities. “White coat hypertension” remains a key consideration when considering initiating or increasing anti-hypertensives. Blood pressure may be transiently elevated on initial screening and improve on recheck. Problem: In our clinic, only ~55% of patients were at goal, defined as BP < 140/90 at last office visit. • < 50% of patients received serial recheck after identifying an elevated reading. • 43% of same-day rechecks were < 140/90. Aim: Enhance hypertension management using low-cost, easy to implement interventions. Results: Process was examined iteratively, starting with a yellow card that was placed on the door to alert clinicians to the need to recheck blood pressure before discharge. This was continually refined based on staff feedback. Visual cues prompted more frequent rechecks by rooming staff, increasing the rate of those with elevated initial reading who had serial recheck from 48% to 69%, a net increase of 21%. Improvement was seen in clinic-wide blood pressure control, with the percentage of patients with a blood pressure < 140/90 at most recent office visit increasing from 55.7% to 66.6% after 1 year. This represented a net increase of 10.9%. Discussion: Visual cues in the exam room were effective at alerting clinicians for the need for serial BP recheck. These were most-effective when they were “eye catching”. PharmD visits were effective at creating a visit to focus solely on hypertension management, thereby eliminating competing interests that may dominate office visits with their primary care provider. These paired interventions were surprisingly effective at halting clinical inertia and ultimately led to more effective management of hypertension clinic-wide. Team-based EMR messaging was particularly helpful as an adjunct for coordinating timing of blood pressure rechecks. In a residency setting, this can be performed while ‘staffing’ with a faculty physician. Limitations: Current guidelines identify blood pressures >130/80 as hypertensive. This study utilizes 140/90 as a cutoff. Frequency of blood pressure rechecks highly variable based on available support staff. May place strain on support staff when short staffed. PharmD involvement may not be available in every setting
-

Implementation and Impact of the Transition Series for Senior Residents in Internal Medicine Residency
Abby Lindseth, MD and Jeffrey Youker
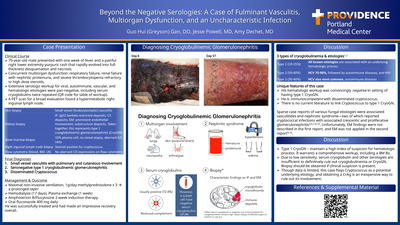
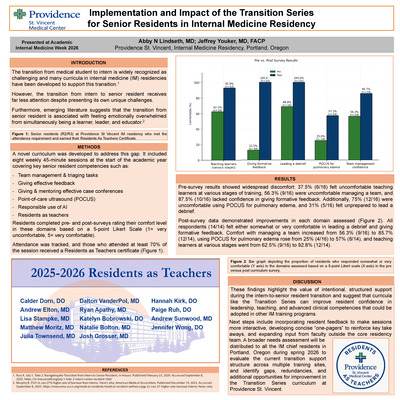
The transition from medical student to intern is widely recognized as a challenging period, and numerous curricula have been developed to support this transition. However, the transition from intern to senior resident receives far less attention despite presenting its own unique challenges. Anecdotal feedback from internal medicine residents and emerging literature suggests that the transition to senior resident is associated with feeling emotionally overwhelmed from simultaneously being a learner, leader and educator.1,2 To address this gap, the Transition Series was developed as a novel curriculum to support internal medicine residents as they advance into their senior roles. Building on the existing Intern Only series, the Transition Series emphasized leadership development, strategies for teaching, and advanced clinical skills not typically covered during intern year. By providing dedicated time for developing these skills, the curriculum aimed to enhance senior resident preparedness, confidence, and well-being in their new roles. The curriculum consisted of eight weekly 45-minute sessions at the start of the academic year, covering key senior resident competencies: team management, giving effective feedback, tools for giving and mentoring morning reports, point-of-care ultrasound (POCUS), residents as teachers, leading a debrief, and the responsible use of AI in medicine and medical education. Residents completed pre- and post-surveys rating their comfort in these domains (1 = very uncomfortable, 5 = very comfortable). Attendance was tracked, and those who attended at least 70% of the sessions received a Residents as Teacher certificate. Pre-survey results showed widespread discomfort: 37% (6/16) felt uncomfortable teaching learners at various stages, 56% (9/16) were uncomfortable managing a team, and 87.5% (10/16) lacked confidence in giving formative feedback. Additionally, 75% (12/16) were uncomfortable using POCUS for pulmonary edema, and 31% (5/16) felt unprepared to lead a debrief. Post-survey data demonstrated improvements in each domain assessed. All respondents (14/14) felt either somewhat or very comfortable in leading a debrief and giving formative feedback. Comfort with managing a team increased from 56.3% (9/16) to 85.7% (12/14), using POCUS for pulmonary edema rose from 25% (4/16) to 55.6% (5/9), and confidence in team management went from 43.8% (7/16) to 77.8% (7/9). These findings highlight the value of intentional, structured support during the intern-to senior resident transition and suggest that curricula like the Transition Series can significantly improve resident confidence in leadership, teaching, and advanced clinical competencies. Beyond the quantitative improvements, the series fostered a sense of community and validation among residents navigating their new responsibilities. A personal lesson learned through this project is the power of using lived experience to drive meaningful change and the importance of creating space for emerging educators to shape the systems they are a part of. Having just completed residency, I was uniquely positioned to prioritize topics that felt most relevant in real time. This perspective allowed me to design a curriculum that directly addressed the gaps I had experienced, and to advocate for a more learner-centered approach to resident development. Moving forward, resident feedback will be incorporated into the sessions to make them more interactive and include concise “one-pagers” to reinforce take-home points and support diverse learning styles. I also hope to broaden the scope of input by inviting perspectives from outside the residency core faculty, including subspecialists and recent graduates who have just experienced the transition. To further refine this curriculum and enhance the project’s reach, a focused needs assessment will be distributed to multiple internal medicine residency programs to better understand the challenges of this transition and refine the curriculum to meet evolving learner needs.
-

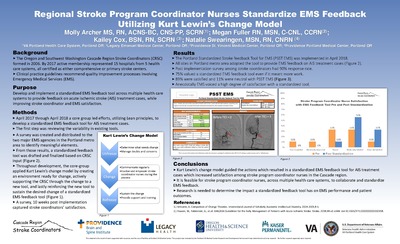
Emergency department prepack implementation at Providence Portland Medical Center
Bowei Liu PharmD; Jessica Dizon Scheer; and Mac Ovenell, PharmD, MS
Introduction: Providence Portland Medical Center (PPMC) implemented a multiphase ‑quality improvement‑ project to standardize the emergency department (ED) prepack program with the Providence Oregon region. Background/Purpose: Prior to the project, ED prepack dispensing lacked a uniform process; individual sites stored and labeled medications differently, reconciliation was paper based, and staff were unclear on regulatory limits. Oregon Board of Pharmacy rules allow prepack medications for outpatient use only when the supply does not exceed a ‑48-hour‑ course, with limited exceptions. Each prepack must also carry a unique serial number, and a label specifying the hospital’s pharmacy’s contact information, drug name and strength, manufacturer, expiration date, and other required elements. To bring PPMC into alignment with the regional standard operating procedure, the team established a structured program that encompassed formulary alignment, translation/accessibility improvements, and a reconciliation process. Methods: In Phase 1, pharmacy informatics specialists (RXI) and operations staff compared PPMC’s medication list to the approved Oregon ED prepack formulary. For each prepack, the electronic prescribing (ERX) build in Epic was reviewed and modified to ensure that the ERX identifier, the custom National Drug Code (NDC), and the automated dispensing system (Pyxis) entries matched exactly. A secure storage area was designated in the ED and prepacks were labeled with date b‑ased serial numbers as described in the policy, ensuring that documentation in the medication administration record captured the unique prepack number, drug details, and prescriber information. In Phase 2, the team discovered a knowledge gap: central pharmacy staff were unfamiliar with how to use Epic translation functions and TelRx to support patients with limited English proficiency‑ or visual impairments. Finally, because each facility had been reconciling prepack usage differently, the project created a reconciliation process from scratch. Paper reconciliation was replaced by an electronic method. Results: Phase 1 led to accurate ED prepack orders from Epic to Pyxis and a consistent formulary list with the OR region. Phase 2 improved staff knowledge in translation and TelRx. Preliminary reconciliation data show that documentation errors improved from 20-30% to less than 5%. Additional outcome measures such as staff feedback, workflow efficiency, and medication error rates will be assessed; final results will be presented at the conference. Conclusions: Standardizing the ED prepack program required aligning the local formulary and dispensing systems with regulatory expectations, addressing communication and accessibility barriers, and instituting a working reconciliation process. The project demonstrates that electronic tools, staff education, and process redesign can bring PPMC’s ED prepack practices into compliance with Oregon administrative rules and a regional standard operating procedure. Future work will evaluate long-term‑ effects on patient safety and operational efficiency. IRB status: Exempt
-
Short duration antimicrobial therapy for non-staphylococcal Gram-positive bacteremia (SHORT-STOP)
Mason Melbuer, PharmD; Gregory B. Tallman, PharmD, MS, BCPS, BCIDP; Emily Fox; and Soraya Hobart, PharmD
Recent clinical trials have demonstrated non-inferiority of shorter antibiotic courses for many infections, including gram-negative bacteremia. Longer courses were associated with numerically fewer deaths in the gram-positive subgroup of the BALANCE trial; however, only ~15% of the cohort had streptococcal or enterococcal bacteremia. Conversely, other retrospective studies have demonstrated comparable mortality in uncomplicated streptococcal or enterococcal bacteremia but many of these studies targeted narrow populations, limited pathogens, or were susceptible to confounding variables. The purpose of this study is to determine if patients with uncomplicated non-staphylococcal gram-positive bacteremia can be safely managed with short course antimicrobial therapy. This is a retrospective, multicenter cohort study examining adult (age >= 18 years) patients admitted for an uncomplicated non-staphylococcal gram-positive bloodstream infection blood stream infection from 9/1/2024 to 9/1/2025 at 8 hospitals within a multistate health system. Patients were excluded if they were diagnosed with an active infection requiring prolonged duration of therapy (eg. endocarditis, osteomyelitis), presence of prosthetic material or endovascular grafts, if blood cultures suggest contamination, or if diagnosed with polymicrobial bacteremia. The primary outcome was 30-day all-cause mortality. Secondary outcomes include recurrent bacteremia and Clostridioides difficile infections; all outcomes were assessed at 30 and 90 days. Patient sex, age, ethnicity, comorbidities, organism identified, length of hospital stay, source of infection, and formal infectious disease consult will be collected as well. Patient characteristics were summarized with descriptive statistics. Differences between short and long course therapy were compared using chisquare, Fisher’s exact, Wilcoxon rank-sum, and Student’s t-tests as appropriate. Multivariable logistic regression will be used to model the relationship between treatment duration and outcome, with results reported as odds ratios and associated 95% confidence intervals. Variable selection was determined a priori based on expert input. Approximately 693 patients were examined; preliminary data was collected through electronic extraction and manual chart review of patients’ electronic health records. Approximately 61.6% of patients were male and the most common organisms isolated were Streptococcus pyogenes, Streptococcus pneumoniae, and Enterococcus faecalis. Full results and conclusions will be shared when the project is completed. The study was determined to be exempt from IRB review. Learning objective: Identify the optimal antimicrobial duration in those diagnosed with uncomplicated, non-staphylococcal, Gram-positive bacteremia. Category: Infectious disease
-

Addressing Food Insecurity through partnering with the Community Teaching Kitchen on Lifestyle Medicine Hypertension Class
Emily Miyasako and Jill Christensen
Background: Food insecurity is defined as limited or unreliable access to adequate and nutritious food. In Oregon, approximately 1 in 8 residents experience food insecurity, with rates disproportionately affecting low-income individuals, racial and ethnic minorities, and households with children or elderly individuals. Food insecurity remains a significant threat to our patients’ health and is associated with obesity, malnutrition, and poor mental health. As a primary care provider, I have seen the effects of food insecurity on my patients, but I am thankful for the presence of our Community Teaching Kitchen. The Community Teaching Kitchen (CTK) at Providence Milwaukie provides nutritional counseling, operates a community garden that provides a sustainable source of fresh produce, and manages a family food pantry providing nutritious foods available to patients experiencing food insecurity. CTK serves a vital role in providing reliable access to healthy foods for individuals in our community. However, after HR 1 was passed in July 2025, SNAP benefits were significantly reduced. This severely impacted CTK’s ability to help support our community due to decreased funding and increased need. Our clinic has been implementing a group hypertension class as part of the lifestyle medicine elective. My passion project involved partnering with the CTK for the lifestyle medicine group hypertension class to help provide revenue for the CTK and the family food pantry, while also introducing our patients to this valuable resource. Goals and objectives: To introduce our patients to the services offered by the Community Teaching Kitchen, as well as to create a sustainable source of revenue for the Community Teaching Kitchen so they can continue to provide nutritious food for our patients with food insecurity. Methods: We adapted the 4-week lifestyle medicine group hypertension course to incorporate services offered by CTK. The classes are scheduled on 3/11, 3/18, 3/25 and 4/1. One of the sessions of the class will be held in the community garden, where we will discuss the importance of exercise and demonstrate a meditation class. The final session will be held at the teaching kitchen, where we will demonstrate how to cook a DASH diet meal by using resources and a recipe provided by the CTK staff. We will measure patient learning and satisfaction with pre and post-course surveys. Results: In order to increase recruitment, I personally reached out to my panel of patients who had uncontrolled hypertension via Mychart messages. We were able to recruit 7 patients (of which 6 attended the first class), thereby meeting our goal of 6-8 participants. We will be able to share the proceeds of the class (each session is billed as a level 3 visit) with our Community Teaching Kitchen, which will be able to fund the family food pantry. We have collected pre-course survey on baseline hypertension knowledge and plan to compare this to post-course survey results to evaluate patient learning. We will also analyze patient satisfaction scores on the post-course survey. Discussion/conclusion: Food insecurity is a highly prevalent yet under-addressed determinant of health among our patients. Our Community Teaching Kitchen has been essential in helping our patients with food insecurity by providing nutritious food and dietary counseling. By partnering with the CTK for our group lifestyle medicine hypertension class, we can introduce our patients to this valuable resource as well as provide a sustainable source of income for our community food pantry to continue to support our patients with food insecurity.
-

Improving Recognition of Chronic Kidney Disease in a Federally Qualified Health Center Through a Quality Improvement Initiative
Rachel Monroe, Evan Saulino, and Kathleen McKenna
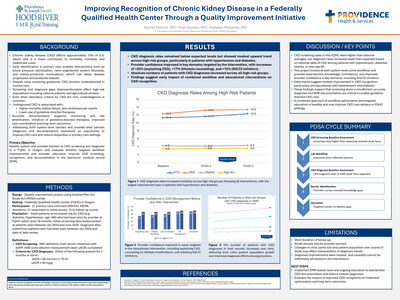
Context/background: Chronic kidney disease (CKD) affects approximately 15% of adults in the United States, yet nearly 90% of affected individuals are unaware of their diagnosis. Early identification in primary care enables interventions such as blood pressure optimization, renin –angiotensin system blockade, and kidney -protective medications that can significantly delay disease progression and postpone dialysis. Screening and diagnosis gaps disproportionately affect high -risk populations, including Latinx patients and immigrant agricultural workers commonly served in federally qualified health centers (FQHCs). National CKD screening rates among patients with diabetes or hypertension remain low, leaving many high -risk individuals unscreened for kidney disease. Improving CKD screening and recognition in primary care is critical to reducing disparities and preventing progression to advanced kidney disease. Objective: To identify system and provider barriers to CKD screening and diagnosis in a FQHC in Oregon and evaluate whether targeted workflow improvements and provider education improve CKD screening, recognition, and documentation in the electronic medical record (EMR). Methods: Quality improvement project conducted primarily in an FQHC in Hood River, Oregon using iterative Plan -Do-Study -Act (PDSA) cycles. PDSA cycle 1 established baseline CKD screening rates using EMR data among patients seen within the previous 18 months and at increased risk for CKD. Screening was defined as having both serum creatinine/eGFR and urine albumin test results in the EMR. Screening rates ranged from 53–68% across risk groups and 54% overall, substantially higher than national estimates. PDSA cycle 2 evaluated laboratory workflows affecting urine specimen collection for albuminuria testing and implemented process adjustments to improve specimen collection reliability. PDSA cycle 3 compared expected CKD prevalence in high -risk populations with documented diagnoses in the EMR, revealing lower -than- expected diagnosis rates (9.4% vs expected 25–30% among patients with hypertension and 12.3% vs expected 30–40% among patients with diabetes). PDSA cycle 4 surveyed clinicians regarding barriers to CKD diagnosis; 21 of 41 clinicians responded (12 MD/DO, 6 NP/PA, 3 residents). Areas of lowest confidence included explaining CKD diagnosis and prognosis, counseling on lifestyle modification, initiating SGLT2 inhibitors, and determining when to refer to nephrology. PDSA cycle 5 implemented a targeted educational session addressing these gaps, followed by a repeat survey (15 responses). Results: Post-intervention survey responses demonstrated increased provider comfort in several previously identified areas. The proportion of clinicians selecting the two highest Likert -scale categories increased for explaining CKD diagnosis and prognosis (71% [15/21] to 93% [14/15]), counseling patients on lifestyle modification (76% to 93%), and initiating SGLT2 inhibitors (81% to 93%). Preliminary EMR review suggests increasing CKD problem list documentation among high -risk patients following the intervention; additional pre/post analysis is ongoing. Discussion/conclusions: In this FQHC population with relatively strong CKD screening rates, underdiagnosis remained a significant care gap. A structured quality improvement approach addressing both workflow and provider barriers improved clinician confidence and may increase CKD recognition in primary care. Improving CKD documentation in the EMR supports earlier guideline -directed management and represents a feasible strategy for strengthening CKD care in community health centers.
-

An Atypical Presentation of Metastatic Gastric Adenocarcinoma Due to Pulmonary Lymphangitic Carcinomatosis
Matthew Moritz and Omar Pandhair
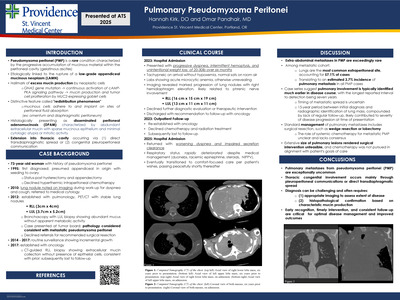
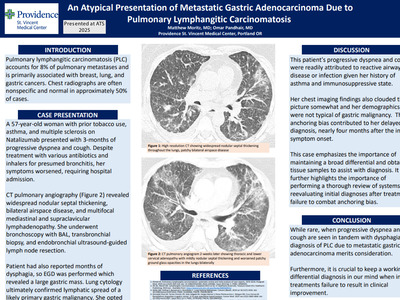
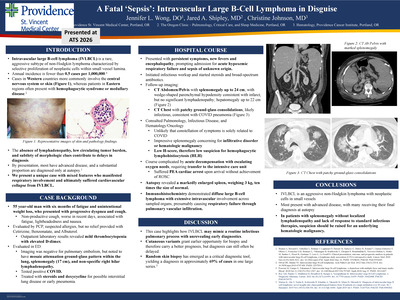
Pulmonary lymphangitic carcinomatosis (PLC) accounts for approximately 8% of pulmonary metastases and is primarily associated with breast, lung, and gastric cancers. Chest radiographs are often nonspecific and normal in approximately 50% of cases. We present a case of PLC as an initial presentation of metastatic gastric adenocarcinoma. A 57-year-old White woman with prior tobacco use, asthma, and multiple sclerosis on Natalizumab presented with three months of progressive dyspnea and cough. She was evaluated multiple times and treated with various antibiotics and inhalers for presumed bronchitis. Despite this, her symptoms worsened, prompting hospital evaluation. She was tachycardic and markedly hypoxemic on arrival. A high-resolution computed tomography (CT) scan revealed widespread nodular septal thickening, bilateral airspace disease, and multifocal mediastinal and supraclavicular lymphadenopathy most concerning for lymphoma or atypical infection. She underwent bronchoscopy with bronchoalveolar lavage, transbronchial biopsy, and endobronchial ultrasound guided lymph node resection. She also reported progressive dysphagia with solid foods and significant weight loss over the prior months, so esophagogastroduo denoscopy was performed with pathology showing a poorly differentiated adenocarcinoma. Lung cytology confirmed lymphatic spread of a likely primary gastric malignancy. She opted to discharge on hospice. Given our patient’s asthma and immunosuppressive therapy, her progressive dyspnea and cough were easily readily attributed to reactive airway disease or infection. Her chest imaging findings also clouded the picture somewhat and her demographics were not typical of gastric malignancy as it is half as common in women and has very low prevalence in the non-Hispanic White population. Natalizumab therapy was also not associated with increased risk of malignancy in a recent cohort study. This anchoring bias contributed to her delayed diagnosis, as her weight loss and dysphagia were not uncovered until she was hospitalized, four months after the initial symptom onset. In a similar case, a man presenting with respiratory symptoms whose imaging showed only bilateral ground-glass opacities was felt to have non-malignant disease until trans-bronchial biopsy revealed metastatic gastric adenocarcinoma. Both cases emphasize the importance of maintaining a broad differential and obtaining tissue samples to assist with diagnosis. Our case highlights the importance of performing a thorough review of systems and reevaluating initial diagnoses after initial treatment failure to combat anchoring bias. When progressive dyspnea and cough are seen in tandem with dysphagia, the otherwise very rare diagnosis of PLC due to metastatic gastric adenocarcinoma merits consideration.
-

Ceftriaxone-Induced Thrombocytopenia: An Atypical Presentation of a Commonly Used Antibiotic
Matthew Moritz and Omar Pandhair
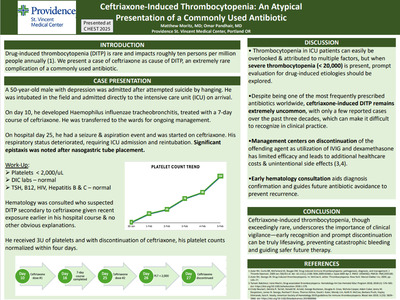
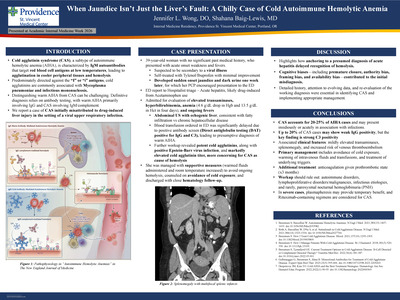
INTRODUCTION: Drug-induced thrombocytopenia (DITP) is rare and impacts roughly ten persons per million people annually (1). Over one-hundred medications have been identified as possible offenders, with immune response occurring within one to two weeks of drug exposure (2). Here we present a case of ceftriaxone as cause of DITP, an extremely rare complication of a commonly used antibiotic. CASE PRESENTATION: A fifty-year-old male with diabetes and depression initially presented after attempted suicide by hanging. He was intubated in the field and admitted directly to the intensive care unit (ICU). He remained in the ICU due to persistent encephalopathy which was confounded by polysubstance withdrawal and brain anoxia. His course was complicated by Haemophilus influenzae tracheobronchitis which was treated with a seven-day course of ceftriaxone. This was completed on day sixteen of his hospital course. He was eventually extubated and transferred to the hospitalist service. On hospital day twenty-five, he suffered a seizure and suspected aspiration event, and again ceftriaxone was administered to cover for potential aspiration pneumonia. He became more tachypneic, lethargic, and febrile so was transferred back to the ICU and reintubated. Epistaxis was noted after nasogastric tube placement. The following morning, his laboratory studies revealed a platelet count of< 2,000/uL. His heparin-induced thrombocytopenia (HIT) "4T" score suggested a low probability of HIT and additional studies ruled out disseminated intravascular coagulation; TSH, B12, HIV, Hepatitis C, and Hepatitis B were all negative as well. Hematology was consulted who felt this was most consistent with DITP due to ceftriaxone given recent exposure earlier in his hospital course. He received three units of platelets and with discontinuation of ceftriaxone, his platelet counts normalized within four days. DISCUSSION: Thrombocytopenia occurs frequently in patients admitted to the intensive care unit and is often attributed to sepsis, critical illness, and bone marrow suppression. However, a platelet count< 20,000/uL should raise suspicion for a more sinister process. Despite being one of the most used antibiotics, ceftriaxone is rarely the culprit of DITP, with only a handful of case reports identified in the literature over the past thirty years. Our case emphasizes the importance of discontinuation of the offending agent (i.e ceftriaxone) with as-needed platelet transfusions to avoid bleeding complications. Contrary to previous case reports, utilization of intravenous immunoglobulin and dexamethasone, which has only shown to be beneficial in case reports of DITP and primary ITP respectively, is unnecessary and can lead to additional healthcare costs and unintentional side effects (3,4). We also demonstrated benefits of early hematology consultation, which supported the management approach and helped confirm the DITP diagnosis, particularly emphasizing the avoidance of ceftriaxone in the future to prevent a potentially fatal recurrence. CONCLUSIONS: Thrombocytopenia is a commonly encountered diagnosis; however, ceftriaxone-induced thrombocytopenia is extremely rare. DITP should be on the differential diagnosis especially when platelet counts drop below 20,000/uL. When suspected, offending medications should be promptly discontinued to avoid serious, life-threatening bleeding complications.
-

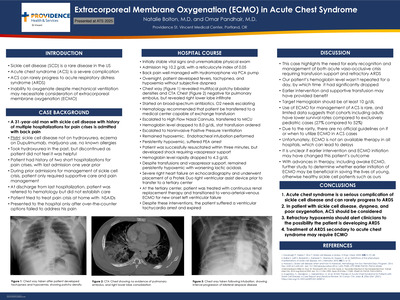
ECMO as a Bridge to Lung Transplant for Refractory Rapidly Progressive Interstitial Lung Disease
Matthew Moritz and Omar Pandhair
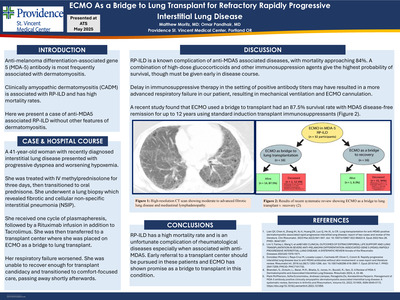
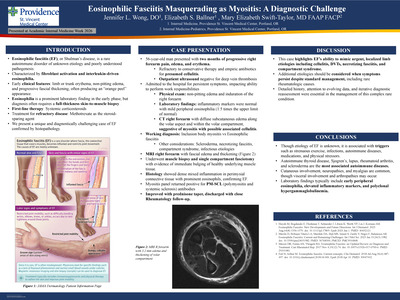
Anti-melanoma differentiation-associated gene 5 (MDA-5) antibody is most frequently associated with dermatomyositis with various degrees of clinical manifestations including rapidly progressive interstitial lung disease (RP-ILD), inflammatory arthritis, vasculopathy, and other cutaneous findings. Clinically amyopathic dermatomyositis (CADM) is frequently associated with RP-ILD and has high mortality rates. Here we present a case of anti-MDA5 associated RPILD but without other features of dermatomyositis that did not respond to standard immunosuppressive therapy. A 41-year-old woman with recently diagnosed interstitial lung disease and polyarthritis previously on methotrexate presented with progressive dyspnea and worsening hypoxemic respiratory failure. She was previously admitted for respiratory failure two months prior where high resolution CT revealed moderate to advanced fibrotic lung disease and mediastinal lymphadenopathy and was discharged on a prolonged prednisone taper. Previous studies revealed a positive MDA5 antibody. She was treated initially with intravenous methylprednisolone 1,000 mg for three days then transitioned to oral prednisone. Lung biopsy revealed fibrotic and cellular non-specific interstitial pneumonia (NSIP). She received one cycle of plasma pheresis, followed by a Rituximab infusion in addition to Tacrolimus. She was then transferred to a transplant center where she was placed on veno-arterial venous extracorporeal membrane oxygenation (ECMO) as a bridge to lung transplant. Unfortunately, her respiratory failure worsened, requiring ECMO reconfiguration. She was unable to recover enough for transplant candidacy and transitioned to comfort-focused care, passing away shortly afterwards. RP-ILD is a known complication of anti-MDA5 associated diseases, with mortality approaching 84%. A combination of high-dose glucocorticoids and other immunosuppression agents give the highest probability of survival, though they must be administered early in the disease course. Our patient had a delay in additional immunosuppressive therapy, despite positive antibody titers two months prior, which may have resulted in a more advanced respiratory failure and hypoxemia on presentation, ultimately requiring mechanical ventilation and subsequent ECMO cannulation. A systematic review published in Annals of Rheumatology found that ECMO used a bridge to transplant had an 87.5% survival rate with MDA5 disease-free remission for up to 12 years using standard induction transplant immunosuppressants, which a more recent case report in CHEST exemplified. Our case emphasizes the importance of early antibody screening and prompt initiation of appropriate immunosuppressive therapy to avoid transformation to RP-ILD. Early referral to a transplant center should be pursued in these patients as ECMO has shown promise as a bridge to transplant in this condition.
-

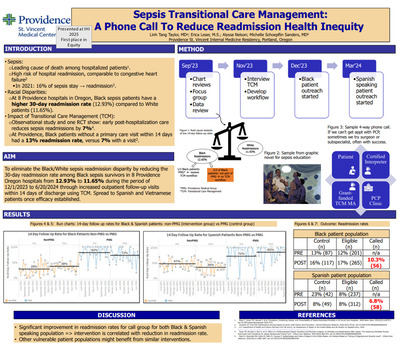
An Exploration of Drivers of Sepsis Outcomes in Racial and Ethnic Minority Populations
Matthew Moritz, Omar Pandhair, and Shelley Schoepflin Sanders
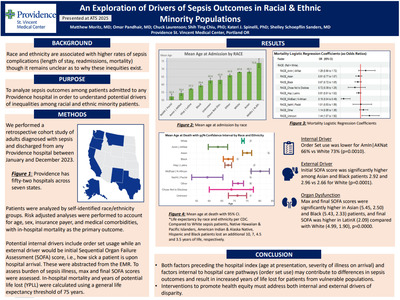
RATIONALE: Race and ethnicity affect sepsis outcomes in unclear ways. Existing data is conflicting, with some studies suggesting minority patients do worse, while others did not show a difference in outcomes between these groups. We sought to investigate whether inequalities exist in sepsis outcomes for different racial and ethnic groups in our large hospital system and to characterize how they may manifest. METHODS: We performed a retrospective cohort study of adults diagnosed with sepsis and discharged from any of Providence’s 52 hospitals between January 1 and December 31, 2023. We grouped patients into ten different race/ethnicity groups including White, Black, Hispanic/Latinx, Black, Asian, Middle Eastern/North African, American Indian/Alaska Native, and other/ unknown/chose not to disclose. Patient age, gender, insurance payer, and medical comorbidity groups were determined. In-hospital mortality, hospital length of stay (LOS), 30-day readmission rate, lactic acid level, sepsis order set usage, and initial, final, and maximum sequential organ failure assessment (SOFA) scores were abstracted from the electronic medical record. RESULTS: We identified 44,443 sepsis patients, of whom the mean age was 65.3 years and 52.7% were male. 65.2% were White, 17.0% were Hispanic/Latinx, 5.2% were Asian, 4.1% were Black, and 1.3% were Native American. White (67.9 years) and Asian (68.1 years) patients were of similar average age, while Black (59.4 years), Hispanic (57.2 years), and Native American (54.4 years) patients were younger. Hispanic/ Latinx patients had a 2.46% lower mortality rate (p < 0.0001) than White patients. Black patients had a LOS of 0.63 days longer (p < 0.0001) than White patients on average, while Hispanic patients had a 0.51-day shorter LOS (p< 0.0001). Readmission rates were similar across groups. Black and Asian patients had higher initial, maximum, and final SOFA scores than Whites (p < 0.0001). Asian patients also had a higher lactic acid level by 0.13 mmol/L (p = 0.0001) than White patients. CONCLUSIONS: We noted a significant difference in the average age of each race/ethnicity group, meaning that despite similar mortality rates, Black and Native American patients on average present and die younger of sepsis than White patients. Similarly, age may account for much of the mortality benefit associated with the Hispanic/Latinx group. Further study investigating years of potential life lost may help better elucidate these disparities. Disparities in the severity of presenting illness of Black and Asian patients may be due to delayed recognition in the prehospital setting.
-

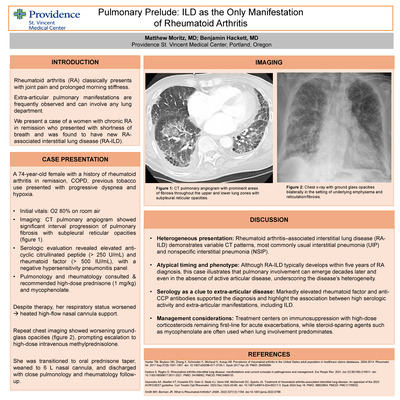
Pulmonary Prelude: ILD as the Only Manifestation of Rheumatoid Arthritis
Matthew Moritz, MD and Benjamin Hackett
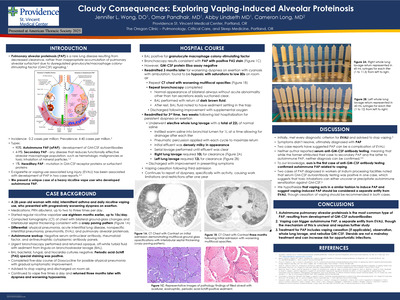
Abstract: Rheumatoid arthritis (RA), a systemic autoimmune disorder, classically presents with joint pain and prolonged morning stiffness. Extra-articular pulmonary manifestations are frequently observed but can be the primary initial presentation. We present a case of a women with chronic RA in remission who presented with shortness of breath and was found to have new RA-associated interstitial lung disease (RA-ILD). A 74-year-old female with a history of rheumatoid arthritis in remission, chronic obstructive pulmonary disease, and recent admission for septic shock presented with progressive dyspnea and hypoxia. Initial vitals noted an oxygen saturation in the low 80s. CT pulmonary angiography excluded pulmonary embolism but demonstrated significant interval progression of basilar predominant pulmonary fibrosis with subpleural reticular opacities compared to imaging seven months prior. Pulmonology was consulted and recommended high-dose prednisone (1 mg/kg). Serologic evaluation revealed elevated anti-cyclic citrullinated peptide(> 250 U/ml) and rheumatoid factor(> 500 IU/ml), with a negative hypersensitivity pneumonitis panel. Rheumatology agreed with mycophenolate monotherapy given lack of synovial involvement. Despite therapy, her respiratory status declined, necessitating heated high-flow nasal cannula support. Repeat chest imaging showed worsening ground-glass opacities, prompting escalation to high-dose intravenous methylprednisolone, which led to gradual clinical improvement. She transitioned to an oral prednisone taper, weaned to 6 L nasal cannula, and discharged with close pulmonology and rheumatology follow-up. RA-ILD chest CT findings are variable but most commonly demonstrate usual interstitial pneumonia (UIP) or nonspecific interstitial pneumonia (NSIP) patterns, although organizing pneumonia and rheumatoid nodules are also well described. While RA-ILD typically develops within five years of RA onset, our patient exhibited pulmonary manifestations decades after diagnosis, highlighting the marked heterogeneity in disease presentation. Furthermore, the absence of articular involvement further distinguishes this case, as most patients with RA-ILD exhibit at least some degree of joint disease. The presence of markedly elevated rheumatoid factor and anti-cyclic citrullinated peptide (anti-CCP) antibodies supported the diagnosis in this case and aligned with known associations between serologic activity and extra-articular disease expression. Current treatment strategies for RA-ILD emphasize systemic steroids and DMARDs, and like our patient, most receive high-dose steroids for management of acute flare, though augmentation with mycophenolate was selected given the predominance of pulmonary involvement. Since there are no dedicated randomized controlled trials in this area, treatment is based on observational data and expert opinion and should include a multidisciplinary approach to optimize patient outcomes.
-

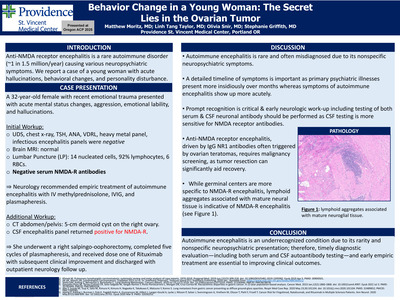
Behavior Change in a Young Woman: The Secret Lies in the Ovarian Tumor
Matthew Moritz, MD; Linh Tang Taylor, MD; Olivia L Snir; and Stephanie Griffith, MD
Introduction: Autoimmune encephalitis is a rare immune-mediated disorder characterized by neuropsychiatric symptoms. Anti-NMDA receptor (NMDA-R) encephalitis, the most common subtype, affects approximately 1 in 1.5 million people annually. We present a case of a young female with new-onset hallucinations, behavioral changes, and personality disturbance. Case Presentation: A 32-year-old female with remote methamphetamine use and recent trauma presented with acute mental status changes, aggression, emotional lability, and hallucinations. Vitals were normal; on exam she appeared confused, agitated, and displayed unusual behavior, including hallucinations. Initial evaluation revealed mild leukocytosis, but otherwise normal urine drug screen, chest radiograph, TSH, ANA, VDRL, heavy metal panel, infectious and autoimmune encephalitis panels, and brain MRI. Lumbar puncture (LP) revealed fourteen nucleated cells, ninety-two percent lymphocytes, and six red blood cells. Psychiatry was consulted but felt this was unlikely to represent a primary psychiatric disorder. Neurology recommended repeat LP and initiation of empiric methylprednisolone, IVIG, and plasmapheresis for presumed autoimmune encephalitis. CT abdomen/pelvis revealed a five-centimeter dermoid cyst on the right ovary. She underwent right salpingoopherectomy with pathology showing a cystic teratoma with mature neuronal tissue. The CSF encephalitis panel returned positive for NMDA-R. She completed five sessions of plasmapheresis and one dose of rituximab induction. Her agitation and behavioral disturbances were slow to resolve, requiring high-dose antipsychotics and benzodiazepines, but she was ultimately discharged with close outpatient neurology follow -up and a plan for a second rituximab dose. Discussion: Due to its rarity and nonspecific symptoms, autoimmune encephalitis is often overlooked in clinical practice. Furthermore, our patient’s age and recent traumatic experience prompted a primary psychiatric diagnosis to be pursued. This case underscores the importance of assessing symptom onset, as primary psychiatric disorders such as schizophrenia or bipolar disorder typically present with a more gradual, insidious onset— unlike the acute presentation seen in our case. When suspected, a basic workup should include a brain MRI, lumbar puncture, and neuronal autoantibody testing, though brain MRI findings may be normal. Both serum and CSF should be tested for neuronal autoantibodies, as CSF offers greater sensitivity—particularly for NMDA receptor antibodies, as demonstrated in our case where only CSF testing yielded a positive result. In anti-NMDA receptor encephalitis, IgG antibodies against NR1 are often triggered by neural tissue in ovarian teratomas via molecular mimicry. Once autoimmune encephalitis is diagnosed, evaluation for an underlying malignancy should follow, as treatment of a paraneoplastic process is integral to disease management. In our case, an ovarian teratoma—commonly associated with anti-NMDA receptor encephalitis—was identified and resected, contributing to clinical improvement
-
Evaluation of SAVED/IMPEDE risk assessment models for VTE prophylaxis in multiple myeloma patients
Rina Mullendore, PharmD and Ian Ingram, PharmD, BCOP
Abstract: Venous thromboembolism (VTE) is a significant complication in patients with multiple myeloma. The National Comprehensive Cancer Network (NCCN) Multiple Myeloma guidelines recommend administering VTE prophylaxis for eligible patients if there are no contraindications to anticoagulation or antiplatelet agents. Current VTE prophylaxis recommendations are guided by the SAVED and IMPEDE scores, which are tools used to predict the risk of VTE in patients with multiple myeloma. The primary purpose is to determine the incidence of VTE, stratified by IMPEDE/SAVED score, in patients with multiple myeloma receiving treatment at Providence Cancer Institute Franz Clinic. EPIC will be queried using SlicerDicer to identify patients diagnosed with multiple myeloma who are actively receiving treatment at Providence Cancer Institute Franz Clinic. Exclusion criteria include research participants, patients already on an anticoagulation or antiplatelet agent for other prescribed indications, and patients not being actively treated for multiple myeloma. A report will be generated that includes potential patients for study inclusion. Additional reports will be generated to identify patients who have a VTE diagnosis, on aspirin or an anticoagulation agent, and other variables that are important for IMPEDE/SAVED score calculation such as age, immunomodulatory drug therapy, Asian race, BMI, pelvic/hip/femur diagnosis, surgery within the last 90 days, erythropoiesis-stimulating agents, dexamethasone dose, doxorubicin, tunneled line or central venous catheter, and existing thromboprophylaxis (therapeutic or prophylaxis). The IMPEDE/SAVED score will be calculated for patients to identify whether patients were on an appropriate prophylactic agent, indexed to their Cycle 1, Day 1 treatment, based on the calculated IMPEDE/ SAVED score per NCCN guidelines. For patients with a VTE diagnosis, it will be determined if the VTE occurred before or after the initiation of multiple myeloma treatment. Adverse events related to VTE prophylaxis (clinically relevant bleeding) will also be reported. IRB status is exempt. Data is currently being collected. Results and conclusions will be shared when the project is completed. Presentation category: Hematology/oncology/immunology/transplant
-
Impact of restricting medication auto-verification on patient safety in the emergency department
Anthony Nguyen, PharmD; Savita Bathija, PharmD, BCEMP; and Jessica Dizon-Scheer, PharmD, MHA, BCPS
Abstract: When Providence Portland Medical Center (PPMC) first transitioned to an electronic health record system, most Emergency Department (ED) medication orders were signed by licensed prescribers and bypassed pharmacist review. Only a small list of high‑risk medications required pharmacist verification prior to dispensing. While this workflow supported rapid medication availability, it also introduced potential patient‑safety risks due to limited pharmacist oversight. In August 2024, PPMC revised its ED medication verification policy. Under the new process, nearly all medications require pharmacist review before dispensing, with exceptions for a small group of low‑risk, time‑sensitive emergent agents that may still be auto‑verified. This change aimed to enhance medication safety while preserving ED efficiency. However, the impact of this policy shift has not been evaluated. This IRB‑approved, single‑center pre–post observational study assessed the effects of this revised process. A preliminary review of reports from Providence’s medication event reporting system identified ceftriaxone as the medication most frequently associated with safety events at PPMC’s ED. We included and compared ED ceftriaxone orders for adults (≥18 years) that were auto‑verified between August 2023–August 2024 and pharmacist‑verified ceftriaxone orders between August 2024–August 2025. Orders were excluded if the patient did not receive ceftriaxone in the ED or was younger than 18 years from our analysis. Primary outcomes included surrogate safety measures: total medication safety events associated with ceftriaxone pre and post revised verification process. Secondary outcomes included ceftriaxone safety events per 1,000 medication orders or ED visits, safety event type (duplication, incorrect dose, incorrect indication, incorrect timing), number of number of documented pharmacist antimicrobial stewardship interventions number and percentage of ED orders prospectively reviewed by a pharmacist, and time from verification to ceftriaxone administration pre and post implementation. This study is currently ongoing. Results and conclusions will be shared when the project is completed. Presentation Category: Medication safety/quality improvement
-
Evaluating the clinical, operational, and financial opportunities for developing a pharmacist-led iron infusion clinic
Yasasvi Obeyesekera, PharmD; Stephanie Matta, PharmD, BCOP; and Shuntao Cai, PharmD
Abstract: Iron deficiency anemia (IDA) affects more than three million individuals in the United States and frequently requires intravenous (IV) iron therapy when oral iron is ineffective due to malabsorption, intolerance, or the need for rapid repletion. At many health systems, patients requiring IV iron are routinely referred to hematology specialists, even when cases could potentially be managed in a primary care or pharmacist-led setting. This practice can lead to delays in treatment due to limited specialist availability and inefficient utilization of healthcare resources. Pharmacist-provider collaborative clinics have demonstrated success in improving access to care and optimizing medication management in various disease states. The purpose of this project is to evaluate current IV iron utilization patterns and identify clinical, operational, and financial opportunities to support the development of a pharmacist-led iron infusion clinic. This study is a single-center, retrospective pre–post analysis of adult patients re ceiving IV iron at Providence Franz Clinic and Providence Cancer Institute (PCI) West Clinic. Pre-intervention data was collected from February 2, 2025, through August 19, 2025, and post-intervention data will be collected following imple mentation of a pharmacist-led IV iron clinic. Eligible patients include adults ≥18 years old with absolute or functional iron deficiency referred by hematology providers and treated with IV iron formulations. Patients receiving hemodialysis or meeting other exclusion criteria will be excluded. Data collected includes or dered iron formulations, number of administrations per patient, infusion time, treatment cost, and associated net margins. The primary objective is to evaluate current IV iron prescribing patterns and cost margins for each formulation. Secondary objectives include identifying operational opportunities for a pharmacist-led clinic through estimating potential physician visits saved and evaluating opportunities to streamline formulary prescribing. Pre-intervention analysis included 221 patients treated with IV iron formulations across both clinics. Results from the post-intervention period will be analyzed to assess the impact of pharmacist-led management on clinical workflow, resource utilization, and financial outcomes. Findings from this study may support implementation of pharmacist-led infusion services to improve efficiency, patient access, and health system resource allocation. Learning objectives: Describe current utilization patterns of intravenous iron formulations in an outpatient oncology and infusion clinic setting. Evaluate clinical, operational, and financial considerations for implementing a pharmacist led intravenous iron infusion clinic.
-

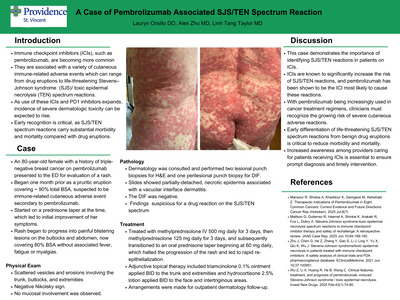
A Case of Pembrolizumab Associated SJS/TEN Spectrum Reaction
Lauryn Orsillo, DO; Alex Zhu, MD; and Linh Tang Taylor, MD
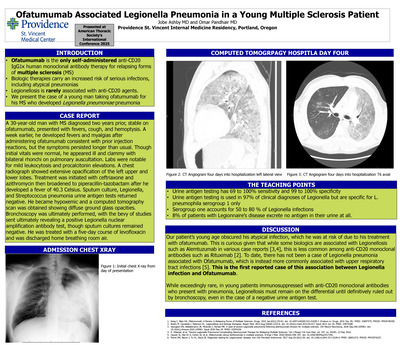
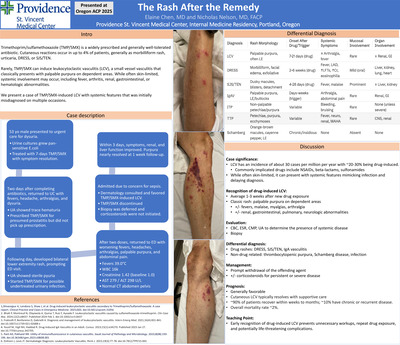
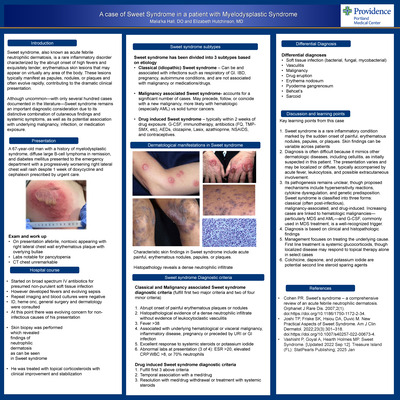
Introduction: Immune checkpoint inhibitors (ICIs), such as pembrolizumab, are becoming increasingly more common.1 They are associated with a variety of cutaneous immune-related adverse events which can range from drug eruptions to life-threatening Stevens–Johnson syndrome (SJS)/ toxic epidermal necrolysis (TEN) spectrum reactions.2 As use of these ICIs and PD1 inhibitors expands, the incidence of severe dermatologic toxicity can be expected to rise. Early recognition is critical, as SJS/TEN spectrum reactions carry substantial morbidity and mortality compared with drug eruptions. Case report: An 80-year-old female with a history of triple-negative breast cancer on pembrolizumab presented to the ED for evaluation of a worsening rash. She reported that the rash began approximately one month earlier as a pruritic eruption covering an estimated 90% total body surface area. Her oncologist suspected an immune-related cutaneous adverse event secondary to pembrolizumab, with her most recent dose administered one month prior to rash onset. She was started on a prednisone taper, which led to initial improvement of her symptoms. A few days prior to presentation, while still receiving the prednisone taper, the rash progressed and evolved into painful blistering lesions on the buttocks and abdomen, now covering 80% total body surface area. She denied associated fever, fatigue or myalgias. Physical examination revealed scattered vesicles and erosions involving the trunk, buttocks, and extremities, with a negative Nikolsky sign. No mucosal involvement was observed. Dermatology was consulted and performed two lesional punch biopsies for H&E and one perilesional punch biopsy for DIF. The slides were interpreted by a dermatopathologist and showed a partially-detached, necrotic epidermis associated with a vacuolar interface dermatitis. The DIF was negative. These findings were suspicious for a drug reaction in the SJS/TEN spectrum. The patient was treated with methylprednisolone IV 500 mg daily for three days, followed by methylprednisolone 125 mg daily for three days, and subsequently transitioned to an oral prednisone taper beginning at 60 mg daily, which halted the progression of the rash and led to rapid re-epithelialization. Adjunctive topical therapy included triamcinolone 0.1% ointment applied twice daily to the trunk and extremities and hydrocortisone 2.5% lotion applied twice daily to the face and intertriginous areas. Arrangements were made for outpatient dermatology follow-up. Discussion: This case demonstrates the importance of identifying SJS/TEN reactions in patients on ICIs. ICIs are known to significantly increase the risk of SJS/TEN reactions, and pembrolizumab has been shown to be the ICI most likely to cause these reactions. 2, 3 With pembrolizumab being increasingly used in cancer treatment regimens, clinicians must recognize the growing risk of severe cutaneous adverse reactions.1 Early differentiation of life-threatening SJS/TEN spectrum reactions from benign drug eruptions is critical to reduce morbidity and mortality. Increased awareness among providers caring for patients receiving ICIs is essential to ensure prompt diagnosis and timely intervention.
-

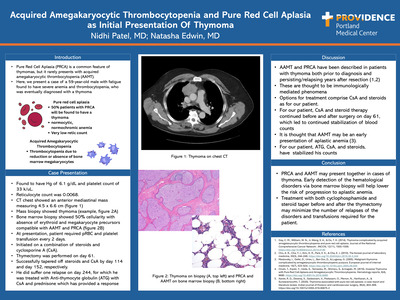
Acquired Amegakaryocytic Thrombocytopenia and Pure Red Cell Aplasia as Initial Presentation Of Thymoma
Nidhi Patel, MD and Natasha Edwin, MD
Introduction: Pure Red Cell Aplasia (PRCA) is a common feature of thymomas, but it rarely presents with acquired amegakaryocytic thrombocytopenia (AAMT). Here, we present a case of a 59-year-old male with fatigue found to have severe anemia and thrombocytopenia, who was eventually diagnosed with a thymoma Case Presentation: Found to have Hg of 6.1 g/dL and platelet count of 33 k/uL; Reticulocyte count was 0.0068. CT chest showed an anterior mediastinal mass measuring 4.5 x 6.6 cm. Mass biopsy showed thymoma. Bone marrow biopsy showed 50% cellularity with absence of erythroid and megakaryocyte precursors compatible with AAMT and PRCA. At presentation, patient required pRBC and platelet transfusion every 2 days. Initiated on a combination of steroids and cyclosporine A (CsA). Thymectomy was performed on day 61. Successfully tapered off steroids and CsA by day 114 and day 152, respectively. He did suffer one relapse on day 244, for which he was treated with Anti-thymocyte globulin (ATG) with CsA and prednisone which has provided a response Discussion: AAMT and PRCA have been described in patients with thymoma both prior to diagnosis and persisting/relapsing years after resection. These are thought to be immunologically mediated phenomena. Options for treatment comprise CsA and steroids as for our patient. For our patient,CsAand steroid therapy continued before and after surgery on day 61, which led to continued stabilization of blood counts. It is thought that AAMT may be an early presentation of aplastic anemia. For our patient, ATG, CsA, and steroid, have stabilized his counts Conclusion: PRCA and AAMT may present together in cases of thymoma. Early detection of the hematological disorders via bone marrow biopsy will help lower the risk of progression to aplastic anemia. Treatment with both cyclophosphamide and steroid taper before and after the thymectomy may minimize the number of relapses of the disorders and transfusions required for the patient
-

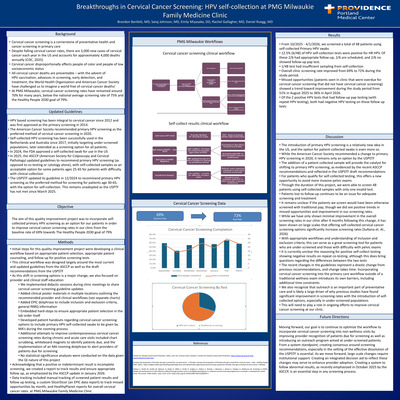
Improving Cervical Cancer Screening at PMG Southeast Family Medicine Through Implementing a New Screening Tool: Patient-Collected High-Risk HPV Screening
Brianna Pickering, August Stuppy, Eric Waelbroeck, Ben Pederson, and Daniel Ruegg
-

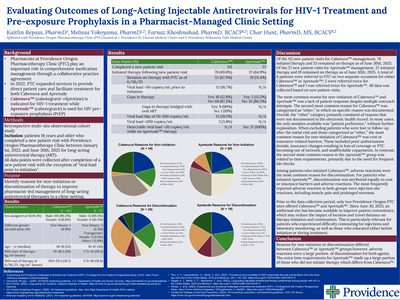
Evaluating Outcomes of Long-Acting Injectable Antiretrovirals for HIV Treatment and Pre-exposure Prophylaxis in a Pharmacist-Managed Clinic Setting
Kaitlin Repass, PharmD; Melissa Yokoyama, PharmD; Farnaz Khoshnahad, PharmD, BCACP; and Char Hunt, PharmD, MS, BCACP
-

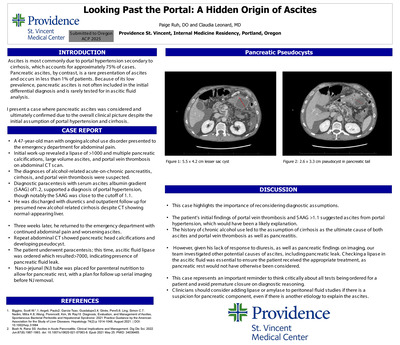
Looking Past the Portal: A Hidden Origin of Ascites
Paige Ruh, DO and Claudia Leonard, MD
Introduction: The most common cause of ascites is portal hypertension secondary to cirrhosis and accounts for nearly 75% of cases. In contrast, pancreatic ascites is a rare presentation of ascites and occurs in less than 1% of patients. Because of its low prevalence, pancreatic ascites is often excluded from the initial differential diagnosis and rarely assessed in ascitic fluid analysis. This is a case in which pancreatic ascites was considered and ultimately confirmed based on the overall clinical picture, challenging the initial assumption of portal hypertension and cirrhosis. Case Presentation: A 47-year-old man with ongoing alcohol use disorder presented to the emergency department with abdominal pain. Initial work-up revealed a lipase >1000 U/L, multiple pancreatic calcifications, large-volume ascites, and portal vein thrombosis on abdominal CT scan. A diagnosis of alcohol -related acute-on-chronic pancreatitis, cirrhosis, and portal vein thrombosis were suspected. Diagnostic paracentesis showed a serum-ascites-albumin gradient (SAAG) of 1.2, supporting portal hypertension, though notably close to the cutoff of 1.1. He was discharged on diuretics and outpatient follow-up for presumed new alcohol related cirrhosis despite CT showing normal-appearing liver. Three weeks later, he returned with persistent abdominal pain and worsening ascites. Repeat CT demonstrated pancreatic head calcifications and a developing pseudocyst. A second paracentesis was performed, and ascitic fluid lipase was ordered, resulting >7000 U/L-- confirming a pancreatic fluid leak. A nasojejunal (NJ) tube was placed for enteral nutrition to allow pancreatic rest, with plans for serial imaging prior to NJ removal. Discussion: This case highlights the importance of reconsidering diagnostic assumptions and recognizing cognitive biases. The patient’s initial findings of portal vein thrombosis and SAAG >1.1 suggested ascites from portal hypertension. The history of chronic alcohol use led to the assumption of cirrhosis as the ultimate cause of both ascites and portal vein thrombosis, with ongoing alcohol use to explain pancreatitis. However, his lack of response to diuresis, as well as pancreatic pseudocysts on imaging, our team investigated other potential causes of ascites, including pancreatic leak. Checking a lipase in the ascitic fluid was essential to ensure the patient received the appropriate treatment, as pancreatic rest would not have otherwise been considered. This case represents an important reminder to think critically about all tests being ordered for a patient and avoid premature closure on diagnostic reasoning. Clinicians should consider adding lipase or amylase to peritoneal fluid studies if there is a suspicion for pancreatic component, even if there is another etiology to explain the ascites
-

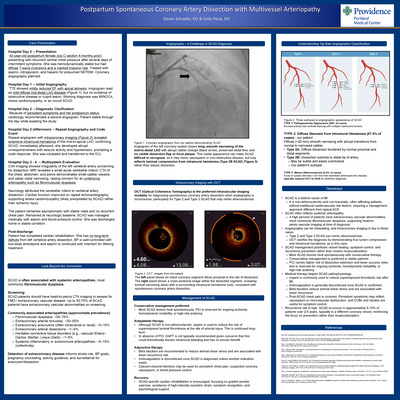
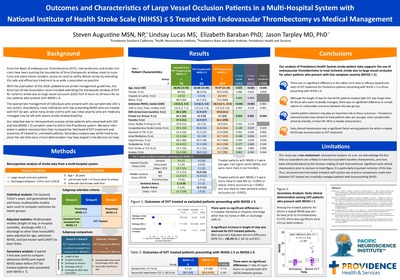
Postpartum Spontaneous Coronary Artery Dissection with Multivessel Arteriopathy
Devon Schaefer, DO and Cody Paiva, DO
Case Presentation: Hospital Day 0 – Presentation: 43-year-old postpartum female (s/p C-section 4-months prior) presenting with recurrent central chest pressure after several days of intermittent symptoms. She was hemodynamically stable but had diffuse T‑wave inversions and a marked troponin rise. Treated with aspirin, nitroglycerin, and heparin for presumed NSTEMI. Coronary angiography planned. Hospital Day 1 -- Initial Angiography: TTE showed mildly reduced EF with apical akinesis. Angiogram read as mild diffuse mid-distal LAD disease (Figure 1), but no evidence of obstructive disease or culprit lesion. Working diagnosis was MINOCA, stress cardiomyopathy, or an occult SCAD. Hospital Day 2 -- Diagnostic Clarification: Because of persistent symptoms and her postpartum status, cardiology recommended a second angiogram. Patient stable through the day while awaiting the study. Hospital Day 2 (Afternoon) -- Repeat Angiography and Code Event: Repeat angiogram with intracoronary imaging (Figure 2) revealed extensive intramural hematoma of the mid‑to‑apical LAD, confirming SCAD. Immediately afterward, she developed abrupt unresponsiveness with seizure activity and hypotension, prompting a code response. She was intubated and transferred to the ICU. Hospital Day 2 - 4 -- Multisystem Evaluation CVA imaging showed irregularity of the left vertebral artery concerning for dissection. MRI revealed a small acute cerebellar infarct. CTA of the chest, abdomen, and pelvis demonstrated small‑caliber vessels and celiac ostial narrowing, raising concern for an underlying arteriopathy such as fibromuscular dysplasia. Neurology attributed the cerebellar infarct to vertebral artery dissection. Cardiac function improved on repeat echocardiography, supporting stress cardiomyopathy (likely precipitated by SCAD) rather than ischemic injury. The patient remained asymptomatic with stable vitals and no recurrent chest pain. Remained at neurologic baseline. SCAD was managed medically with aspirin and blood‑pressure control. She was discharged home in stable condition. Post-discharge: Patient has completed cardiac rehabilitation. She has no long-term deficits from left vertebral artery dissection. BP is well-controlled with low-dose amlodipine and aspirin is continued with intention for lifelong treatment. Takeaways: SCAD is a distinct cause of MI It is non-atherosclerotic and non-traumatic, often affecting patients without traditional cardiovascular risk factors, requiring a management approach different from typical ACS. SCAD often reflects systemic arteriopathy A high percent of patients have extra coronary vascular abnormalities, most commonly fibromuscular dysplasia, supporting head-to-pelvis vascular imaging at time of diagnosis Angiography can be misleading, and intracoronary imaging is key in these cases Type 2 and Type 3 SCAD can mimic atherosclerosis. OCT clarifies the diagnosis by demonstrating true lumen compression and intramural hematoma, as in this case. SCAD management prioritizes vessel healing, symptom control, and recurrence prevention rather than routine revascularization Most SCAD lesions heal spontaneously with conservative therapy. Conservative management is preferred in stable patients PCI carries higher risk of dissection extension and lower success rates, and is reserved for ongoing ischemia, hemodynamic instability, or high‑risk anatomy. Medical therapy targets SCAD pathophysiology Aspirin is commonly used to reduce superimposed thrombotic risk after MI. Anticoagulation is generally discontinued once SCAD is confirmed. Beta blockers reduce arterial shear stress and are associated with lower recurrence Post‑SCAD chest pain is common. Persistent symptoms may reflect vasospasm or microvascular dysfunction, and CCBs and nitrates are useful for symptom control. Recurrence risk is high. SCAD re-occurs in approximately 5-15% of patients over 2-5 years, typically in a different coronary vessel, reinforcing the focus on prevention rather than revascularization.
-

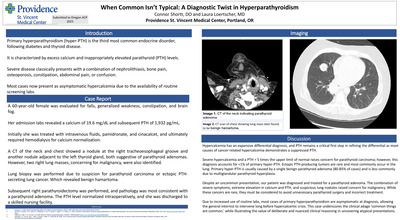
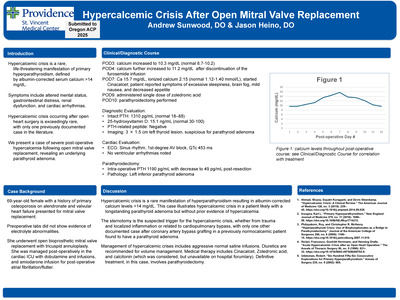
When Common Isn’t Typical: A Diagnostic Twist in Hyperparathyroidism
Connor Shortt, DO* and Laura Loertscher, MD*
Introduction: Primary hyperparathyroidism is the third most common endocrine disorder, following diabetes and thyroid disease. It is characterized by excess calcium and inappropriately elevated parathyroid (PTH) levels. Severe disease classically presents with a combination of nephrolithiasis, bone pain, osteoporosis, constipation, abdominal pain, anxiety, depression, or confusion. However, due to the availability of routine labs, most cases now present as asymptomatic hypercalcemia. Case Description: A 60-year-old female was evaluated for falls, generalized weakness, constipation, and brain fog. Her admission labs revealed a calcium of 19.6 mg/dL and subsequent PTH of 1,932 pg/mL. She was treated with intravenous fluids, pamidronate, and cinacalcet, and ultimately required hemodialysis for calcium normalization. A CT of the neck and chest showed a nodule at the right tracheoesophageal groove and another nodule adjacent to the left thyroid gland, both suggestive of parathyroid adenomas. However, two right lung masses, concerning for malignancy, were also identified. In the setting of extreme hypercalcemia, a CT-guided lung biopsy was performed due to suspicion for parathyroid carcinoma or ectopic PTH-secreting lung cancer. Lung pathology revealed benign hamartoma. Subsequent right parathyroidectomy was performed, and pathology was most consistent with a parathyroid adenoma. The PTH level normalized intraoperatively, and she was discharged to a skilled nursing facility. Discussion: Hypercalcemia has an expansive differential diagnosis, and the magnitude of elevation influences the pretest probability for a cancer-related etiology. Severe hypercalcemia, defined as >14 mg/dL, raises concern for malignancy. PTH remains a critical first step in refining the differential as most causes of cancer-related hypercalcemia demonstrate a suppressed PTH. Severe hypercalcemia and a PTH > 5 times the upper limit of normal can raise concern for parathyroid carcinoma; however, this diagnosis accounts for < 1% of primary hyperparathyroid cases. Ectopic PTH-producing tumors are rare and most commonly occur in the lung. Primary hyperparathyroidism is usually caused by a single benign parathyroid adenoma (80-85% of cases) and is less commonly due to multiglandular parathyroid hyperplasia. Despite an uncommon presentation, our patient was ultimately diagnosed and treated for parathyroid adenoma. The combination of severe symptoms, extreme elevation in calcium and PTH, and suspicious lung nodules raised appropriate concern for malignancy. While these cancers are rare, they must be considered to avoid unnecessary parathyroid surgery and incorrect treatment. Due to increased use of routine labs, most cases of primary hyperparathyroidism are asymptomatic at diagnosis, allowing the general internist to intervene long before hypercalcemic crisis. This case underscores the clinical adage ‘common things are common,’ while illustrating the value of deliberate and nuanced clinical reasoning in uncovering atypical presentations.
-

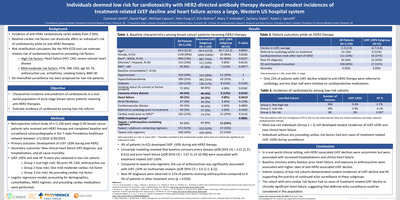
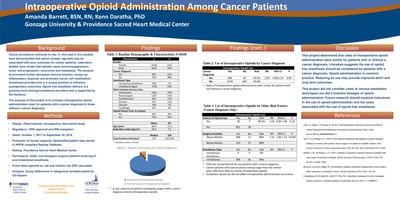
Individuals deemed low risk for cardiotoxicity with HER2-directed antibody therapy developed modest incidences of treatment-related LVEF decline and heart failure across a large Western US hospital system
Cameron Smith1, David Page1, Michael Layoun, and Li Hsin-Fang
Background: Incidence of anti-HER2 cardiotoxicity varies widely from 3-30%. Baseline cardiac risk factors can drastically affect an individual's risk of cardiotoxicity while on anti-HER2 therapies. Risk stratification calculators like the HFA-ICOS tool can estimate relative risk of cardiotoxicity based on preceding risk factors. High risk factors: Heart failure (HF), CAD, severe valvular heart disease. Mild-moderate risk factors: HTN, DM, CKD, age 65-79, anthracycline use, arrhythmia, smoking history, BMI>30. De-intensified surveillance has been proposed for low-risk patients. Objective: Characterize incidence and predictors of cardiotoxicity in a real world population of early-stage breast cancer patients receiving anti-HER2 therapies. Evaluate incidence of cardiotoxicity among low-risk cohorts. Methods: Retrospective cohort study of n=1,156 early stage (I-III) breast cancer patients who received anti-HER2 therapy and completed baseline and surveillance echocardiography in the 7-state Providence healthcare network between 1/1/2016-3/20/2024. Primary outcome: Development of LVEF < 50% during anti-HER2. Secondary outcomes: New clinical heart failure (HF) diagnosis, any hospitalization, and all-cause mortality. LVEF ≤50% and new HF % were also obtained in low-risk cohorts: Group 1 (not high risk): No prior HF, CAD, anthracycline use; Group 2 (low-risk): One mild-moderate cardiac risk factor; Group 3 (no-risk): No preceding cardiac risk factor. Logistic regression models accounting for demographics, comorbidities, HER2 regimen, and preceding cardiac medications were performed. Conclusions: In a real-world clinical setting, anti-HER2-associated LVEF declines were uncommon but were associated with increased hospitalizations and clinical heart failure. Baseline coronary artery disease, prior heart failure, and exposure to anthracyclines were associated with higher rates of anti-HER2- associated LVEF decline. Interim analysis of low-risk cohorts demonstrated modest incidences of LVEF decline and HF, supporting the practice of continued echo surveillance in these subgroups. The cohort with zero cardiac risk factors had no cases of treatment-related LVEF decline or clinically significant heart failure, suggesting that deferred echo surveillance could be considered in this population.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}