
Files
Download Full Text (395 KB)
Publication Date
4-29-2026
Keywords
oregon, psvmc, psvmc gme, psvmc gme pharmacy
Disciplines
Medical Education
Abstract
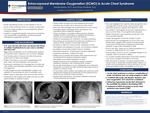
Introduction: Acute chest syndrome (ACS) is a severe complication of sickle cell disease. Rarely, it may progress to acute respiratory distress syndrome (ARDS). Inability to oxygenate despite mechanical ventilation necessitates consideration of extracorporeal membrane oxygenation (ECMO). Case Summary: A 31-year-old man with sickle cell disease presented with low back pain similar to prior pain crises. Vital signs were normal, and his hemoglobin level was 10.2 g/dL, with a reticulocyte index of 0.05. He was admitted for pain control and rehydration. That night, he developed fever, tachypnea, and hypoxemia with imaging showing a right lower lobe infiltrate, consistent with ACS. He was treated with broad-spectrum antibiotics and escalated to high flow nasal cannula. Hematology recommended transfer to a center capable of exchange transfusion, and he was admitted to the intensive care unit in the interim. Repeat hemoglobin level decreased to 8.0 g/dL and a stat transfusion was ordered. Despite noninvasive ventilation, he remained hypoxemic and endotracheal intubation was performed; however, he remained hypoxemic and suffered a cardiac arrest with successful resuscitation within three minutes, though he developed shock. His hemoglobin level rapidly dropped to 4.3 g/dL. He received multiple transfusions and vasopressor support and remained persistently hypoxemic and with worsening lactic acidosis. He was found to have severe right heart failure on echocardiography and underwent placement of a Protek Duo right ventricular assist device before transferring to a tertiary center. Continuous renal replacement therapy was started and despite transition to veno-arterial-venous ECMO for new onset left ventricular failure, he suffered a ventricular tachycardia arrest and expired. Discussion: This case highlights the need for early recognition and management of both acute vaso-occlusive crisis requiring transfusion support and refractory ARDS potentially needing ECMO. Our patient’s hemoglobin level was not re-checked until he arrived in the ICU, by which time it dropped significantly. Earlier supportive transfusion may have provided benefit, targeting a goal hemoglobin level of at least 10g/dL. Employment of ECMO for management of ACS is rare, and limited data suggests cohorts including adults have a lower survival rate compared to exclusively pediatric cases (27% vs. 52%). Due to this rarity, there are no official guidelines on if or when to use ECMO in ACS. With advances in this therapy, including awake ECMO, we advocate for further study to determine whether earlier initiation of ECMO may be beneficial in saving the lives of young, otherwise healthy sickle cell patients such as ours.
Specialty/Research Institute
Graduate Medical Education
Specialty/Research Institute
Pharmacy



