
Files
Download Full Text (346 KB)
Publication Date
4-29-2026
Keywords
oregon, psvmc, psvmc gme, psvmc oaa
Disciplines
Cardiology | Medical Education
Abstract
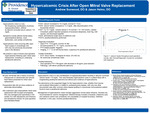
59. Hypercalcemic Crisis After Open Mitral Valve Replacement Andrew Sunwood, DO Background: Hypercalcemic crisis is a rare manifestation of primary hyperparathyroidism characterized by a sudden increase in serum calcium levels to >14 mg/dL with symptoms of hypercalcemia including adverse gastrointestinal symptoms, abdominal pain, and even predisposition to cardiac arrhythmias. There is only one other documented case of hypercalcemic crisis occurring after open heart surgery. Case information: 69-year-old female with a history of primary osteoporosis on alendronate and valvular heart failure presented for mitral valve replacement. Preoperative lab work did not show evidence of electrolyte abnormalities. She under- went open bioprosthetic mitral valve replacement with tricuspid valve annuloplasty. She was taken to the cardiac intensive care unit for routine post-operative management and placed on dobutamine and furosemide infusions. Amiodarone was also started for post-operative atrial fibrillation/flutter. Post-operative day 3 (POD3), calcium levels were noted to rise to 10.5 mg/dL (normal 8.7-10.2 mg/dL). POD4, furosemide infusion was discontinued and calcium levels continued to rise to 11.2 mg/dL. The patient reported symptoms including increased sleepiness, brain fog, mild nausea, and decreased appetite. Further workup showed elevated intact parathyroid hormone 1310 pg/mL (normal 18-88 pg/mL), 25-hydroxyvitamin D 15.1 ng/mL (normal 20-50 ng/mL), and a negative parathyroid hormone-related peptide. Electrocardiogram showed sinus rhythm with a 1st degree AV block and QTc of 453 ms. A thyroid ultrasound demonstrated a 3 x 1.5 cm lesion on the left thyroid lobe, suspected parathyroid adenoma. Management included cinacalcet, normal saline infusion with IV furosemide for volume management, and zoledronic acid. Calcitonin was considered but was not on the hospital formulary. Serum calcium levels peaked on POD7 at 15.7 mg/dL with an ionized calcium of 2.15 mmol/L (normal 1.12-1.40 mmol/L). There was no evidence of arrhythmia apart from atrial fibrillation. She underwent parathyroidectomy revealing a left inferior parathyroid adenoma with immediate intraoperative normalization of parathyroid hormone levels post-resection. Serum calcium levels remained within normal limits for the remainder of her hospitalization, and she was discharged with vitamin D and calcium citrate. Discussion: Hypercalcemic crisis is a rare manifestation of hyperparathyroidism resulting in albumin-corrected calcium levels >14 mg/dL. This case illustrates hypercalcemic crisis in a patient likely with a longstanding parathyroid adenoma but without prior evidence of hypercalcemia. The sternotomy is the suspected trigger for the hypercalcemic crisis, whether from trauma and localized inflammation or related to cardiopulmonary bypass, with only one other documented case after coronary artery bypass grafting in a previously normocalcemic patient found to have a parathyroid adenoma. Management of hypercalcemic crisis includes stabilization through normal saline infusions and reduction of serum calcium levels with +cinacalcet, bisphosphonates, and calcitonin, if possible; and definitive treatment with parathyroidectomy. Post-valvular surgery patients especially require close moni- toring for signs of cardiac arrhythmias given the heightened risk post-operation.
Specialty/Research Institute
Graduate Medical Education
Specialty/Research Institute
Internal Medicine
Specialty/Research Institute
Cardiology



