
Files
Download Full Text (2.4 MB)
Publication Date
4-29-2026
Keywords
oregon, psvmc, psvmc gme, psvmc oaa
Disciplines
Infectious Disease | Medical Education
Abstract
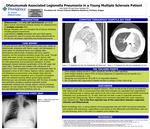
Ofatumumab is the only anti-CD20 IgG1κ human monoclonal antibody therapy for relapsing forms of multiple sclerosis (MS) that patients can self-administer subcutaneously. Anti-CD20 agents are biologic therapies that carry an increased risk of serious infections, but rarely Legionellosis. We present the case of a young man taking ofatumumab for his MS who developed Legionella pneumoniae pneumonia. A 30-year-old man with MS diagnosed two years prior, stable on ofatumumab, presented with fevers, cough, and hemoptysis. A week earlier, he developed fevers and myalgias after administering ofatumumab, but these symptoms persisted longer than usual. Though initial vital signs were normal, he appeared ill and clammy and had bilateral rhonchi on pulmonary auscultation. There was leukocytosis and an elevated procalcitonin level. A chest radiograph showed extensive opacification of the left upper and lower lobes. Treatment with ceftriaxone and azithromycin was initiated. Overnight, he developed a high fever to 40.3 Celsius and treatment was broadened to piperacillin-tazobactam. Sputum culture and urine antigen tests for Legionella and Streptococcus pneumonia were negative. Days later he became hypoxemic, and a computed tomography scan was obtained showing diffuse ground glass opacities. Bronchoscopy was ultimately performed, ultimately revealing a positive Legionella nuclear amplification antibody test, though sputum cultures remained negative. He was treated with levofloxacin for a five-day course with improvement and discharged breathing room air. Our patient’s young age belied his atypical infection, which he was at risk of due to his ofatumumab. While some biologics are associated with Legionellosis such as alemtuzumab, this is less common among anti-CD20 therapies like rituximab. While ofatumumab has been associated with upper respiratory tract infections, this is the first report of an association with Legionella. The final diagnosis in our case was delayed because the Legionella urine antigen testing was negative. Urine antigen testing is commonly used to rule out Legionella as a cause of atypical pneumonia; Urine antigen testing is used in 97% of clinical diagnoses. However, this test is not definitive, despite 69 to 100% sensitivity and 99 to 100% specificity, because it is specific for L. pneumophila serogroup 1 only. Serogroup 1 accounts for 50 to 80 % of Legionella infections and 8% of patients with Legionnaire’s disease excrete no antigen in their urine. This first report demonstrates that in patients immunosuppressed with anti-CD20 therapies presenting with pneumonia, Legionellosis must be considered until definitively ruled out by bronchoscopy, even when urine antigen testing is negative.
Specialty/Research Institute
Graduate Medical Education
Specialty/Research Institute
Internal Medicine
Specialty/Research Institute
Infectious Diseases



