
The PGY1 Pharmacy Residency program has been accredited by ASHP since 1994, offering residents the opportunity to participate in collaborative, integrated care in health system pharmacy practice. Residents apply advanced practice-based skills, expand leadership skills, participate in professional organizations, and participate in innovative approaches to delivery of care.
The PGY1 Pharmacy Residency is one program with two sites: Providence Portland Medical Center and Providence St. Vincent Medical Center. Both Providence Portland Medical Center and Providence St. Vincent Medical Center have implemented a layered learning model, with pharmacy student/resident/attending pharmacist teams on each of the core clinical services, modeled after the medical education model. The teams work collaboratively with health care practitioners to provide patient care and improve medication management across transitions in care. The PGY1 Pharmacy Residency program provides broad experience and confidence in practice-based skills across diverse practice settings while offering the opportunity to obtain focused experience in areas of interest.
-

Clinical Impact of an HIV Specialist Pharmacist Collaborative Practice Agreement: a 1-year Retrospective Review of Interventions
Rebekah Bartholomew, Geoffrey L'Heureux, and Brent Footer
Title: Clinical Impact of an HIV Specialist Pharmacist Collaborative Practice Agreement: a 1-year Retrospective Review of Interventions
Purpose/Background:
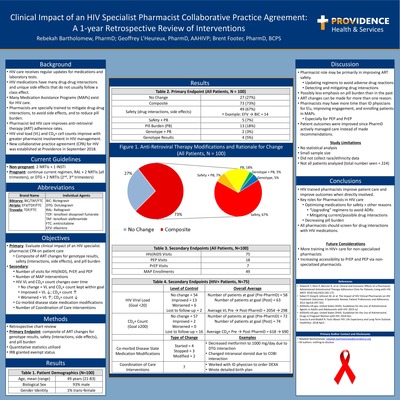
HIV continues to be one of the most complex disease states for patients and providers to manage. With new medications and guidelines being routinely updated, ensuring that patients are on optimal anti-retroviral therapy (ART) throughout their lives can be difficult. Previous studies on pharmacist-led HIV services have shown that utilizing a pharmacist to manage ART is beneficial. The purpose of this study is to add to that body of evidence by analyzing the clinical impact of a nascent collaborative practice agreement for an HIV specialist pharmacist to manage patients seeking care related to HIV.
Methods:
This study was granted exempt status by the Providence Institutional Review Board. An electronic health record was utilized to identify patients whom were seen at an HIV clinic under the management of a pharmacist. Chart reviews were conducted to collect and analyze pharmacist interventions. Data collected included the following: number of ART changes (and rationale for each change to be categorized as for efficacy, safety, or simplification reasons), number of patients seen for HIV/AIDS, PrEP, and PEP, number of patients enrolled in medication assistance programs (MAPs), HIV viral loads (VLs) and CD4+ cell counts over 1 year (each patients’ level of control to be classified as improved, worsened, or no change), number of co-morbid disease state medication modifications, and number of coordination of care interventions. The data was recorded without patient identifiers to maintain confidentiality. Data analysis consisted of quantitative analyses.
Results:
A total of 100 patient charts were reviewed. Of those 100, 73 patients had their ART regimens modified. Of those 73 ART regimen changes, 54 were for safety related reasons (such as to avoid drug-drug interactions or to mitigate adverse drug reactions), 20 were for simplification reasons (such as to decrease pill burden), and 6 were related to improving efficacy due to genotype resistance testing. Some patients had their ART regimens changed for more than one reason. Of the 100 patients, 75 patients were living with HIV, 18 were on PEP, and 7 were on PrEP. Nearly half (49) were enrolled in MAPs with pharmacist assistance. Most patients’ HIV VLs and CD4+ cell counts improved or stayed the same (89% VL and 79% CD4+). Few changes were made to co-morbid disease state medications (9 total modifications). Only 7 patients required coordination of care interventions.
Conclusions:
Because HIV medicine is so complex, there can possibly be a mentality of “don’t change what is working” when it comes to which ART regimen patients are on. Leaving patients on the same regimen for years and decades may lead to medication related problems. Pharmacists are uniquely trained to help mitigate medication related issues. This study appears to show that pharmacists are most valuable in HIV medicine in mitigating safety concerns (drug interactions and adverse drug events). Pharmacists may also be especially useful in enrolling patients in MAPs.
-
 Song, Pamela Levine, Katharine F. Marshall, and Chelsea Harmon")
Development and implementation of take-home naloxone kit for patients admitted to the emergency department of a large tertiary care hospital
Myung Seon (Amy) Song, Pamela Levine, Katharine F. Marshall, and Chelsea Harmon
Title: Development and implementation of take-home naloxone kit for patients admitted to the emergency department of a large tertiary care hospital
Authors: Myung Seon (Amy) Song, PharmD; Pamela Levine, PharmD, BCPS; Katharine F. Marshall, MD; Chelsea Harmon, PharmD Candidate 2020
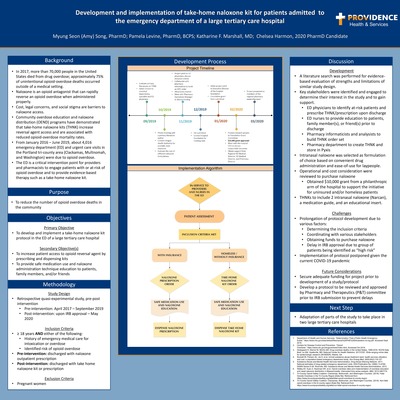
Background/Purpose: In 2017, the United States Department of Health and Human Services (HHS) declared the opioid epidemic as a public health emergency as more than 70,000 people died from drug overdoses. Approximately 75% percent of unintentional opioid-overdose deaths occurred outside of a medical setting. In order to combat the opioid crisis, the US Surgeon General urged prescribers and pharmacists to increase access to naloxone for individuals who are at risk for opioid overdose. Community overdose education and naloxone distribution (OEND) programs have demonstrated that take-home naloxone kits are associated with reduced opioid-overdose death rates and are cost-effective. From January 2016 – June 2019, about 4,016 emergency department (ED) and urgent care visits in the Portland metropolitan area were identified to be due to opioid overdose. Recent data from the Centers for Disease Control and Prevention (CDC) indicates a continuing upward trend, making the ED a critical intervention point for providers and pharmacists to engage patients with at-risk of opioid overdose and provide evidence-based interventions such as take-home naloxone kit. The primary objective of this study is to develop and implement a pharmacist driven take-home naloxone kit protocol. The secondary objective is to increase access to naloxone by prescribing and dispensing kits to at-risk patients in the emergency department.
Methods: A retrospective quasi-experimental, pre- and post-protocol analysis, will be used to compare the number of prescriptions written prior to implementation of protocol (April 1, 2017 to September 1, 2019) to the number of take-home naloxone kit dispensed post implementation of the protocol. Inclusion criteria include patients 18 years or older and admitted to ED for treatment of opioid overdose, or with risk factors of opioid overdose. The primary endpoint is number of naloxone prescription written and take-home naloxone kits dispensed.
Results: Key stakeholders were identified and engaged in developing the protocol. Operational and cost consideration were reviewed. Various factors affected development and implementation of the study.
Conclusions: Adaptation of parts of the study to take place in two large tertiary care hospitals.
IRB status: Pending
-
 pilot project by Ling J. Zhan, Sharon Leigh, Mary E. Kuebrich, Clara Mikhaeil, Kevin Hom, and Colleen M. Casey")
Evaluating outcomes of medication-related interventions from the “Seniors At risk for Falls after Emergency Room visit” (SAFER) pilot project
Ling J. Zhan, Sharon Leigh, Mary E. Kuebrich, Clara Mikhaeil, Kevin Hom, and Colleen M. Casey
Primary Author: Ling J. Zhan, PharmD
Co-Authors: Sharon Leigh, PharmD BCPS, Mary Beth Kuebrich, MS, AGPCNP-BC, Clara Mikhaeil, PharmD, BCPS, Colleen M. Casey, PhD, ANP-BC
Location: Providence Health & Services, Portland, Oregon
Title: Evaluating outcomes of medication-related interventions from the “Seniors At risk for Falls after Emergency Room visit” (SAFER) pilot project
Purpose: Falls are the leading cause of injury in older adults, resulting in decreased mobility, loss of independence, and increased health care costs. Even a single fall puts an older adult at higher risk for future falls. Despite numerous studies showing evidence that multifactorial fall risk interventions are effective in decreasing fall risk, even older adults who have an injurious fall often do not receive meaningful interventions to mitigate their fall risk. This study evaluated the impact of medication-related interventions for older adults who had a fall-related ED visit, as part of a larger study of multifactorial fall-risk interventions in the primary care setting.
Methods: This study was approved by the Providence-Oregon Institutional Review Board. This retrospective chart review studied a subset of patients enrolled in the SAFER pilot project who presented to an ED following a fall. Included patients were 75 years or older and taking at least one high-risk medication (HRM) that is associated with increased risk for falls. Patients were enrolled in the SAFER pilot from December 2018 to June 2019. Eligible patients received a comprehensive medication review by a clinical pharmacist; some also received a Geriatric consult that included medication recommendations. Medication recommendations were then forwarded to the clinic’s Primary Care Provider (PCP) and Registered Nurse for follow up. The parent study used a matched control design to compare SAFER interventions with usual care; this study did not include a comparison to the control group. Study outcomes included: overall burden of high-risk medications, number of high-risk medications discontinued or tapered, initiation of osteoporosis treatment or prevention measures, changes in blood pressure (BP) or hemoglobin A1c goals, and overall reduction in polypharmacy. The study also evaluated to what degree medication-related recommendations were adopted by the PCP over a minimum follow-up period of 7 months.
Results: Overall, 50 patients underwent chart review with 4 patients not meeting inclusion criteria; 46 patients were on HRM (average 4.3 HRM/person) and included in the final analysis.
Of those patients, 25 (54%) received a PharmD consult. For these 25 patients, 117 medication-related recommendations were made by the Geriatric and Clinical Pharmacy teams. Of those, a total of 52 (44%) changes were implemented by the PCP: 17 HRMs were discontinued, 9 taper/cross-tapered, and 17 osteoporosis-related initiated. BP and A1c goals on patient’s problem list were not clearly defined for 69% and 50% of patients, respectively.
Conclusion: Medication optimization and reduction of HRM was effective in patients receiving a PharmD consult. The most accepted recommendations included ordering DEXA, orthostatic BP testing, adding Vitamin D, and discontinuing opioids. Not every patient who qualified received a PharmD consult, suggesting that more medication changes could have been implemented had PharmDs been involved. The process of referring to a PharmD for a consult will need to be reviewed. Given that these patients are at high risk to fall, BP and A1c goals should be clarified and perhaps more lenient goals may be indicated. In addition, these results should be compared with the matched-control group of the parent study to determine the value of reducing HRM use in older patients at high risk of falls.
-

Evaluating the utility of CYP2C19 genetic testing for P2Y12 inhibitor prescribing within an inpatient setting
Thomas E. Maslo and Carolynn Null
Thomas Maslo, PharmD, PGY-1 Pharmacy Resident
Carolynn Null, PharmD
Providence Portland Medical Center, Portland, Oregon
Evaluating the utility of CYP2C19 genetic testing for P2Y12 inhibitor prescribing within an inpatient setting
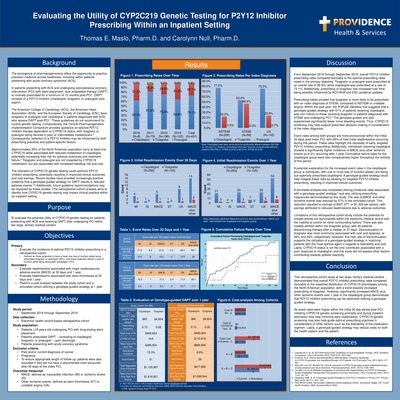
The emergence of pharmacogenomics offers the opportunity to practice precision medicine across health care. In patients presenting with acute coronary syndrome (ACS) and undergoing percutaneous coronary intervention (PCI), dual antiplatelet therapy (DAPT) is routinely prescribed for 12 months. DAPT consists of a P2Y12 inhibitor (clopidogrel, ticagrelor, or prasugrel) plus aspirin. Of the P2Y12 inhibitors, clopidogrel is uniquely impacted by CYP2C19 status. About 30% of the North American population carry at least one CYP2C19 allele associated with reduced metabolism. Ticagrelor and prasugrel are not impacted by CYP2C19 metabolism, but are associated with increased bleeding and cost. Current guidelines favor the use of the latter, with routine genetic testing not recommended. Recent studies have provided positive evidence that a genotype-guided approach results in improved outcomes. This study aims to identify how CYP2C19 genetic testing may impact prescribing practices. This is an IRB-approved, retrospective cohort analysis of P2Y12 inhibitor prescribing and outcomes following PCI. Chart review within the electronic health record was completed from September 2016 to September 2019 among patients presenting to two large, tertiary medical centers. Patients included those >18 years old, with an index diagnosis of ACS. Patients were excluded if they had a history of cancer, pregnancy, or if they did not have a documented encounter after 30 days following PCI. The primary outcome was the incidence of optimal P2Y12 inhibitor prescribing. Secondary outcomes included major adverse cardiovascular events (MACE) and stent thrombosis at 30 days and 1 year. A cost analysis was also completed utilizing a simulated genotype-guided strategy. A total of 401 patients were included within the primary analysis, with clopidogrel and ticagrelor being prescribed at rates of 73.1% and 26.1%, respectively. Prasugrel was prescribed at a rate of 0.8%. There was no difference among prescribing for an index diagnosis of NSTEMI vs. unstable angina (p=0.71). However, prescribing was different for NSTEMI vs. STEMI (p=0.00) and unstable angina vs. STEMI (p=0.00). Patients prescribed clopidogrel were readmitted for MACE or other ischemic events significantly more than those prescribed ticagrelor (p=0.01). Additionally, event rates were increased within the initial 30 days. In a cost-analysis with a simulated genotype-guided strategy, reduced readmission rates resulted in total cost-savings of $527,377, or $1,325 per person. This study shows that overall P2Y12 inhibitor prescribing rates compare favorably to the expected population distribution of CYP2C19 alleles. However, individuals with loss of function alleles are potentially being prescribed clopidogrel at discharge, thus increasing their risk for adverse outcomes. As these event rates are more pronounced within the initial 30 days, initiating CYP2C19 screening in the inpatient setting may help minimize early readmissions. Additionally, a genotype-guided approach may result in cost-savings over 1 year.
-

Evaluation of a two-way, HIPAA-compliant text-messaging platform in a health system specialty pharmacy
DJ Clark, Adam Saulles, and Tara Berkson
PDJ Clark, PharmD, PGY1 Pharmacy Practice Resident
Adam Saulles, PharmD, CSP, BCACP; Tara Berkson, PharmD, BCACPProvidence Health and Services, Portland, Oregon
Evaluation of a two-way, HIPAA-compliant text-messaging platform in a health system specialty pharmacy
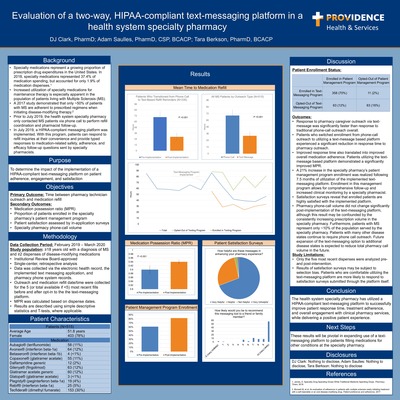
Specialty medications, including those used to treat Multiple Sclerosis (MS), represent a growing proportion of prescription drug expenditures in the United States. MS is a chronic, progressive condition that requires maintenance therapy with disease-modifying medications. Many patients with MS rely on specialty pharmacies to obtain, dispense, and perform the necessary monitoring for these complex medication regimens. A study performed in 2017 by Munsell et al, demonstrated that only ~50% of patients with MS are adherent to prescribed regimens when initiating disease-modifying therapy. Routine pharmacy outreach could potentially help improve medication adherence in a population at high risk of disease progression secondary to non-adherence. Prior to July 2019, this health system specialty pharmacy only contacted MS patients via phone call to perform refill coordination and pharmacist follow-up. This strategy has been effective, but is not without flaws. Oftentimes, patients prefer not to receive phone calls or are unavailable during pharmacy business hours. This can lead to repeat outreach phone calls from caregivers and gaps in therapy. In July 2019, a HIPAA-compliant messaging platform was implemented. With this program, patients can respond to refill inquiries at their convenience and provide typed responses to medication-related safety, adherence, and efficacy follow-up questions sent by specialty pharmacists. This project seeks to identify whether implementation of the aforementioned messaging platform has had a quantifiable benefit on patient outreach and workflow outcomes within a health system specialty pharmacy setting. This single center, retrospective cohort analysis evaluated adult patients with a diagnosis of MS and at least 2 dispenses of disease-modifying medications. Data was collected via the electronic health record and the implemented text messaging application. The primary outcome is time between pharmacy technician outreach and medication refill. Secondary outcomes include medication adherence reported as medication possession ratio (MPR), the proportion of patients enrolled in the specialty pharmacy’s patient management program, patient satisfaction, and pharmacy phone call volume. Between group differences were described using simple descriptive statistics and T-tests, where applicable. A total of 335 patient had fills prior to and post-implementation of the text messaging platform, and 313 had multiple fills in each category, allowing for calculation of MPR. Response time (HH:MM ± 95% Confidence interval) was significantly decreased with utilization of text-message refill reminders (32:03 ± 7:09 vs 68:34 ± 11:37; p
-

Evaluation of Guideline-Directed Medication Therapy for Heart Failure with Reduced Ejection Fraction Patients at Discharge on 30-Day Readmission Rates at Two Tertiary Healthcare Centers
Jacqueline Hesse, Yan Xu, Meri Slavica, James E. Watkins, Alan Rankin, and Joshua Remick
Evaluation of Guideline-Directed Medication Therapy for Heart Failure with Reduced Ejection Fraction Patients at Discharge on 30-Day Readmission Rates at Two Tertiary Healthcare Centers
Principal Investigator: Jacqueline Hesse, Pharm.D.
Preceptors: Yan Xu, Pharm.D., BCPS, BCCP; Meri Slavica, Ph.D., BCPS
Pharmacy Student: James Watkins, 2020 Pharm.D. Candidate
Sub-Investigators: Alan Rankin, MD; Joshua Remick, MD
Background:
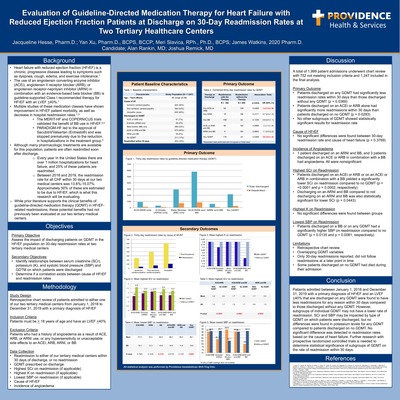
Heart failure with reduced ejection fraction (HFrEF) is a chronic, progressive disease leading to symptoms such as dyspnea, cough, edema, fatigue, and exercise intolerance. The use of anangiotensin converting enzyme inhibitor (ACEi), angiotensin II receptor blocker (ARB), or angiotensin receptor-neprilysin inhibitor (ARNI) in combination with an evidence-based beta blocker (BB) is guideline-supported Class I recommended therapy for HFrEF with an LVEF
Methods:
A retrospective chart review was completed using the Epic Electronic Medical Record of all patients admitted to one of our tertiary medical centers between January 1, 2018 and December 31, 2019 with a primary diagnosis of HFrEF. Patients were included if they were at least 18 years of age and had an LVEF of
Results
A total of 1,999 patient admissions underwent chart review with 752 admissions not meeting inclusion criteria and 1,247 admissions being included in the final analysis. Of those included, 202 patients (16%) were readmitted within 30 days. Patients discharged with any GDMT had less readmissions within 30 days than those without any GDMT (OR 0.6, 95% CI 0.4-1.0, p = 0.0369). However, patients discharged on an ACEi or ARB had more readmissions within 30 days than patients discharged on no GDMT (OR 1.4, 95% CI 1.0-1.9, p = 0.0283). 49% of patients (N = 609) had an idiopathic cause of heart failure followed by 32% of patients with non-ischemic cardiomyopathy (N = 394) and 20% of patients with ischemic cardiomyopathy (N = 244). No significant differences were found between the 30-day readmission rate and cause of heart failure. For highest K value on readmission, no significant differences were found between groups. For highest SCr on readmission, discharging on an ACEi or ARB or discharging on an ACEi or ARB in combination with a BB yielded a significantly lower SCr on readmission compared to no GDMT (1.6 vs. 2.6, p =
Conclusion
In conclusion, patients admitted with a primary diagnosis of HFrEF that are discharged on any GDMT were found to have less readmissions for any reason within 30 days than those without any GDMT. However, subgroup analysis for individual GDMT may not have a lower rate of readmissions. Further research with prospective randomized controlled trials is needed to determine statistical significance of subgroups of GDMT on the rate of readmission within 30 days.
-

Evaluation of late-onset sepsis antibiotic utilization and revision of empiric late-onset sepsis antibiotic prescribing guidelines
Alex Creevan, Sara Clark, Anavice Jimenez, and Michael Garcia
Alex Creevan, PharmD
Michael Garcia, PharmD, Angela Roberti, PharmD, Sara Clark, PharmD, Anavice Jimenez, PharmD Candidate
Providence St. Joseph Health, Portland, OR
Evaluation of late-onset sepsis antibiotic utilization and revision of empiric late-onset sepsis antibiotic prescribing guidelines
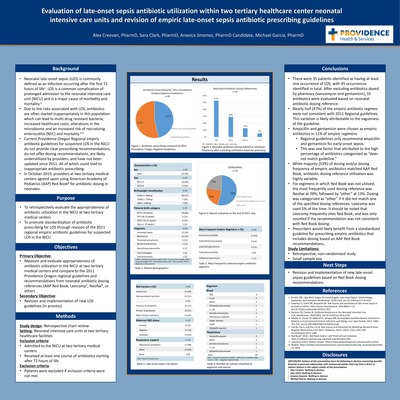
Neonatal late-onset sepsis (LOS) is commonly defined as an infection occurring after the first 72 hours of life. Late onset sepsis is a common complication of prolonged admission to the neonatal intensive care unit (NICU) and is a major cause of morbidity and mortality. Due to risks associated with LOS, empiric antibiotics can be inappropriately prescribed, which may lead to multi-drug resistant bacteria, increased healthcare costs, alterations in microbiome, increased risk of necrotizing enterocolitis (NEC) and mortality. Current Providence Oregon regional guidelines for suspected LOS in the NICU do not provide clear prescribing or antibiotic dosing recommendations, have not been updated since 2011, and are underutilized by providers. All of which can lead to inappropriate antibiotic prescribing. Providers at two tertiary medical centers agreed upon using American Academy of Pediatrics (AAP) Red Book for antibiotic dosing in October 2019. A retrospective chart review was conducted to evaluate the appropriateness of antibiotic utilization in the NICU at two tertiary medical centers, and to promote standardization of antibiotic prescribing for LOS through revision of the 2011 regional empiric antibiotic guidelines for suspected LOS in the NICU. This study was approved by the institutional review board. Patients admitted to the NICU between September 1, 2016 through August 31, 2019 with confirmed or suspected LOS who received at least one dose of empiric antibiotics starting after 72 hours of life were included in the study. The primary outcome is to measure the appropriateness of antibiotic utilization compared to the 2011 Providence Oregon Regional guidelines and recommendations from the neonatal antibiotic dosing references AAP Red Book, Lexicomp, Neofax, or “other” if dosing did not match one of the specified reference. The secondary outcome measure of revision and implementation of new late-onset sepsis guidelines is still in progress. Exploratory outcomes include antibiotic selection, indication, and duration of therapy. Patient data such as risk factors for LOS, diagnosis, gestational age, postnatal age and postmenstrual age at time of antibiotic initiation, birth weight, blood culture and susceptibilities, and outcomes such as mortality, transfer to a higher level of care, discharge home, and further courses of antibiotics were also included as exploratory outcomes. Thirty-five patients were identified as having at least one instance of LOS, and there were 45 instances of LOS total, as some patients had more than one occurrence. After excluding antibiotics dosed by pharmacy (vancomycin and gentamicin), 55 antibiotics were evaluated based on neonatal antibiotic dosing reference. For the primary outcome, 47% (21) empiric antibiotic regimens did not correspond with the 2011 guideline. Fifty-three percent (29) of antibiotic dosing matched AAP Red Book recommendations, 29% (16) matched Neofax, 5% (3) matched Lexicomp, and 13% (7) other. Nearly half of the empiric antibiotic regimes were not consistent with 2011 Regional guidelines. These inconsistencies are likely attributable to the vagueness of the guideline. In addition, while the majority of dosing matched AAP Red Book, antibiotic dosing reference utilization was highly variable. Prescribers would likely benefit from a standardized guideline for prescribing empiric antibiotics based on AAP Red Book dosing recommendations.
-

Evaluation of surgical antibiotic prophylaxis at a large, tertiary medical center
Emily Fox, Brent Footer, and Angel Mendez
Emily Fox, PharmD, PGY-1 Pharmacy Resident
Brent Footer, PharmD, BCPS; Angel Mendez, Pharmacy Student
Providence Portland Medical Center, Portland, Oregon
Evaluation of surgical antibiotic prophylaxis at a large, tertiary medical center
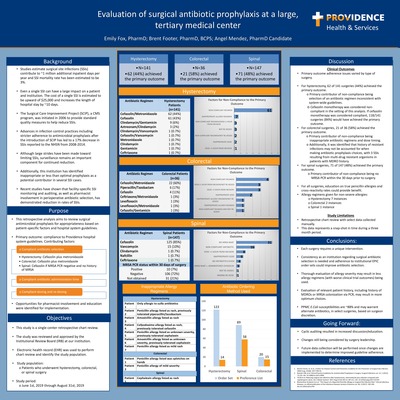
Surgical site infections (SSI) are a significant cause of morbidity, prolonged hospitalization, and mortality. The cost of a single SSI is estimated to be upward of $25,000 and increases a patient’s length of hospital stay by ~10 days. Our institution has identified inappropriate or less than optimal antimicrobial prophylaxis as a potential contributor in several recent SSI cases. Current literature on this topic has found that there may be a role for clinical pharmacists in cyclic auditing to improve surgical antibiotic prophylaxis guideline adherence. This retrospective analysis of hysterectomy, colorectal, and spinal surgeries aims to review surgical antimicrobial prophylaxis for appropriateness based on patient-specific factors and published system and national guidelines.
This is an IRB-approved, single institution retrospective chart review of surgical antibiotic prophylaxis regimens for adult patients that underwent hysterectomy, colorectal, or spinal surgery between the months of June and August 2019. Specific surgery types were chosen based on requests by surgery leadership and highest potential for quality improvement. Patients were identified by surgery classification via the electronic medical record (EMR). Other relevant data was obtained via the EMR including: surgeon, anesthesiologist, antibiotic regimen, dose, administration time, ordering method, and patient weight. Additional chart review was required for other relevant factors including history of multi-drug resistant organisms and allergy history/severity. The primary outcome measured was compliance to hospital system guidelines, accounting for antibiotic selection, administration timing, and dosing.
Primary outcome adherence rates varied greatly depending on the type of surgery. For hysterectomy, 62 of 141 surgeries (44%) achieved the primary outcome, with the primary contributor of non-compliance being selection of an antibiotic regimen inconsistent with system-wide guidelines. For colorectal surgeries, 21 of 35 (60%) achieved the primary outcome, with the primary reason for non-compliance being inappropriate antibiotic administration timing. Additionally, it was identified that history of resistant infections was not properly accounted for when making antibiotic prophylaxis choices, with 3 SSIs resulting from multi-drug resistant organisms in patients with MDRO history. Spinal surgery compliance to the primary outcome was less-clear, as guidelines are not as well-defined. However, MRSA colonization status was not determined via PCR when appropriate for 31 of 148 (21%) of surgeries.
Opportunities for pharmacist intervention and education were identified for implementation after chart review of each surgery. Each surgery requires a unique intervention. Primary outcome data and proposed interventions for each surgery was presented to the institutional surgical site infection committee, which met quarterly. Pharmacist cyclic auditing of antibiotic prophylaxis choices resulted in increased discussion and education. Proposed changes are still being considered by surgery department leadership, including a change in antibiotic choice for colorectal surgeries. Future data collection will be performed after changes are implemented to determine improved guideline adherence.
-
 by Adam Olesen and Kristen Wendell")
Impact of clinical pharmacist medication review upon enrollment in a Program for All-inclusive Care of the Elderly (PACE)
Adam Olesen and Kristen Wendell
Impact of clinical pharmacist medication review upon enrollment in a Program of All-Inclusive Care for the Elderly (PACE)
Adam Olesen, PharmD, PGY1 Resident
Kristen Wendell, PharmD, BCGPProvidence Elderplace Oregon
Learning Objective:
Describe the interventions and recommendations made by a pharmacist upon enrollment of a new participant at a PACE facility.
Abstract:
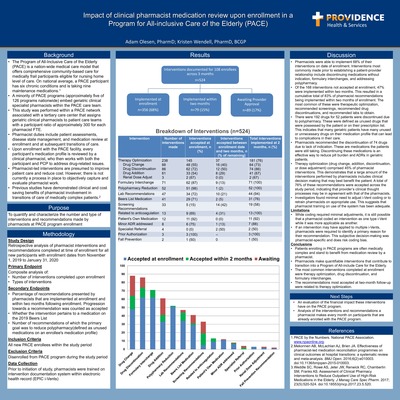
Pharmacists have been proven to be beneficial in the transitions of care for high-risk patients with multiple morbidities, such as the reduction of both polypharmacy and thirty-day readmission rates. The objective of this study is to quantify and characterize the total number and type of interventions and recommendations made by pharmacists over a three-month span when new participants enrolls with Providence ElderPlace, a Program of All-Inclusive Care for the Elderly (PACE). Clinical pharmacists at Providence Elderplace were trained on how to document their interventions and recommendations within the EPIC electronic medical record using the I-vent documentation system. The pharmacists documented interventions made at the time of enrollment and recommendations for follow-up after enrollment for all participants who were enrolled between Nov 1, 2019 and Jan 31, 2020. The primary investigator gathered this data via the I-vent reporting system within EPIC. Pharmacists also documented whether each recommendation pertained to a Beers List medication and whether the recommendation is made with the primary goal of reducing polypharmacy. The primary investigator followed recommendations that were not implemented at enrollment for two months to assess whether they were implemented by the provider. Data was analyzed to quantify the impact of these recommendations and interventions that the clinical pharmacists had made. The primary endpoint was a composite analysis of the number and type of interventions completed upon enrollment. Secondary endpoints included the percentage of recommendations presented by pharmacists that are implemented at enrollment and within two months following enrollment, whether the intervention pertains to a medication on the 2019 Beers List, and the number of recommendations of which the primary goal was to reduce polypharmacy (defined as unused medications on an enrollee's medication profile). Results will be presented. This study approved by the Institutional Review Board.
-

Impact of real-time antimicrobial stewardship team intervention versus conventional microbiology reporting on time to appropriate antimicrobial therapy in patients with Enterobacterales bacteremia
Scott C. King, Alyssa B Christensen, Brent Footer, Timothy G. Shan, Kim Health, Ivor Thomas, and Margaret Oethinger
Scott C. King
Alyssa B. Christensen, Brent W. Footer, Timothy G. Shan, Kim Health, Ivor Thomas, and Margret Oethinger
Impact of real-time antimicrobial stewardship team intervention versus conventional microbiology reporting on time to appropriate antimicrobial therapy in patients with Enterobacterales bacteremia.
Introduction:
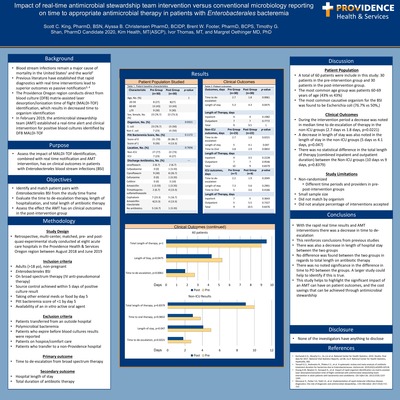
The benefit of rapid laboratory speciation combined with real time antimicrobial stewardship team (AMT) interventions has been shown to improve patient outcomes and decrease hospital costs. The Providence Oregon region conducts direct from blood culture matrix-assisted laser desorption/ionization time of flight (MALDI-TOF) identification, which results in decreased time to organism identification. The MALDI-TOF identification has allowed the AMT to intervene earlier than a health system using standard MALDI identification or comparable methods. The purpose of this study is to assess the impact of real time notification plus AMT intervention on clinical outcomes in patients with Enterobacterales blood stream infections (BSI).
Methods:
This was an IRB approved, retrospective, multi-center, pre- and post- quasi-experimental study conducted at eight acute care hospitals in the Providence Health & Services Oregon region. Adult patients (>18 years old) with a diagnosed BSI caused by an Enterobacterales species were included. The control group was from August 2018 to January 2019 and the intervention group was from February 2019 to June 2019. Patients were matched based on age, gender, and admission to the ICU. Exclusion criteria included polymicrobial infection, Pitt bacteremia score >1, unable to take PO therapy, and patients discharged to hospice care.
During the intervention period the AMT members received real-time alerts for all blood culture speciation via a paging system. These cases where then reviewed and recommendations were made to the primary care team based off an approved protocol. The primary outcome for the study was time to de-escalation of therapy. Secondary outcomes include hospital length of stay and total duration of therapy.
Results:
A total of 60 patients were include in this study: 30 patients in the pre-intervention group and 30 patients in the post-intervention group. The most common age group was patients 60-69 years of age (43% vs 43%). The most common causative organism for the BSI was found to be Escherichia coli (76.7% vs 50%). During the intervention period a decrease was noted in median time to de-escalation of therapy (2.7 days vs 1.8 days, p=0.0061) and length of stay (5.3 days vs 4.3 days, p=0.0475). There was no statistical difference in the total length of therapy (combined inpatient and outpatient duration) noted between the two groups (9 days vs 9.5 days, p=1).
Conclusion:
The results show a statistically significant decrease in both time to de-escalation and length of stay within the intervention group due to AMT recommendations. This is in line with previous studies and also highlights the benefit de-escalation could have on length of stay in the hospital. Studies with larger samples sizes should be considered to further explore these results.
IRB Status:
Approved
-

Implementation and evaluation of pulmonary arterial hypertension clinical program and pharmacist education at a health-system specialty pharmacy
Timothy Cao, Adam Saulles, and Tara Berkson
Timothy Cao, PharmD, PGY-1 Pharmacy Resident
Preceptors: Adam Saulles, PharmD, CSP, BCACP and Tara Berkson, PharmD, BCACP
Providence Health and Services, Portland, Oregon
Implementation and evaluation of pulmonary arterial hypertension clinical program and pharmacist education at a health-system specialty pharmacy
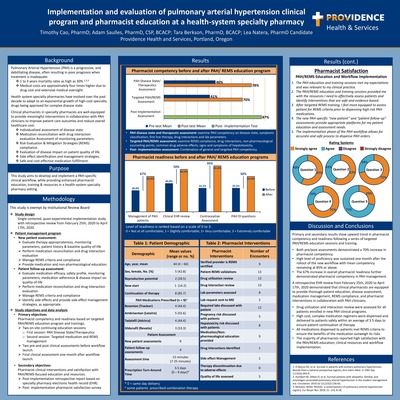
Pulmonary Arterial Hypertension (PAH) is a progressive, debilitating, and costly disease, often resulting in poor prognosis when treatment is inadequate. With an exponential growth of specialty therapies, clinical pharmacists in specialty pharmacies are well-equipped to play an integral role in improving patient care outcomes and reducing overall healthcare costs. By incorporating a PAH-specific clinical program as part of the specialty pharmacy workflow, clinical pharmacists can provide meaningful interventions, such as evaluation of disease-modifying medications through individualized assessment of disease state symptoms, reconciliation of medications to assess for drug interactions, and laboratory parameter, compliance with Risk Evaluation & Mitigation Strategies (REMS) programs, while dispensing medications in a safe and cost-effective manner.
The purpose of this study was to develop and implement a PAH-specific clinical assessments and workflow, while providing enhanced pharmacist education, training & resources in a health-system specialty pharmacy setting.
This was a single-centered, quasi-experimental and implementation study with retrospective review at a health system specialty pharmacy. The primary objective of this study centered on building PAH-specific “new patient” and “patient follow-up” assessments and providing specialty pharmacists enhanced PAH and REMS education and training. The effectiveness of pharmacist education was evaluated based on pre-and- post clinical assessments during two targeted training sessions before the launch of the new workflow, along with a final clinical assessment one-month post-workflow launch. The secondary objective of this study focused on the quality of patient intervention during the implementation phase and pharmacist satisfaction with PAH/REMS-focused education. A retrospective report was run from the specialty pharmacy electronic health record (EHR) from February 2nd, 2020 to April 17th, 2020 for all completed PAH assessments and pharmacist interventions.
Primary objective results found upward trend in pharmacist competency and readiness following two PAH/REMS education sessions. Clinical assessments during pre-implementation phase found average pre-test results of 43.5% and post-test results of 74%, indicating 70% increase in pharmacist competency. High level of proficiency was sustained one-month post-implementation phase with mean competency at 85% and above. Pharmacist readiness in PAH management increased by 67% overall. Secondary objectives found majority of pharmacists were satisfied with the PAH education, implementation process and resources provided. EHR retrospective review identified several meaningful pharmacist interventions, notably drug utilization and interaction reviews, lab parameter assessments, side effect management and medication educations. High cost, complex medication regimens were dispensed according to REMS criteria and delivered to patients safely within an average of 3.5 days to ensure patient continuation of therapy.
PAH clinical program implementation and targeted- education successfully enhanced pharmacists’ clinical knowledge, readiness, and meaningful intervention for PAH population in a health-system specialty pharmacy.
-

Implementing a simplified targeted feedback method to reduce fluoroquinolone prescriptions in emergency departments
Minh Le, Alyssa Christensen, and Brent Footer
Minh Le, PharmD
Alyssa Christensen, PharmD, BCIDP, Brent Footer, PharmD, BCPS
Providence Health System, Oregon
Implementing a simplified targeted feedback method to reduce fluoroquinolone prescriptions in emergency departments
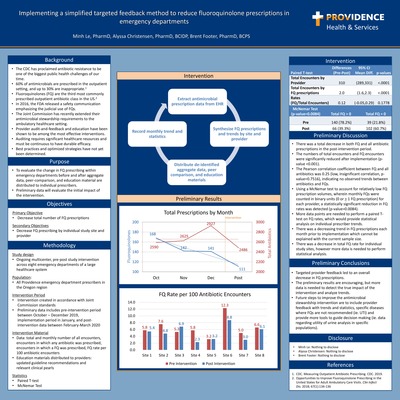
Background: The CDC has proclaimed antibiotic resistance to be one of the biggest public health challenges of our time. Although fluoroquinolones (FQs) are among the most widely prescribed antibiotics in the ambulatory setting, there have been recent efforts to reduce their usage due to mounting concerns regarding their safety profile and resistance patterns. Provider audit-and-feedback has been shown to be among the most effective antimicrobial stewardship interventions, but the auditing process requires significant healthcare resources, is time consuming, and must be continuous in order to have sustained durability. The purpose of this study is to determine if targeted provider feedback and education material can reduce FQ prescriptions independent of prospective auditing and feedback.
Methods: This is an ongoing, multicenter, quasi experimental study across all emergency departments of a large healthcare system within the Oregon region. The primary objective is to decrease overall FQ prescriptions. Secondary objectives include reduction of FQ prescriptions by individual prescriber and study site. Pre-intervention antibiotic data was gathered between October and December 2019. Aggregate FQ prescription data was extrapolated by individual prescriber and study site and distributed in January. Education material containing the latest guideline recommendations and relevant practice pearls was also provided. Post-intervention data was then gathered between February and March 15. This study has been approved and given exempt status by the institutional review board.
Results: There was a total decrease in both FQ and all antibiotic prescriptions in the post-intervention period. Total encounters in which a FQ was prescribed was significantly lower in the post-intervention period with a difference of 2 (95% CI 1.6 to 2.3; p 1 FQ prescriptions) for each provider, there was a statistically significant reduction in FQ rates from 140 providers (78.2%) in the pre-intervention period to 66 (39.3%) in the post-intervention period (p-value=0.0084). There was not enough data to perform statistics on FQ rates per provider or between study sites.
Conclusion: Targeted provider feedback led to an overall decrease in FQ prescriptions. Although the preliminary results are encouraging, more data is needed to detect the true impact of the intervention and analyze trends.
-
 Experience by Sarah Tu and Shuntao Cai")
PD-1 and PD-L1 Inhibitors: A Single Center Medication Assistance Program (MAP) Experience
Sarah Tu and Shuntao Cai
PD-1 and PD-L1 Inhibitors: A Single Center Medication Assistance Program (MAP) Experience
Sarah Tu, PharmD and Shuntao Cai, PharmD, BCOP
Robert W. Franz Cancer Center, Providence Cancer Institute, Portland, OR, USA
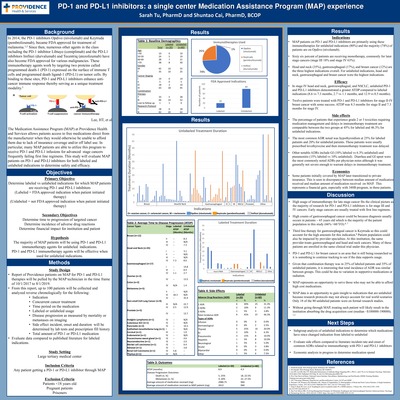
Background: PD-1 and PD-LI inhibitors are a large component of the growing immuno-oncology field and every year there are increasing studies investigating potential indications for these agents. This IRB approved retrospective chart review examines patients in the Medication Assistance Program (MAP) within a large tertiary medical center who are on PD-1 and PD-L1 medications due to financial barriers and/or non-FDA approved regimens (unlabeled indications). This study seeks to evaluate efficacy and safety of PD-1 and PD-L1 for unlabeled vs labeled indications within this population.
Methods: One hundred MAP patients treated with the PD-1 and PD-L1 inhibitors Opdivo (nivolumab), Keytruda (pembrolizumab) and Imfinzi (durvalumab) from October 2017- August 2019 will be analyzed in a reverse chronological order. The following data will be collected from the EMR: patient age, gender, medication, indication, duration of therapy, duration of therapy, labeled or unlabeled usage, if patient had a response, time to disease progression, concurrent therapies, total amount of drug administered, noted side effects, and if the FDA indication has changed since initiation. Labeled indications will be defined as medications that are FDA approved for the patient’s cancer type at time of medication initiation. Unlabeled medications are those not FDA approved for a patient’s cancer type at time of medication initiation. Evaluation of provider notes, lab tests and medication history records will be the primary data source for information collected. Primary objectives include evaluation of labeled vs unlabeled indications for PD-1 and PD-L1 inhibitors. Secondary objectives include determining time to disease progression, incidence of adverse drug reactions, and financial impact for institution and patient.
Results: Out of one hundred patients analyzed, 20% were on PD-1 and PD-L1 inhibitors for unlabeled indications and 80% patients were treated for labeled indications. The top three indications for PD-1 and PD-L1 inhibitors overall were head and neck (35%), gastroesophageal (17%), and breast cancer (12%) which was primarily driven by unlabeled patients. In stage IV head and neck, gastroesophageal, and NSCLC, unlabeled PD-1 and PD-L1 inhibitors demonstrated a greater average time to disease state progression compared to labeled indications (8.6 vs 7.3 months, 2.7 vs 1.1 months and 12.9 vs 0.5 months). The percentage of patients with grade 2 and 3 toxicities were comparable between the unlabeled and labeled indications with total incidence of ADR at 45% for labeled indications and 46.3% for unlabeled indications. The most common ADR requiring medications or delay of therapy was hypothyroidism (25% in labeled and 20% in unlabeled).
Conclusions: The majority of MAP patients are on PD-1 and PD-L1 inhibitors for unlabeled indications with the highest usage of Opdivo (nivolumab) at 74%. From our small sample size, there is promising data that PD-1 and PD-L1 inhibitors may prolong survival for several months longer for various indications including breast cancer, stage IV head and neck, gastroesophageal and NSCLC. These indications may later be incorporated into clinical trials as these agents seek new drug approvals.
-

Pharmacoeconomic impact of patient-centric oncology service model
Kasey Rubin, Samuel Jacobson, and Shannon Buxell
Kasey Rubin PharmD.
Samuel Jacobson PharmD. BCOP, Shannon Buxell PharmD.
Providence Health & Services, Portland Oregon
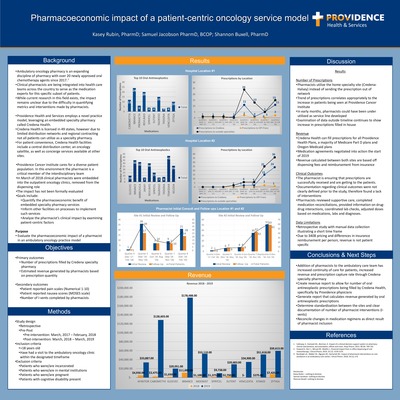
Pharmacoeconomic impact of patient-centric oncology service model
Providence Health & Services recently embedded ambulatory oncology pharmacists into the ambulatory oncology clinic setting. The overall purpose of this retrospective study is to quantify the financial benefits of ambulatory oncology pharmacists as well as quantify patient-centric factors through utilization of an onsite specialty pharmacy. This study was submitted and approved by Institutional Review Board. Electronic health records of patients who visited the ambulatory oncology clinic will be retrospectively reviewed over two time periods: 12 months preceding integration of a pharmacist and 12 months post integration of a pharmacist on the ambulatory oncology team at Providence Portland Medical Center (PPMC). Each group will consist of 250 patients. The following patient data will be collected: Patient MRN, Patient visit encounter (if multiple visits), sex, ICD10 code for diagnosis, number of prescriptions/dispense report, cost of medication, financial revenue, nausea scores, pain scores, and number of Interventions completed by pharmacists. These endpoints will be assessed and an estimated dollar amount will be attached to each non-monetary service provided by pharmacists. Epic projects an equivalent dollar amount per each intervention completed by a pharmacists. This projected dollar amount will be utilized to quantify the benefits of a pharmacist and will be considered as cost-savings. Number of prescriptions/dispense report and cost data will be provided by Providence specialty pharmacy, Credena. Credena utilizes Epic and CPR+. The primary investigator will not access to CPR+ and will defer to secondary investigators to collect prescription data.
Preliminary pharmacoeconomic data will be presented. Clinical results from the addition of the pharmacists show an initial review of the oral antineoplastic in 70% and 86% of patients in sites #1 and #2, respectively. Follow-up calls were made to 55% and 85% of patients in sites #1 and #2, respectively. Patients getting their prescriptions through Credena are continually counseled by Credena specialty pharmacists. Pharmacists reviewing medications reviewed drug-drug interactions, with the true number of interventions not able to be calculated. In conclusion, pharmacists have added both financial and patient centered benefits after integration with the care team.
-

Safe Opioid Prescribing at Discharge
Taylor Goodman, Elva Van Devender, Luetta Jones, and Courtney Barber
Safe Opioid Prescribing at Discharge Taylor Goodman, PharmD; Elva Van Devender, PharmD; Luetta Jones, PharmD; Courtney Barber
Background/Purpose: The opioid epidemic has led to devastating consequences, especially in Oregon, with an average of five Oregonians dying each week from opioid overdose. Opioid prescriptions at discharge are correlated with future continued opioid use. United States providers prescribe more opioids both inpatient and at discharge than other countries, and Oregon providers wrote more opioid prescriptions per person than the national average. Oversupplying prescription opioids can lead to reservoirs of unused medication, creating opportunities for non-medical use and overdose. Pharmacy interventions have shown significant improvement in safe opioid prescribing practices at hospital discharge. However, inpatient discharges still represent a major source of high-volume opioid prescriptions. The purpose of this study is to evaluate hospital discharge opioid prescriptions and to assess the impact of data sharing and education on subsequent discharge prescribing practices.
Methods: This was a retrospective review of discharge opioid prescriptions for adult hospitalist patients discharged from two, large, tertiary hospitals during July 2018, September 2019, and either February 2020 or February 18th thru March 18th, 2020 depending on the location. Eligible patients’ data elements including discharge opioid, quantity of opioid tablets (QTY), morphine milligram equivalence (MME), concomitant benzodiazepine prescription, ordering provider, and ordering department were evaluated for pre and post intervention implementation analysis. Data was collected through a review of orders in the electronic health record (EHR). Further investigation into charts was completed for necessary additional information if needed. The primary outcome is hospitalist group opioid discharge prescribing practices pre and post multiple interventions (EHR changes to default quantity on new orders, addition of MME daily calculation and provider education) and provider education alone presented on either January 21st or February 11th, 2020. Secondary outcomes include department and individual provider prescribing practices. This study has been approved by the institutional review board.
Results: At Hospital A, both the average quantity of tablets and MME per discharge decreased post EHR and education interventions, then increased (25.8 to 23 to 25 and 198.3 to 177.5 to 195.6 respectively) post education only intervention. At Hospital B, a similar trend in both the average quantity of tablets and MME per discharge post interventions (34.9 to 23.3 to 25.8 and 303.5 to 191 to 212 respectively) was seen. The percentage of(62% to 62.7% to 67.5% at Hospital A and 50.6% to 70.2% to 66.5% at Hospital B).
Conclusion: Results comparison prior to intervention (2018) to post intervention (2019 and 2020) indicate that it was effective in promoting safer prescribing practices however education/data sharing only intervention may be more effective when combined with more system orientated interventions. While longer term monitoring and individual provider follow up is needed to elicit the true impact of provider education and data sharing intervention, future efforts should combine multiple interventions. These should target the individual via continued education/data sharing and system processes via workflow adjustments such as encouraging utilizing new opioid orders upon discharge. Targeting specific service lines could help identify more opportunities to promote safer prescribing practices going forward.
-

Standardizing Specialty Pharmacist Follow-Up Frequency in Patients Prescribed Inflammatory Disease-Modifying Therapies
Rochelle Castrillo, Linda Huynh, Tara Berkson, and Adam Saulles
Submission Category Specialty Pharmacy
Purpose Specialty medications for inflammatory conditions have demonstrated decreased effectiveness, safety, and quality of life, largely attributable to inadequate medication adherence. Furthermore, with poorer health outcomes, patients face greater healthcare costs associated with exacerbations, flares, and hospitalizations. Monitoring for non-adherence, side effects, and health status changes is essential for patients diagnosed with inflammatory conditions. The benefit of a standardized pharmacist clinical follow-up assessment is currently lacking in specialty pharmacy literature. This study will implement a standardized pharmacist follow-up frequency guide and determine its clinical value and utility for patient safety and therapeutic goals in newly established patients diagnosed with inflammatory conditions.
Methods A standardized follow-up frequency adjustment guide based on patient-specific factors, such as patient adherence, side effects experienced, and therapy efficacy was provided to all pharmacists where clinical consultations should be conducted at month 0, 1, and 4. After the implementation of the pharmacist guide, the electronic health system record was reviewed for all patients who received an inflammatory condition new patient consultation between August 5th, 2019 and October 4th, 2019. Pharmacist consultations are conducted by utilizing pre-designed assessment forms, the “New Patient Inflammatory Assessment” for initial consults and the “Specialty Medication Management Services (SMMS) Inflammatory Assessment” for follow-up assessments. How often pharmacists consistently stay within the standardized follow-up intervals versus how many times they deviate from the guide for patient care or safety reasons will be evaluated as the primary outcome. Secondary outcomes include categorizing and assessing the reasons for pharmacist deviation, assessing quantity and types of pharmacist (RPh) interventions made during deviations from the guide by medication and condition, evaluate patient reported medication adherence, quality-of-life (QoL) metrics, and pharmacist time spent per assessment. Patient-reported QoL was reported on a scale of 0 to 10, with 0 representing the best QoL and 10 representing poor QoL.
Results There were a total of 154 patients enrolled into the study. Out of the 185 completed follow-up assessments, 36 were deviations. The reasons for pharmacist deviation from the guide included inability to reach the patient during standardized follow-up frequency (41.7%), RPh clinical decision that sooner follow up was necessary (27.8%), patient initiated consult (25%), and RPh failed to attempt follow-up consultation at month 1 and/or 2 (5.6%). Pharmacist interventions occurred predominantly at month 0 (71.7%), month 1 (15.5%), & month 4 (6.6%). The most frequent pharmacist interventions during consult deviations comprised of medication reconciliation (37%), and side effect management (33%), the remaining interventions were equal to or less than 7%. Following the initial assessment, the medication adalimumab and inflammatory condition psoriatic arthritis required the most pharmacist intervention at 32.2% and 21.5% of all follow-up interventions, respectively. However, it was tofacitinib and ankylosing spondylitis, which required the most pharmacist consultation time. Tofacitinib averaged 13.2 minutes and ankylosing spondylitis averaged 15.2 minutes per consultation. Patients taking adalimumab reported missed or late doses most frequently (33.3% of the 24 reported). Although QoL metrics were not consistently reported, there is a notable improvement from baseline to month 4. At month 0, the average patient-reported QoL was 5.6, while after 4 months of treatment, QoL scores improved to 3.6.
Conclusion The standardized pharmacist follow-up frequency guide has provided a clinically meaningful strategy to monitor and follow-up with patients prescribed high-cost, high-risk inflammatory disease-modifying therapies. By establishing that the majority of clinically significant interventions occurred during the standardized frequency intervals, this guide accomplished maintaining patient safety, in addition to aiding patients with their clinical goals and overall quality of life. In addition, this data supports continuing a standard follow-up frequency at month 1 and 4 by demonstrating that no critical interventions were missed and most deviations occurred due to pharmacist’s inability to reach patients during the pre-defined intervals. Although most pharmacist interventions occurred at the recommended intervals, it is important to consider patient-specific factors when determining follow-up frequency. Thus, it is reasonable for specialty pharmacists to utilize a standardized follow-up frequency guide that allows modifications based on clinical judgment to manage patients diagnosed with an inflammatory condition.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}