
-

Employed Mothers’ Satisfaction with the Breastfeeding Provisions in the Patient Protection and Affordable Care Act in Two Northwestern U.S. hospitals
Rebecca Penders
Background: Breastfeeding is the gold standard for infant nutrition. Many workplace barriers to lactation exist for mothers returning to work after the birth of an infant. In 2010 the Breastfeeding Provisions in the Patient Protection and Affordable Care Act (BP-PPACA) was enacted as the first federal breastfeeding law which outlined specifically break time and a place to pump for businesses with over 50 employees who employed hourly wage workers. There is little known about the satisfaction of hospital employees pumping/lactation experience after the BP-PPACA.
Purpose/Aims: The purpose of this study was to determine the extent to which employed mothers' perceived satisfaction in their breastfeeding experiences after the BP-PPACA. A major aim is to determine the extent to which the health policy allows employed mothers to combine breastfeeding and employment at two Northwestern U.S. hospitals since the 2010 law. Data were from self-reported breastfeeding initiation/duration and pumping experiences.
Methods/Approach: This 43-item survey in REDCap-Research Electronic Data Capture was exploratory and descriptive and sent out to all female employees at 2 hospitals in July 2020. The survey included demographic questions, occupation, as well as five Likert-scale satisfaction questions related to the experience with the BP-PPACA. Results: N=215 returned surveys from one large (over 500-bed) hospital and one medium (100-499 bed) hospital. Employees represented a variety of areas: administrate (non-clinical), clinical pharmacy, food service/dietary (other), phlebotomy/ other lab, EKG/other licensed techs, sterile processing, switchboard/ other communications, however most participants were from nursing. Most responses indicated satisfaction 1) with the BP-PPACA, 2) in their own breastfeeding duration and 3) exclusive use of breastmilk, however there were diverse positive and negative experiences 4) in the actual break time and 5) places to pump.
Conclusions: The BP-PPACA are a start for increasing breastfeeding in the U.S. among employed mothers however other policy considerations include support for PUMP for Mothers Act (S. 3170 and H.R.5592), and future building construction to include lactation spaces. Future research should explore paid maternity leave, on-site daycare/bring baby to work, occupational types, salaried employees, tax deductions for businesses for better workplace accommodations, ideal milk expression times for full milk expression and other satisfaction level research for whom these policies are aiming to support.
-

Pain Management Trends among Adults Hospitalized with Cellulitis: An Evidence-based Practice Project
Syndey Pham, Teresa Bigand, Brenda Senger, Kenn Daratha, and Kris Daratha
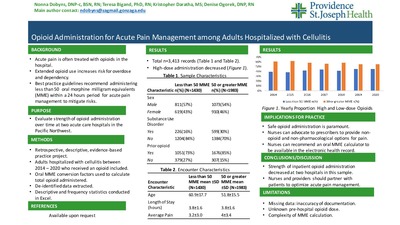
Background: Cellulitis is an infection of the skin causing swelling and acute pain. Two and a half to three and a half million adults seek care in the emergency department annually for this condition. Opioid medications are commonly administered and prescribed for pain, especially following the Joint Commission’s campaign in 2001 characterizing “pain as the 5th vital sign”. An estimated 22% of older adults hospitalized with a painful medical condition receive a new prescription for an opioid medication. Evidence suggests that there is no difference in pain outcomes among adults prescribed opioid versus non-opioid medications for acute pain conditions in the ambulatory setting. Conversely, outcomes favor the use of non-opioids, particularly acetaminophen and non-steroidal anti-inflammatories (NSAIDs), compared to opioids in the treatment of acute pain. Furthermore, best practice guidelines for acute pain management published in 2018 recommend maximizing the use of non-opioids and minimizing the use of opioids. In two acute care hospitals in the Pacific Northwest, prescription pain management for adults treated for cellulitis was previously unknown.
Purpose/aims: Our aim was to determine whether the rate of inpatient analgesics administered to manage pain related to cellulitis changed between the years 2014- 2020 at two acute care hospitals before and after local opioid stewardship efforts.
Methods/Approach: Data were extracted and de-identified from two hospitals in the Pacific Northwest for adults 18 years and older admitted with primary or secondary diagnosis of cellulitis between the years of 2014 and 2020 for a length of stay between 1-7 days. These data were retrospectively analyzed using descriptive statistics, chi-square analyses, and t-tests in excel.
Results:A total of 4,523 records met criteria were included in analysis. In the sample, rate of inpatient opioid administration significantly decreased from 91% to 73% (p
Conclusion: Opioid administration significantly decreased over time in our sample, and non-opioids, particularly acetaminophen, were frequently administered. In these two hospitals, it appears that local opioid stewardship efforts led to decreased opioid administration in alignment with best practice guidelines for managing acute pain for adults hospitalized with cellulitis. Future work should be done to compare pain management strategies over time for other acutely painful, non-surgical conditions treated in the hospital, and to characterize pharmacological pain management strategies post-hospitalization for an acutely painful, non-surgical conditions.
Implications for practice: Nurses should educate patients on best practice guidelines for pharmacological treatment of acute, non-surgical pain. Nurses could also advocate to prescribers to optimize non-opioid pain medications, particularly NSAIDS if patients meet criteria, to manage acute pain in the hospital setting.
-

Exploring the relationship between exposure to nature while at work and burnout among female nurses on day shift
Jamie Roney, Sahar Mihandoust, and Stephanie Dunkle
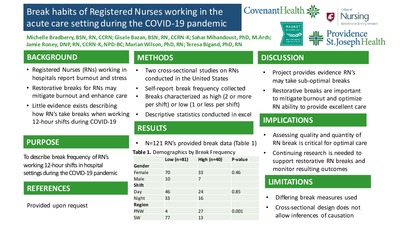
Background: Registered Nurses working extended shifts in the hospital setting may report burnout, which reduces caregiver satisfaction, increases turnover, and potentially translates to delivery of suboptimal patient care. To align with the quadruple aim, efforts are needed to reduce nurse burnout. Limited literature suggests that visual access to nature, either via artwork or exterior landscaping, may reduce burnout. However, more research is needed to understand whether visual access to nature influences burnout among Registered Nurses delivering direct patient care.
Purpose/Aims: The purpose of this study was to explore the relationship between visual access to exterior landscaping or nature artwork and burnout among Registered Nurses.
Methods/Approach: This cross-sectional study recruited female nurses working dayshift in one large medical center to avoid potential confounders of gender and shift on burnout and exterior nature views. Participants were recruited from 6 different nursing units based on the pre-existing characteristics of unit break rooms: 1) exterior nature view and nature artwork(n=2 units; n=16 nurses);2) no exterior nature views but containing artwork of nature scenes (n=2 units; n=18 nurses); 3)no exterior nature view and no nature artwork (n=2 units; n=17 nurses).Nurses self-reported demographics as well as perceived frequency and duration of exterior nature views or nature artwork during an average shift at one point in time immediately following the end of a 12-hour shift. In addition, nurses provided burnout data by completing the Maslach Burnout Inventory (MBI),which characterizes burnout as emotional exhaustion, depersonalization, and personal achievement. Surveys were collected from February –March 2019. Data were analyzed descriptively and using a subset regression model to explore relationships between measured variables.
Results: A total of 51 Registered Nurses working 12-hour day shift in the hospital setting reported on average low to moderate burnout. In the multivariable model, nurses who self-reported more time viewing natural light during a shift reported lower burnout subscales of emotional exhaustion and depersonalization compared to those reporting less time viewing exterior nature during the shift. The subscale of personal achievement was not significantly related to nurses’ perception of nature views.
Conclusion: Our study supports that the amount of self-reported exposure to nature primarily through window views throughout 12-hour shifts may impact nurse burnout scores. However, the burnout subscale of personal achievement appeared to be independent of nature views, suggesting that future work should explore other factors that may support this nurse burnout sub-component.
Implications for Practice: Our study provides preliminary evidence that increasing nurse-perceived exposure to nature through window views of exterior landscaping during a 12-hour day shift may mitigate the amount of burnout reported. Nurses could partner with therapeutic architects to advocate for work and break areas containing windows, balconies, alcoves and indoor/outdoor gardens to enhance opportunities for nurses to view exterior landscaping for greater frequencies during a shift to decrease burnout. Future studies are needed to test long-term outcomes related to nurse views of nature and burnout, acknowledging that solutions to support burnout may require multifactorial approaches.
-

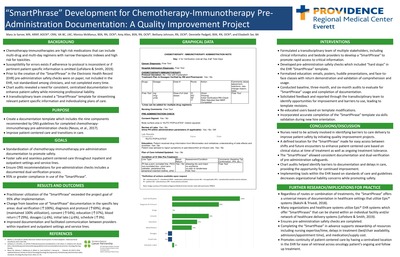
Development of a SmartPhrase in the electronic health record to promote chemotherapy and immunotherapy safety
Mary Jo Sarver, Monica McManus, Amy Allen, Bethany Johnson, Dennielle Padgett, and Elizabeth Ser
Background: Chemotherapy-immunotherapies are high risk medications that can include multi-drug and multi-day regimens with narrow therapeutic indexes and high risk for toxicities. Susceptibility for errors exists if adherence to protocol is inconsistent or if pertinent patient specific information is omitted. Prior to the creation of the "SmartPhrase" in the Electronic HealthRecord (EHR) pre-administration safety checks were on paper, not included in the EHR, not standardized among clinicians, and not completed every time. Chart audits revealed a need for consistent, centralized documentation to enhance patient safety while minimizing professional liability. A trans-disciplinary team created a "SmartPhrase" template for streamlining relevant patient specific information and individualizing plans of care. The template created, included the nine components recommended by the Oncology Nursing Society (ONS) guidelines and recommendations for practice in correlation to chemotherapy-immunotherapy pre-administration checks. Purpose & Goal: Improve patient-centered care and transitions in care while standardizing chemotherapy-immunotherapy pre-administration documentation. Collaborate with inpatient and outpatient settings and service lines to have buy in and continuity related to content and location in the EHR. Ensure ONS recommendations for pre-administration checks included a documented dual verification process in the EHR. Methods: A baseline chart audit was conducted to determine if pre-administration safety checks were within the electronic health record. Based on findings a trans-disciplinary team of multiple stakeholders, including clinical informatics and bedside providers developed a "SmartPhrase" to promote rapid access to critical information. Safety checks included "hard stops" in the "SmartPhrase" template. Formalized education for providers included emails, posters, huddle presentations, job aids, and face-to-face classes with return demonstration and validation of comprehension and usage. Post implementation a three-month EHR audit was preformed, and feedback was solicited from end users to identify opportunities for improvement which lead to template revisions. Re-educated was initiated based on template modifications. Six-month audits re-evaluated usage and completion of documentation. Upon completion of the project the "SmartPhrase" was incorporated into new hire orientation. Results: Practitioner utilization of the "SmartPhrase" exceeded the project goal of 95% after implementation. Change from baseline use of "SmartPhase" documentation were noted in the following specific key areas: dual verification (↑100%),diagnosis and protocol (↑69%), drugs (maintained 100% utilization), consent (↑54%), patient education (↑37%), blood return from venous access device (↑29%), dosages (↓6%), initial labs (↓6%), schedule (↑3%). Implications for practice: Nurses need to be actively involved in identifying barriers to care delivery to improve safety by initiating quality improvement projects. A defined location for the "SmartPhrase" in the EHR made for easy access between shifts and future encounters to enhance patient centered care based on clinical status at time of treatment as well as ongoing treatment tolerance. The "SmartPhrase" allowed consistent documentation and dual verification of pre-administration safeguards. Implementing tools within the EHR based on standards and guidelines decreases organizational liability concerns while promoting safety. Completing the "SmartPhase" in advance supports stewardship of resources including nursing expertise/time, delays in treatment (bed/chair availability, admission/appointment time), and medication/supply cost. Many organizations and healthcare systems utilize Epic® EHR systems which offer "SmartPhrases" that can be shared within an individual facility and/or network of healthcare delivery systems. Standardized documentation promotes continuity of patient centered care in the EHR for ease of retrieval across oncology patient's initial, ongoing and follow up treatment
-

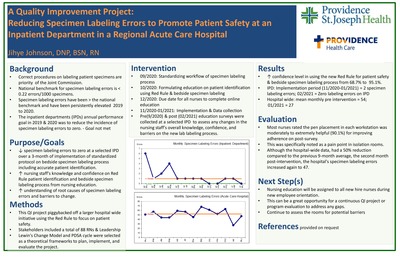
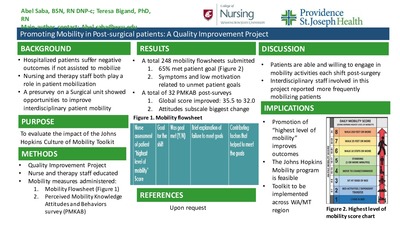
Promoting Mobility in Post-Surgical Patients: A Quality Improvement Project
Abel Sawa and Teresa Bigand
Background: Hospitalized patients suffer negative outcomes related to lack of mobilization activities such as falls with injury or infection. Mobility requires a multi-disciplinary team approach including Registered Nurses (RNs), Certified Nursing Assistants (NA-Cs), and Physical/Occupational Therapists (PT/OTs) to promote best patient outcomes. The Johns Hopkins Culture of Mobility toolkit provides evidence-based practices for integrating multi-disciplinary mobilization efforts for hospitalized patients. This toolkit had not been implemented on a busy orthopedic post-operative nursing unit in one large hospital.
Purpose/aims: To test the impact of the culture of mobility toolkit on caregiver perceptions of mobility barriers and evaluate the implementation of the toolkit on a surgical acute care unit.
Methods/Approach: This quality improvement project was implemented on an orthopedic post-surgery inpatient unit in a large medical center in the Pacific Northwest. A pre-survey was administered to RNs, NA-C's and PT/OTs prior to the implementation of this project, and those findings guided the development of an educational intervention. The education was a poster on the Johns Hopkins Culture of Mobility toolkit with focus on using the toolkit's mobility screening tool presented to RN's, NAC's and PT/OT's. Caregivers were also informed to complete a form each shift on the following: the patient's Highest Level of Mobility score, the patient's mobility goal for the shift, whether the patient met the personal goal, and barriers/facilitators to the patient's ability to meet personal goals. Staff were directed to complete tracking sheets each shift for each patient during a 6-week period. After the intervention, all staff were invited to complete the post-survey to re-assess perceived mobility barriers.
Results: More than 90 caregivers completed the pre-intervention perceived mobility barriers survey, which suggested that staff felt that patient mobilization efforts were time-intensive and posed an injury risk for caregivers. After the education was provided, over 240 mobility tracking sheet were submitted by mainly RN's working night shift, and 65% of caregivers reported that the patient's self-reported mobility goal was met by the end of the shift. Barriers to achieving patient-created mobility goals included inadequate symptom management, reduced patient-specific motivation to move, and lack of adequate resources to safely mobilize patients. A total of 32 caregivers responded to the post-project mobility survey, revealing a significant decrease in overall perceived mobility barriers from pre-intervention levels. PT/OTs reported significantly less barriers compared to nursing staff at both time points.
Conclusion: This project demonstrated that multi-disciplinary staff working on a busy orthopedic post-surgical floor can adopt evidence-based practice tools to promote mobility which may facilitate increased patient mobilization activities. Future projects may include greater adoption of the toolkit throughout the medical center.
Implications for practice: Hospital-based mobility programs such as the Johns Hopkins Culture of Mobility toolkit can mitigate functional decline of adults following hospitalization. Inpatient mobility activities may be enhanced by engaging patients to set and attain mobility goals each shift, partnering with PT/OTs, identifying patient motivation to mobilize, and optimizing symptom management.
-

Improving Outcomes for Pregnant Women with Severe Hypertension
Danette Schloeder
Background: In 2019, a large hospital in Alaska joined the Alaska Perinatal Quality Collaborative (PQC). The first project was the AIM Hypertension Project. The goals of the project were to reduce severe maternal morbidity among preeclampsia cases by 20% and Increase the timely treatment of hypertension to 80%. Other process and structure measures included education, simulation, clinical debriefs, and follow-up visits.
Methods/Approach: The PQC used monthly educational sessions, data collection and review of every case with severe hypertension, and Plan-Do-Study-Act cycles. Data collection occurred over an 18-month period. Cases were identified by the Washington State Hospital Association database and reviewed for timely treatment of severe hypertension. Timely treatment is defined as either a systolic BP of equal to or greater than 160mmHg or diastolic equal or greater than 120mmHg that persists for greater than 15 minutes. The patient must be treated with an anti-hypertensive within 60 minutes of the first blood pressure.
Results: Data collection occurred from July 2019-December 2020. A total of 225 cases were reviewed. The 2020 rate of timely treatment of severe hypertension increased to 81.3% (Goal of 80%). The project was able to reduce the variation in practice. There were three months with 100% timely treatment. In measuring the Severe Maternal Morbidity from Pre-eclampsia cases, the 2019 rate was 8.4%. The2020 rate was 6.9% (Goal 6.72%). The PSJH overall rate was 8.7%.
Conclusions: This project was able to standardize the processes around the management of severe hypertension through order sets, standards of work, education, simulation, and EPIC alerts. This large hospital implemented bedside debriefs and quarterly case reviews of cases that resulted in severe maternal morbidity.
Implications for Practice: This project demonstrated the power of working collaboratively with the statewide PQC to improve patient outcomes. There were significant challenges with COVID-19 priorities and distractions. Overall, both nurses and physicians are committed to timely treatment and the reduction of severe maternal morbidity.
-

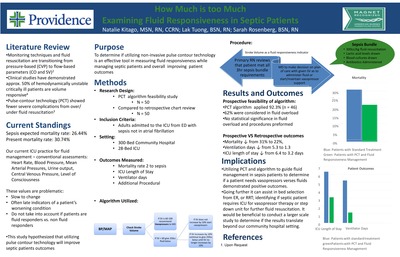
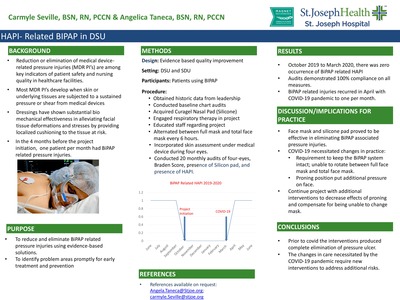
HAPI- Related BIPAP in DSU
Carmyle Seville and Angelica Taneca
Background: Most medical-device related pressure injuries develop when skin or underlying tissues are subjected to a sustained pressure or shear from medical devices. Dressings have shown substantial biomechanical effectiveness in alleviating facial tissue deformations and stresses by providing localized cushioning to the tissue at risk. Our units (DSU and SDU) provide for the monitoring and care of patients with moderate or potentially severe physiologic instability requiring technical support but not necessarily artificial support such as patients on BIPAP management. In the 4 months (June-Sept 2019) before the project initiation, one patient per month had BIPAP related pressure injury.
Purpose: This Hospital Acquired Pressure Injury Improvement was initiated to reduce and eliminate BIPAP related pressure injuries using evidence-based solutions and to identify problem areas promptly for early treatment and prevention.
Methods/Approach: Design: Evidence-based Practice Setting: DSU and SDU Participants for clinical outcomes: Patients using BIPAP Procedures: Historic data was obtained from leadership. Unit nurses acquired curagel nasal silicone pads and engaged respiratory therapy in the project. Staff members were educated in new procedures: alternating mask use between full mask and total face mask every 6 hours, incorporating skin assessment under medical device during 4 eyes, Skin Braden Scores, use of silicone pads, documentation of HAPI. Random chart audits were done to evaluated compliance and clinical outcomes. Results: Between October 2019 through March 2020, there were no BIPAP related HAPI and audits demonstrated 100% compliance on all measures.
Conclusion: Alternating face masks, and application of silicone pads were effective in eliminating pressure injuries related to BIPAP use. Under normal conditions, the interventions produced complete elimination of pressure ulcer.
Implications for practice: Application of evidence to a significant care issue resulted in zero occurrence of BIPAP-related HAPI from October 2019 to March 2020. Audits will continue to help keep project on track. Education and re-education will be done as needed for continued success.
-

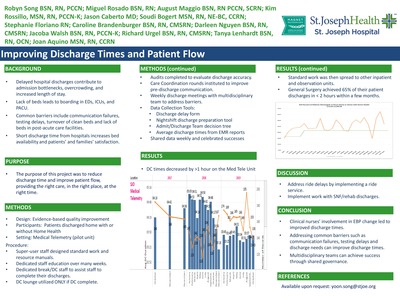
Improving Discharge Times and Patient Flow
Robyn Song, Miguel Ros, August Maggio, Kim Nicole Rossillo, Jason Caberto, Soudi Bogert, Stephanie Floriano, Caroline Brandenburger, Darleen Nguyen, Jacoba Walsh, Richard Urgel, Tanya Lenhardt, and Joan Aquino
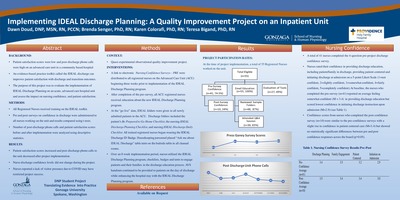
Background: Delays in discharging patients can impact hospital and emergency department (ED) throughput. The complex discharge process makes it difficult to ensure that patients are set up for successful post-hospital care regimens. The focus of this project was to improve discharge times and flow throughout the hospital to align with national standards of providing the right care, in the right place, at the right time. To improve access to beds, The Joint Commission stipulates that hospitals have processes in place to support patient flow throughout the hospital and to use data to drive improvements in patient flow. Failure to regulate flow puts patients at risk for harm and less than optimal care. It also increases clinician burden which may accelerate burnout. A lack of optimal patient flow results in ED boarding and diversions, long waits, and boarding in post-anesthesia care units.
Purpose: The purpose of this project was to improve overall patient throughput within one large acute care hospital by improving discharge times. Baseline discharge times averaged over 4 hours with less than 15% of patients being discharged in less than 2 hours.
Methods: A multidisciplinary patient flow team was charged with improving discharge times and removing barriers to timely discharges. The team consisted of representation from executive leadership, nursing management, pharmacy, physician staff, case management, and frontline staff. Meeting weekly, the team rapidly instituted small tests of change to address the barriers to timely discharges. The Admission Discharge Team facilitated education. Discharge accountability teams on nightshift assisted with preparing patients for discharge. Case Manager/charge nurse rounds were instituted to identify patients ready for discharge and anticipated barriers. Electronic whiteboards were utilized for interdisciplinary communication. Discharge times were reported weekly in a public area on units.
Results: The program resulted in an increase in caregiver engagement in discharges and discharge times. Readmission rates decreased for heart failure patients to below national benchmark. Discharges completed in less than 2 hours improved to almost 30%. Average discharge times decreased from 4 hours to 2 hours and 30 minutes. Also, responses improved to the patient satisfaction question "When I left the hospital, I had a good understanding of the things I was responsible for in managing my heath:" by 25%. Conclusions: Discharge planning that is initiated on the day of admission and addressed ongoing in a uniform fashion by both nursing shifts and ancillary caregivers can alleviate delays on discharge day. An improvement in discharge times improved hospital flow. A focused approach on education throughout the patients stay improved their ability to manage their health at home and reduced readmits.
Implication for Practice: The discharge protocol and procedures will continue to be implemented and evaluated for improvement needs and barriers and expanded to include skilled nursing facility transfers. The discharge process has been implemented in several inpatient units. Discharge times/barriers will be re-evaluated quarterly and the focused patient flow team will make additional adjustments to make the discharge process more efficient.
-

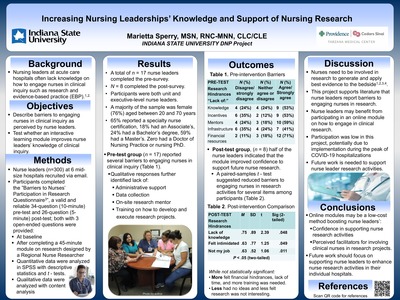
Increasing Nursing Leaderships’ Knowledge and Support of Nursing Research
Marietta Sperry
Background: The lack of leadership support and research knowledge are reported barriers nurses experience in conducting hospital-based research.
Purpose/aims: The purpose was to determine if nursing leadership's knowledge and support of nursing research could be improved through an interactive intervention and to identify their research needs.
Methods/Approach: Design: A translational research study (Doctor of Nursing Practice project) utilizing the Barriers to Nurses' Participation in Research Questionnaire was conducted. Sample: The sample consisted of an even distribution of managers/assistant managers, charge nurses, and directors/chief nursing operating officers. Of the 300 email invitations, 17 nursing leaders completed the pre-test and eight completed the post-test. Setting: Six hospitals within a large health care system in the United States consented to have their nursing leaders receive an email invitation to participate. Intervention: Nursing leaders were provided links for a pre-test, an interactive learning module on clinical scholarship (nursing research), and a post-test. Time frame: Surveys were collected August 19-October 14, 2020. Data: Demographics typical of nurses was collected, such as age, education, position, years of employment, along with perspectives of barriers to nursing research. The Barriers to Nurses' Participation in Research Questionnaire (BNPRQ) provided the basis for the data. The BNPRQ asked which barriers the nursing leader experienced such as lack of time, knowledge, mentors, infrastructure, incentives, nursing research council, leadership support, and training. Participants were given the opportunity to provide some qualitative answers. Paired and un-paired t-tests, descriptive statistics, and a qualitative analysis were performed.
Results: The pre-test group (n = 17) breakdown of nursing leaders was 5 CNOs/directors, 7 assistant managers/managers, and 5 charge nurses. The post-test group (n = 8) consisted of 3 CNOs/directors, 3 assistant nurse managers/managers, and 2 charge nurses. The Pre-test group (n = 17) cited "lack of time" as the number one barrier. Nearly 50% felt a lack of knowledge hindered, and 52.96% either strongly agreed or agreed that the intervention improved their research knowledge. Near this same percentage agreed that lack of time, mentors, and resources also hindered their ability to support or conduct research. However, in the qualitative portion, a lack of leadership support, lack of data collection/tools, need for a hospital-based nurse research mentor, and guidance for developing research inquiry were identified as gaps.
Conclusion: Nursing leaders in this sample reported many of the same barriers that front-line nurses experience including a lack of leadership support for engaging in research. The educational intervention improved nursing leaderships' knowledge and support of nursing research in half of the respondents.
Implications for practice: Hospitals may benefit from providing nurse leaders the basic tools of research, local leadership support, technical advising, and a designated nurse researcher contact in order to facilitate and support nursing research.
-
 by Marietta Sperry and Kimberly Kohlieber")
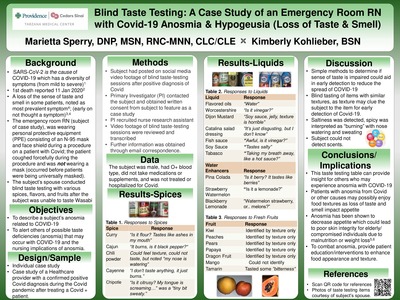
Blind Taste Testing: A Case Study of an Emergency Room RN with Covid-19 Anosmia & Hypogeusia (Loss of Taste & Smell)
Marietta Sperry and Kimberly Kohlieber
Background: Anosmia, or the loss of taste and smell, is an important symptom for nurses to screen for among patients, as this can result in a poor appetite which impairs healing. In the early stages of the COVID19 pandemic, anosmia was not a known symptom indicative of infection with the virus. Yet, one Registered Nurse who was working in an Emergency Room received a positive COVID test following a workplace exposure to the virus while wearing personal protective equipment, and began to complain of anosmia shortly thereafter. Because the anosmia persisted, his spouse conducted blind taste test on him in their home with various spices, flavors, and fruits. The nurse subsequently posted about the experience on social media.
Purpose: The purpose of this case study is to describe one healthcare provider's experience with anosmia associated with a confirmed positive Sars-Cov-2 diagnosis.
Methods: An individual case study was conducted on a Healthcare provider with a confirmed positive COVID diagnosis early in the year 2020 during the COVID pandemic. The individual was a male who was employed as an emergency room Registered Nurse. He was not on any medications or supplements, reported no past medical conditions, and received no treatment or hospitalization during the period of anosmia. The nurse’s spouse blindfolded him and administered an array of spices, flavored liquids, and fruits, asking him to distinguish what he was tasting and smelling. The spouse then recorded all responses and posted results to social media. The project lead of this case study reviewed the information on the social media post, contacted the couple, and received permission to more widely share the findings.
Results: Based on information posted on social media, the nurse was unable to distinguish various spices, or liquid flavorings. While the nurse was able to identify fruits based on texture, he could not detect any distinct flavors such as sweetness. The nurse reported, “I cannot smell a thing; everything tastes bland. Conclusion: Blinded taste-testing is a feasible and low-cost method for confirming the symptom of anosmia among those who may be infected with the COVID virus. Future work should focus on supporting affected individuals with anosmia to maintain healthy nutritional intake despite the absence of taste and smell while ill.
Implications for Practice: Taste and smell deficiencies may occur with SarsCov-2 infection. Nurses should be screen for this symptom among patients and recommend COVID-testing where appropriate to drive early intervention and treatment of the virus. Additionally, because taste and smell normally help drive appetite, nurses should assess for deficiencies in nutritional intake among individuals with anosmia to support a healthy diet for optimal healing.
See agenda for the June 14, 2021: Providence Nurses Supporting Health for a Better World here
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.





{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}