
-

Agenda: Providence Nurses Supporting Health for a Better World
2021 Providence RN Conference
Agenda for the 2021 Providence RN Conference
-

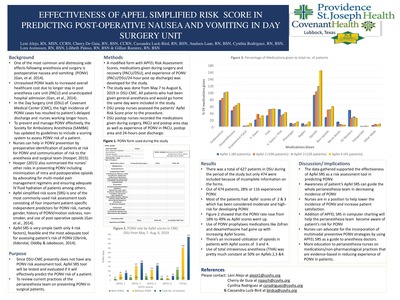
Effectiveness of Apfel Simplified Risk Score in Predicting Postoperative Nausea and Vomiting in Day Surgery Unit
Leni Alejo, Cherry de Guia, Cynthia Rodriguez, and Cassandra Luck-Bird
Background: Postoperative nausea and vomiting (PONV) continues to be a perioperative complication despite improvement in quality and safety of anesthesia care causing an increased overall healthcare cost and sometimes serious physical complications. The American Society of PeriAnesthesia Nurses (ASPAN) supports that risk assessment for PONV helps with its prevention which is in line with the Society of Ambulatory Anesthesia's (SAMBA) current guidelines for PONV management. Literature supports that PONV can be predicted and prevented in patients by assessing risk factors such as gender, smoking status, history of PONV and use of postoperative opioids, among others. At present there is no formal PONV risk assessment tool that will help the perioperative team prevent this unpleasant complication from surgery.
Purpose: The purpose of the study is to determine the effectiveness of APFEL Simplified Risk Score (SRS) in predicting PONV and apply this tool to help prevent PONV in patients undergoing surgery.
Methods: A group of nurses conducted a quality improvement study in the adult day surgery unit of a tertiary hospital in northwestern Texas was done from May 7, 2019 to August 2, 2019. The APFEL SRS (a PONV risk assessment tool) was used in the study because of its practicality and literature-supported effectiveness. A form was devised consisting of patient's APFEL SRS score from 0-4 (0 = no PONV risk, 1 = low PONV risk, 2 = moderate PONV risk and 3-4 = high PONV risk). A list of medications received before, during and after surgery including anesthesia, pain medicines and antiemetics and record of PONV experience after surgery and 24 hours post discharge was also collected. APFEL SRS scores were compared to the likelihood of developing PONV.
Results: A total of 474 patients who received general anesthesia and discharged the same day was included in the study. 17% of patients had an APFEL SRS of 1, 40% with APFEL SRS of 2, 34% with APFEL SRS of 3 and 9% with APFEL SRS of 4. The patients' experience of PONV increased as their risk scores went up. Data showed 18% PONV experience in patients with APFEL SRS of 1, 17% in APFELSRS of 2, 30% in APFEL SRS of 3 and 49% in APFEL SRS of 4. The results showed that the use of prophylaxis drugs for PONV did not correlate with APFEL SRS scores. It was noted that patients with higher APFEL SRS scores also received more narcotics.
Conclusion: The use of APFEL SRS is effective in predicting PONV and awareness of the patient's PONV risk will help the perioperative team prevent and manage its care.
Implications for practice: Since nurses are in position to assess the PONV risk of the patients, adapting APFEL SRS tool will ease the communication of the risk to the anesthesia and surgical team. Awareness of the patient's risk will help doctors do their part in preventing and treating PONV, whereas nurses can use nonpharmacological interventions an
-

Inpatient Registered Nursing Use of Evidence-Based Practice Tools to Manage Withdrawal Symptoms among Adults Hospitalized with Acute Alcohol or Opioid Withdrawal: A Needs Assessment
Julie Baker and Teresa Bigand
Background: Patients who suffer from alcohol or opioid use disorder face unpleasant and potentially life-threatening complications related to substance withdrawal when hospitalized. Evidence suggests that the use of a standardized tool to rate withdrawal severity and direct treatment, including score-driven medication dosing to alleviate withdrawal, leads to improved clinical outcomes. However, clinical nurses working in the inpatient medical-surgical specialty in a large medical center questioned whether all nurses were effectively using evidence-based practice (EBP) tools to assess and treat alcohol or opiate withdrawal severity.
Purpose/Aims: To understand nursing practice at one hospital regarding use of ministry-specific evidence-based practice tools for rating symptom severity for alcohol and opioid withdrawal.
Methods/Approach: A needs assessment using a cross-sectional survey was conducted to understand nursing practice regarding use of two EBP tools for rating withdrawal symptom severity: the Clinical Institute Withdrawal Assessment for Alcohol (CIWA), and the Clinical Opioid Withdrawal Scale (COWS). Two fictitious withdrawal case studies were developed: one illustrating an inpatient withdrawing from alcohol, and the other depicting withdrawal from opiates. Professional Development Specialists collaborated to enact the scenarios and video recorded each patient case. Nurses working on adult medical-surgical units received an electronic survey link containing the written and recorded patient cases. Nurse participants were instructed to first read and watch each case, then to calculate either a CIWA or COWS score based on the presented cases.
Results: A total of 61 Registered Nurses completed the survey out of a possible 191 eligible nurses. Of these, 97% correctly scored the case illustrating opiate withdrawal using the COWS tool. However, only 35% correctly assigned the CIWA score based on the alcohol withdrawal exemplar. In all, 60% of participants assigned a higher symptom severity than expected using the CIWA tool. The CIWA items with the most inconsistent scores were anxiety, agitation, and visual hallucinations.
Conclusion: Nurses at our ministry responded positively to completing a survey featuring written and videotaped case scenarios to identify gaps in practice using the CIWA and COWS tools. Our innovative needs assessment pointed to a gap in standard practice for using the CIWA but not the COWS tools. Targeted education on enhancing nursing assessment of anxiety, agitation, and visual hallucinations in this population may optimize symptom rating and subsequent protocol-driven treatment.
Implications for Practice: Improper scoring with the CIWA tool could trigger an inappropriate medication dose administered to the patient. A future opportunity to educate nurses in our ministry could lead to an improvement in appropriate alcohol withdrawal symptom rating and treatment.
-

Exploring the Relationship Between COVID-19 Unit Designation and Nurse Burnout Syndrome
Gisele Bazan, Tiffany Patterson, Kelsey Sawyer, Jamie Roney, Erin Whitley, Sahar Mihandoust, and JoAnn Long
Background: The COVID-19 pandemic impacted healthcare due to surges in infected patient and respiratory failure. Nursing burnout syndrome (NBS) results from occupational factors leading to mental health problems. Nurses working in intensive care units (ICUs) dedicated to caring for COVID-19infected individuals may be even more susceptible to NBS due to increased burdens of futile care delivery and high mortality rates within overstretched healthcare systems. Identifying socio-demographic, work-related, and psychological predictors of NBS may help organizations mitigate, or at least minimize, the negative psychological impact on ICU nurses working during future pandemics.
Purpose/Aims: The aim of this study was to compare burnout levels in ICU nurses providing direct care to COVID infected patients with nurses caring for non-COVID infected patients.
Methods: An observational descriptive study was conducted using 1) a case-controlled prospective quantitative comparative design to compare neonatal and pediatric ICU to cardiac and medical ICU survey scores measuring nurse burnout, work-related, and psychological predictors of NBS and 2) across-sectional longitudinal quantitative causal and comparative study design comparing NBS scores for nurses working in a cardiac and medical ICU captured in 2019 prior to the COVID-19 pandemic to scores captured in the same units after conversion to dedicated COVID-19 ICUs in 2020. This study will explore the relationship between three subscales(Emotional Exhaustion, Depersonalization, and Personal Accomplishment) of the Maslach Burnout Inventory (MBI) as "outcome variables" and exposure to COVID-19 infected patients during 12-hour shifts worked as "explanatory variables" in a subset regression model. The study will also measure four subscales (Vocation, Finances, Health, and Social Relationships) associated with post-traumatic stress disorder using the Well Being Instrument(WBI) as control variables. A convenience sample of direct care registered nurses working in four ICUs in a large tertiary care hospital will be recruited to participate in the study. Female nurses working day shifts were surveyed in February and March 2019in two ICUs. In November 2020, four ICUs were used for sampling of both male and female nurses working either day or night 12-hour shifts based on designation as COVID-19 ICUs.
Results: Researchers hypothesize burnout scores among nurses working in neonatal and pediatric ICUs will be less than burnout scores for nurses working in designated COVID ICUs. Additionally, investigators hypothesize nurse burnout measured in cardiac and medical ICUs in 2019 will be less than measurements obtained in 2020 after the same ICUs converted into COVID ICUs. This study will also analyze participant socio-demographic and work-related data for psychological predictors of NBS.
Conclusion: NBS has been identified as a global problem facing ICU clinicians. Pinpointing associations betweenCOVID-19 infection and nurse burnout may lead to innovative strategies to mitigate burnout in those caring for the most critically ill individuals during future pandemics.
Implications for practice: Further research is required to establish relationships between socio-demographic and work-related psychological predictors of NBS. Understanding relationships between these variables may guide development of strategies to build nurse resilience and decrease NBS in ICU settings impacted during pandemics.
-

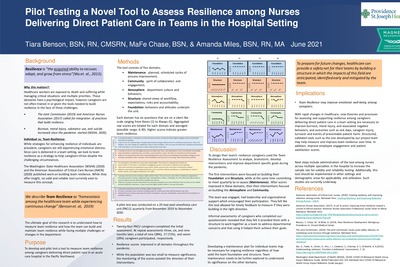
Pilot Testing a Novel Tool to Assess Resilience among Nurses Delivering Direct Patient Care in Teams in the Hospital Setting
Tiara Benson, Ma Fe Chase, and Amanda Miles
Background: With the appearance of the COVID-19 pandemic, nurse emotional well-being has suffered, with burnout being highly reported. Team resilience may mitigate feelings of burnout, and is defined as homeostasis among the healthcare team while experiencing continuous change. Strategies for enhancing resilience of individuals are prevalent, yet nurses often deliver care in a team setting. While some literature offers insight on nurse team resilience, no valid and reliable tools currently exist to measure this concept. Purpose: To develop and pilot test a tool to measure team resilience among nurses delivering direct patient care in an acute care hospital in the Pacific Northwest. Methods: Nurse leaders and direct patient caregivers at one large, urban hospital partnered to conduct a comprehensive review of the literature to develop a team resilience questionnaire. Using concepts from Gesalt theory, action change methodology, and incorporating components of the health care environment, the final tool consists of five domains. They are: 1) maintenance, defined as planned, scheduled cycles of process improvement; 2) community, defined as spirit of collaboration and engagement; 3) atmosphere, defined as department culture and behaviors; 4) structure, defined as shared views of workflow, expectations, roles and accountability; and 5) foundation, defined as behaviors and attitudes that underpin the unit. Each domain is measured with six questions (30 questions total) measured on a Likert like scale ranging from Never (0) to Always (4). Raw scores are summed to calculate a total for each domain (possible range: 0-24) and cumulatively for all domains (possible range 0-120). Higher scores indicate greater team resilience. To evaluate acceptability and feasibility of the assessment tool, a small pilot test was conducted on nurses working on a 20-bed post-anesthesia unit (PACU) from November 2019 to November 2020. Results: Twenty-four PACU nurses completed the initial assessment. At repeat assessments three, six, and nine months later, a total of nine, 17, and seven nurses participated, respectively. Responses analyzed using Chronbach’s Alpha supporting an internal reliability greater than 0.66 for each cycle. Informal assessments of nurses who completed our questionnaire revealed that they felt it provided them with a structure to work together as a team to address departmental concerns and that using it helped them achieve their goals. Discussion: A total of 24 nurses responded to our questionnaire and over a one-year span, between 29 and 71 percent of this cohort participated in repeat assessments. Next steps include administration of the tool among nurses across multiple specialties in the hospital to increase the sample size for validity and reliability testing. Implications: With rapid changes in healthcare, processes for assessing and supporting resilience among nurses delivering direct patient care in a team setting are necessary to support nurse emotional well-being and prevent negative outcomes such as turnover. Structured, validated tools such as the one developed by our project team may help measure and improve team resilience over time.
-

Do Compassion Rounds Improve Professional Quality of Life for Nurses ?
Deepti Bhatnagar and Martha E.F. Highfield
Background: When RN worklife quality is positive, nurse and patient outcomes are positive (e.g, RN retention and patient satisfaction), and when worklife quality is negative, outcomes are negative (e.g., RN disengagement and errors).Yet professional quality of life(QOL)among RNs in progressive care units (PCUs) is undocumented. Stamm’s framework of compassion satisfaction and fatigue guided this study. Purpose: The purpose was to test the effect of supportive groups on professional quality of life. The hypothesis: Compassion Rounds (CR) will improve compassion satisfaction and reduce compassion fatigue among PCU RNs. Methods/ design: Using a quasi-experimental design we measured RNs’ professional QOL once before and once after CR using the well-established ProQOL—a30-item, self-report instrument that yields 3 ordinal subscale scores: Compassion Satisfaction (CS), Burnout (BO), and Secondary Traumatic Stress (STS).Paper-and-pencil demographic sheets and ProQOLs were coded for paired analysis. Return of confidential questionnaires documented consent. After initial data collection, Palliative and Spiritual Care staff facilitateda10-week CR intervention consisting ofbiweekly,30-45 minute, simultaneous live/online, open-ended discussions with staff RNs. Meetings focused on challenges enacting the RN helper role. The sample was an inclusive one of85PCU RNs in a 377-bed, Magnet-recognized, nonprofit facility. Results: Overall response rate was high (44%; N=39). Eighteen (18) respondents attended CR between 1 and 10 times (M= 3). Mean age was 35, and a majority reported female gender(89%), BSN preparation (75%), and no specialty certification (74%). Respondents were ethnically diverse. Using ProQOL cut scores, 7 individuals reported high STS; the remainder reported moderate to low BO, STS, and CS. Inferential t-testing of paired pre/post ProQOL scores (n = 10pairs) showed a pre-CR to post-CR rise in both BO (pre M = 23; post M = 28) t(8) = -2.3, p = .05 and STS scores(pre M = 22; post M = 33) t(8) = -3.5, p = .008. CS subscale scores decreased(pre M = 28; post M = 18) t(8) = 3.7, p = .005. Independent t-testing using all data yielded similar results (p < .05). The hypothesis was rejected. Conclusions: RN professional QOL deteriorated during CR, but no counterfactual exists; CR may have prevented worse outcomes. The PCU housed COVID-19 patients, and data were collected during peak hospitalizations. Moreover, completing ProQOL could have increased respondent self-awareness, and 10 weeks of CR may have been long enough to raise issues without resolving them. ProQOL scores are screening only and so must be cautiously interpreted (Stamm, 2010). Implications: Implications include a need for staff-identified strategies for group empowerment, as well as attending to individual risks for depression, PTSD, or burnout. RNs can access the free ProQOL to aid in guided career counseling. Moreover, further CR and PCU RN studies are warranted. For example, post-pandemic ProQOL data from the same PCU population might differentiate persistent downward trends from transient, self-resolving ones
-

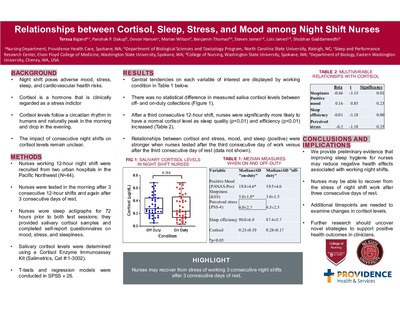
Relationships between Cortisol, Sleep, Stress, and Mood among Night Shift Nurses
Teresa Bigand, Panshak P. Dakup, Devon Hansen, Marian Wilson, Benjamin Thomas, Steven James, Lois James, and Shobhan Gaddameedhi
Background: Working night shift is a physical and emotional stressor related to negative health outcomes. Cortisol is a biomarker that has been related to an increased risk for metabolic syndrome among adults. Cortisol levels follow a circadian rhythm in humans; levels reach a peak in the early morning and drop to the lowest level in the late evening. Changes in cortisol levels have been related to changes in mood or sleep and to exposure to stressful situations. In a group of Registered Nurses, the impact of consecutive 12-hour night shifts on relationships between cortisol levels, sleep, stress, and mood, was not well-defined.
Purpose: To determine relationships between cortisol, sleep, and self-reported mood and stress among nurses working 12-hour night shift after a third consecutive day of work and after a third consecutive day of rest. Methods: Nurses working 12-hour shifts were recruited from two major hospitals in an urban city in the Pacific Northwest to participate in a variety of tests immediately after finishing a third consecutive 12-hour shift and again after a third consecutive day off work. Nurses wore wrist actigraphs for 72 hours prior to both test sessions as an objective measure of sleep. During each test session, nurses completed self-report questionnaires to describe mood, stress, and sleep quality and also provided saliva samples from which cortisol levels were measured. Results: A total of 44 night shift nurses met criteria for data analysis. After a third consecutive 12-hour shift, nurses were significantly more likely to have a normal cortisol level as sleep quality (p<0.01) and efficiency (p<0.01) increased. Expected relationships between cortisol and stress, mood, and sleep were stronger when nurses were tested after the third consecutive day of work versus after the third consecutive day of rest.
Conclusion: We provide preliminary evidence that improving sleep hygiene for nurses may reduce negative health effects associated with working night shifts. Furthermore, nurses may be able to recover from the stress of night shift work after three consecutive days of rest.
Implications for practice: Registered Nurses need to provide 24-hour care to hospitalized patients, and further research should uncover strategies to support positive health outcomes for these clinicians. While our sample was small, we hypothesize that improving sleep hygiene for nurses working consecutive 12-hour night shifts may support health outcomes. Future studies with more frequent cortisol measures are needed to examine time-sensitive changes in cortisol levels.
-

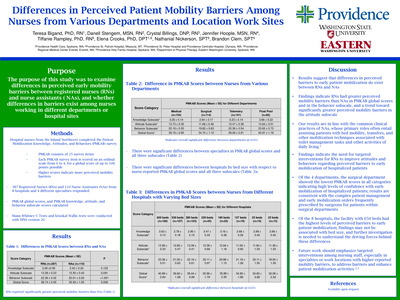
Differences in Perceived Patient Mobility Barriers Among Nurses from Various Departments and Location Work Sites
Teresa Bigand, Danell Stengem, Crystal Billings, Jennifer Hoople, Tiffanie Rampley, Elena Crooks, Nathaniel Nickerson, and Brandon Clem
Background: Hospitalized patients suffer negative outcomes related to lack of mobilization activities such as falls with injury or infection. Mobility requires a multi-disciplinary team approach including Registered Nurses (RNs), Certified Nursing Assistants (NA-Cs), and Physical/Occupational Therapists (PT/OTs) to promote best patient outcomes. The Johns Hopkins Culture of Mobility toolkit provides evidence-based practices for integrating multi-disciplinary mobilization efforts for hospitalized patients. This toolkit had not been implemented on a busy orthopedic post-operative nursing unit in one large hospital.
Purpose/aims: To test the impact of the culture of mobility toolkit on caregiver perceptions of mobility barriers and evaluate the implementation of the toolkit on a surgical acute care unit.
Methods/Approach: This quality improvement project was implemented on an orthopedic post-surgery inpatient unit in a large medical center in the Pacific Northwest. A pre-survey was administered to RNs, NA-C's and PT/OTs prior to the implementation of this project, and those findings guided the development of an educational intervention. The education was a poster on the Johns Hopkins Culture of Mobility toolkit with focus on using the toolkit's mobility screening tool presented to RN's, NAC's and PT/OT's. Caregivers were also informed to complete a form each shift on the following: the patient's Highest Level of Mobility score, the patient's mobility goal for the shift, whether the patient met the personal goal, and barriers/facilitators to the patient's ability to meet personal goals. Staff were directed to complete tracking sheets each shift for each patient during a 6-week period. After the intervention, all staff were invited to complete the post-survey to re-assess perceived mobility barriers.
Results: More than 90 caregivers completed the pre-intervention perceived mobility barriers survey, which suggested that staff felt that patient mobilization efforts were time-intensive and posed an injury risk for caregivers. After the education was provided, over 240 mobility tracking sheet were submitted by mainly RN's working night shift, and 65% of caregivers reported that the patient's self-reported mobility goal was met by the end of the shift. Barriers to achieving patient-created mobility goals included inadequate symptom management, reduced patient-specific motivation to move, and lack of adequate resources to safely mobilize patients. A total of 32 caregivers responded to the post-project mobility survey, revealing a significant decrease in overall perceived mobility barriers from preintervention levels. PT/OTs reported significantly less barriers compared to nursing staff at both time points.
Conclusion: This project demonstrated that multi-disciplinary staff working on a busy orthopedic postsurgical floor can adopt evidence-based practice tools to promote mobility which may facilitate increased patient mobilization activities. Future projects may include greater adoption of the toolkit throughout the medical center.
Implications for practice: Hospital-based mobility programs such as the Johns Hopkins Culture of Mobility toolkit can mitigate functional decline of adults following hospitalization. Inpatient mobility activities may be enhanced by engaging patients to set and attain mobility goals each shift, partnering with PT/OTs, identifying patient motivation to mobilize, and optimizing symptom management.
-

Feasibility of launching a multi-state nursing health study in the midst of the COVID-19 pandemic
Ross Bindler, Shaekira Niehuser, Trisha Saul, and Teresa Bigand
Background: The Quadruple Aim recommends that healthcare institutions support clinician well-being as a strategy to improve patient and caregiver outcomes. During the COVID-19 global pandemic, Registered Nurses (RNs) working full-time, 12-hour shifts have reported increasing health concerns. Therefore, research documenting objective information on preventive health habits of RN’s is needed to support nursing well-being. Yet, conducting bio-behavioral research in this population, especially during the pandemic, presents with unique challenges. Purpose: The purpose of this pilot study to assess the feasibility of collecting and evaluating health data from RNs working full-time, 12-hour shifts across the United States during the COVID-19 pandemic. Methods/Approach: This observational descriptive study recruited 12-hour shift RNs working in a large health system in the United States. RNs wore a wrist actigraph for 10 days, maintained a seven-day electronic food diary, tracked daily step counts using a wrist pedometer, and optionally provided two stool samples for sequencing analysis. Nurses completed an online screening form to assess for study eligibility, and were contacted by a research team member to provide consent if they met eligibility criteria. Research staff created and shared a digital workbook to explain the protocol as well as an interactive online course to provide standardized education on completing electronic food diaries. Participants were mailed devices for tracking health habits. Research staff were available to participants via phone call or email to answer questions at any point during the study. Participants were invited to complete an optional post-study feedback survey to describe the experience of being involved in the study. Recruitment began in October 2020 and the study is still open for participant enrollment. Results: At this time, 82 nurses met study criteria and 49 consented to participate (n=27day shift and n=22night shift). Of these, 37 volunteered to provide a stool specimen. Of the consented nurses, a total of 5 have withdrawn for reasons such as family or school issues. Out of 32 nurses who have completed the study, 22 provided a stool specimen, 2 forgot to collect despite consenting, and9 nurses provided feedback where 66% reported reviewing the online module course. Of those who completed the study, 100% successfully captured sleep data using the wrist actigraph, yet 15.6% required research staff assistance with documenting some aspect of the food diaries. Conclusion: Preliminary findings suggest that it is feasible for nurses to provide objective health information in the context of working full-time, 12-hour shifts during a global pandemic. Future work is needed to understand best strategies for conducting bio-behavioral research among RNs providing direct patient care in the hospital setting. Implication to Practice: Research is needed to characterize health habits of nurses, particularly those providing full-time, direct patient care, to support caregiver well-being and facilitate optimal patient outcomes. Preliminary findings suggest that while barriers exist that restrict nursing involvement in bio-behavioral studies, especially during the pandemic, nurses may successfully participate in studies which could leverage understanding of short and long-term health needs for this population.
-

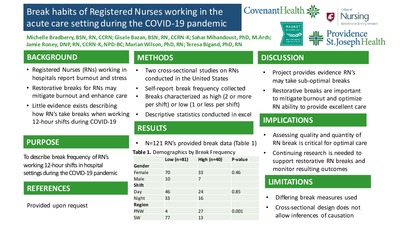
Break habits of Registered Nurses working in the acute care setting during the COVID-19 pandemic
Michelle Bradberry, Gisele Nicole Bazan, Sahar Mihandoust, Jamie Roney, Marian Wilson, and Teresa Bigand
Background: Nurses report high levels of burnout and stress while working in the acute care setting, especially during the current COVID-19 outbreak. Evidence suggests that taking a restorative break during an extended, 12-hour shift may help mitigate stress and translate to better patient and caregiver outcomes. Yet, little is known about how Registered Nurses report taking breaks in the context of the pandemic.
Purpose/Aims: The purpose of this project was to describe the frequency of breaks reported by nurses working 12-hour shifts during the COVID-19 pandemic, and to test for demographic differences between nurses reporting fewer compared to more breaks on average during a shift.
Methods/Approach: Registered Nurses delivering direct patient care in a 12-hour full-time position in the hospital setting in two different regions in the United States (U.S.) were recruited for two different studies during the peak of the COVID-19 outbreak. Demographic data were collected via self-report in both studies. To measure quantity of breaks taken during a shift, participants in the Southern U.S. region were asked, “What is the frequency of breaks you normally take during your shift between 0 (no breaks) to 4 (all provided breaks)?”. Nurse participants in the Pacific Coast study were asked, “In a typical shift, how many 15- minute breaks do you take?” and “In a typical shift, how many 30-minute breaks do you take?”. The numbers of breaks reported were summed to yield a total frequency of breaks taken by the participants in both studies. Data were analyzed using descriptive statistics to quantify the number of breaks reported, and bivariate tests assessed group differences between reporting high or low frequency of breaks.
Results: A total of 121 nurses working either in the Pacific Coast (n=31) or in the southern U.S. (n=90), were included. Across the dataset, the average number of breaks reported was 1.5 and nurses surveyed in the Southern U.S. were significantly more likely to report taking one or fewer breaks during their 12-hour shift compared to nurses working in states along the Pacific coast. There were no noted differences in education, age, gender, or shift type with respect to reported break frequency.
Conclusion This project provides an initial glimpse into self-reported breaks of nurses delivering frontline care in the hospital setting during the COVID pandemic. Nurses may not be taking all break opportunities while working during the pandemic, and efforts should be made to support the ability of frontline caregivers to consistently take all restorative breaks each shift.
Implications for Practice: Strategies for enhancing nurses’ abilities to take restorative breaks are critical, especially for nurses working on the front lines during the COVID-19 pandemic. Ensuring adequate quality and quantity of breaks for frontline caregivers may mitigate caregiver burnout and enhance well-being, potentially translating to delivery of optimal patient outcomes. Our findings are limited as strategies for measuring nursing breaks were not uniform across the two studies. Future work is needed to further characterize breaks and related outcomes among Registered Nurses providing direct patient care during COVID.
-

Utilizing a Social Media Platform to Increase Participation in a Virtual Journal Club
Alex Bubica and Trisha Saul
Background: A virtual journal club (VJC) is a place where nurses can read, synthesize, and discuss research and evidence-based practice articles. There is a well-known time lag of disseminating this knowledge from bench to bedside. In 2016, a 300-bed community hospital constructed a VJC to educate nurses on the latest studies. In 2016 and 2017, this VJC was used via an intranet-based platform with little success. Main barriers included (1) no access outside of work and (2) difficulty following threads leading to in-cohesive interactions. In 2018, a website was created. This platform had one fatal flaw, a multistep verification process to gain access, with the verification email being routed into spam. In late 2018, a literature search was done to identify best practices. A number of articles were reviewed with results indicating that the utilization of a social media platform increased participation.
Purpose/Aim: The purpose of this evidence-based practice project was to offer a social media platform for all nursing staff to participate in a VJC. Aim 1: To set up an organizationally approved social media account for the VJC. Aim 2: For the participants to have access to the VJC at home and at work. Aim 3: To increase the number of participants using the VJC.
Approach: The Nursing Research Council used the Rosswurm and Larrabee model as a systematic evidence-based practice process. Step one, assess the need for change, was done mid-2018 when platform problems were identified. Steps two and three: link problem with interventions and outcomes, and synthesize best evidence, was done at the end of 2018. Step 4, design a plan, was discussed in detailed early in 2019, and a number of traditional social media platforms were reviewed but did not meet institutional security measures. One social media platform that the organization already used was identified. Step 5, implementing and evaluating a plan, involved three phases. Phase one was exploratory. An account was created with basic information. Council members and the Education team were invited to test out the accessibility (i.e., desktop and phone application). Phase two included a soft-opening with the VJC completely set up, and Council members each did an initial post and a response. All potential barriers were evaluated and addressed. Phase 3, hospital go-live in May, included a number of promotional techniques (i.e., QR codes, emails, signs). Stage 6, integrate and maintain is discussed below.
Results: Aim 1 and Aim 2 were successfully met by identifying a user-friendly social media platform, that resembles the basic principles of a traditional social media news feed. Aim 3 was measured by number of total members and posts. Compared to 2018, 2019 increased in VJC members from 22 to 44 and total number of posts from 46 to 106.
Conclusion & Implications: Advances in nursing practice need to be communicated quickly. Utilizing a social media platform versus an internet-based platform has increased participation within the VJC. Thus this practice change has been deemed successful, and continues to be maintained by the Nursing Research Council.
-

The benefits of fasting for patients who are immunocompromised and undergoing cancer treatment: An integrative research review
Lori Burnett
Background: In the past several decades, remarkable advances in the treatment of cancer have been made. However, a gap remains regarding best practice strategies to reduce the amount of short and long-term side effects and adverse or emergent events related to cancer treatment that may negatively impact patient quality of life. Recent evidence suggests that if patients undergoing cancer treatment fast for a period of time, they may experience reduced chemotherapy-related side effects and enhanced immune potential. Weight loss and malnutrition associated with cancer treatments highlight the importance of evidence appraisal associated with fasting prior to recommending this practice as part of an individualized cancer treatment plan.
Purpose: This review aimed to answer the clinical question: Among patients receiving active cancer treatment, does fasting enhance the immune system, increase efficacy of cancer treatment, and decrease chemotherapy-related side effects?
Methods: This review was created using Whittemore's Methodology of Integrated Research Reviews. A search of the articles using Cochran Library, PubMed, Medline, CINHAL, and Health Source: Nursing/Academic Edition was conducted. The key words used to perform the search were: "fasting" AND "immune system" AND "chemotherapy". Search criteria were limited to "free full text articles" between 2015 and 2020 except for PubMed. A total of sixteen articles resulted for review with ten more identified through bibliographic mining. All articles were critically appraised for level and strength of evidence using an evaluative checklist and the EBR (evidence-based readiness) tool.
Results: From the twenty-six unique articles identified, twelve were considered to be appropriate for the scope of this project. Of these twelve articles, two were rated to be level one, one as level two, three as level three, one as level four, and five as level five. All articles used to inform answering the clinical question reported a positive correlation with fasting and the efficacy of chemotherapy agents as well as an enhanced immune system. “Fasting” definitions varied across reviewed literature.
Conclusion: The current integrative literature review suggested that fasting may have a beneficial effect on the immune system and may mitigate adverse side effects associated with chemotherapy. Additionally, some evidence supported that among patients who fasted compared to those who did not, tumor growth was clinically decreased. While this combination of studies offered positive findings, more high-quality clinical research is needed to determine the benefits and potential harms of fasting among patients receiving active cancer treatment. Furthermore, research needs to indicate a clear definition of fasting, including optimal timing and type, before this practice can be effectively recommended in the clinical setting.
-

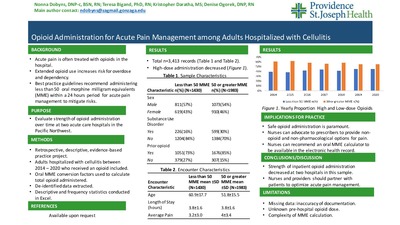
Pain Management Trends among Adults Hospitalized with Cellulitis: An Evidence-based Practice Project
Nonna Dobyns, Teresa Bigand, Kristopher Darath, and Denise Ogorek
Background: Cellulitis is an acute infection of the skin resulting in acute pain and often requires pharmacological analgesics. Past studies revealed that more than half of patients receiving inpatient medical care in the United States received opioid analgesics for pain management during the hospital stay. While opioids are regarded as the strongest analgesic available to ease physical pain, these are habit-forming drugs that contribute to negative outcomes such as opioid use disorder and increased risk for accidental overdose and death. Recommendations for acute pain management in the hospital setting include prescribing less than 50 morphine milligram equivalents (MME's) per day to avoid negative outcomes. Although it is known that opioids should be administered at low doses to treat acute physical pain in the hospital, it is unclear how opioid administration practices have evolved over time to align with best practices in two acute care hospitals in the Pacific Northwest.
Purpose/aims: Our purpose was to evaluate how inpatient opioid administration evolved between the years 2014 and 2020 in two acute care hospitals for a model population with acute pain: adults with cellulitis.
Methods/Approach: Retrospective, de-identified data were extracted from the electronic health records for adults with a primary diagnosis of cellulitis. Records included in the analysis reflected patients age 18 years and older, hospitalized with cellulitis for at least 24 hours but no more than 7 days, treated at one of two hospitals in the Pacific Northwest between the years 2014 and 2020, and administration of an opioid medication during the encounter. Data were analyzed in Excel using descriptive and frequency statistics.
Results: A total of 3,413 inpatient records were included in the analysis. In this sample, adults who received high-dose opioids during the hospital stay were younger, more likely to have a documented substance use disorder, more likely to report taking an opioid within 30 days of the hospital encounter, and reported more pain than those who received low-dose opioids. The proportion of adults receiving high-dose opioids during the hospital stay for cellulitis decreased over time from 61% to 55%.
Conclusion: This project supports that opioid administration has evolved over time to align with best practice guidelines for alleviating acute pain. Future work is needed to further characterize what factors influence the strength of opioids administered in the hospital to manage acutely painful conditions such as cellulitis.
Implications for practice: Safe opioid prescribing is paramount to ensure effective short and long-term patient outcomes. It is important for nurses to advocate to prescribers to ensure all appropriate non-opioid analgesics and non-pharmacological pain management techniques are available to ease patient suffering as well as reduce high-dose opioid administration to avoid potential patient harms.
-

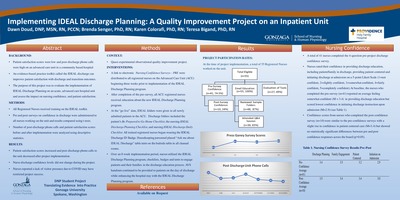
Implementing IDEAL Discharge Planning: A Quality Improvement Project on an Inpatient Unit
Dawn Doud, Brenda Senger, Karen Colorafi, and Teresa Bigand
Background: Effective discharge teaching reduces 30-day hospital readmissions, decreases unnecessary emergency room visits, improves patient satisfaction, and is cost effective for hospitals by improving the Centers for Medicare and Medicaid Services (CMS) measures for reimbursement. Evidence suggests that standardized discharge teaching templates embedded within the electronic health records lack patient engagement and can fail to meet individual patient discharge education needs. A need was identified to improve the discharge planning process on an advanced care unit in a community based hospital.
Purpose: The purpose of this project was to evaluate and assess the implementation of an evidence based toolkit, IDEAL Discharge Planning, on an acute, advanced care hospital unit.
Methods: This quality improvement project included surveys that were electronically sent to measure both nursing confidence and nursing perception of the IDEAL tool kit effectiveness. Nursing Confidence Survey scores including brief demographic data (years as an RN, nursing education level, and current FTE position) were collected using an automated response tool (REDCap)both before the implementation of the toolkit and after. Over an 8-week implementation period, nurses utilized the IDEAL Discharge Planning program to engage patients and their families in the discharge education process. Standard of care “after visit summary”(AVS) handouts continued to be provided to patients on the day of discharge although these were enhanced by the IDEAL Discharge Planning program. The number of patient phone calls to the unit were tallied and compared 3 months pre and post-intervention. Patient satisfaction scores, specifically Press Ganey -Patient Discharge Care at Home were collected as a quarterly measure before and after the intervention. Nurses' perceptions of the use and effectiveness of the IDEAL checklists, badge cards, and table tents was collected from the Evaluation of IDEAL Tool Survey using REDCap. Likert-scaled and open-ended responses were collected.
Results: A total of 55 registered nurses received education on the IDEAL Discharge Planning toolkit. Of these, 27 provided feedback on the use of the tools and 10 provided pre and post confidence scores. Statistical analysis demonstrated no change in nursing confidence pre and post implementation. Post discharge phone calls to the unit significantly decreased and patient satisfaction scores significantly increased during the post implementation time frame. Nurses reported low frequency of tool usage primarily related to COVID-19 pandemic.
Conclusion: Evidence demonstrates that effective discharge education requires engagement with the patient and family during the patient's entire hospital stay. Nurses reported barriers from visitor restrictions that negatively impacted implementation of the IDEAL Discharge Planning toolkit.
Implications for practice: This quality improvement project demonstrated some positive impacts on patient satisfaction and should be re-trialed when the visitor restrictions from COVID-19 have been removed
-

Reducing Hospital Acquired Pressure Injuries on an Advanced Care Unit
Dawn Doud and Lynn Stapleton
BACKGROUND: Hospital-acquired pressure injuries (HAPIs) are increasing nationwide. HAPIs are a negative outcome of hospitalization and these conditions are not eligible for reimbursement, resulting in billions of dollars of healthcare costs to hospitals. HAPI rates were noted to climb on an advanced care unit in a community-based hospital in the Pacific Northwest. In order to reduce this patient harm event, the nurse manager partnered with the nursing professional development specialist to lead a HAPI prevention quality improvement plan.
PURPOSE: To decrease HAPI rates on the Advanced Care Unit.
METHODS: The nurse manager conducted a deep dive on all HAPI events on the unit and identified a wide variance of scores assigned using the evidence-based practice tool for assessing risk for skin breakdown: the Braden Scale. The nurse manager required all nurses who were involved in the care of patients who developed a HAPI in 2020 to complete a facility-specific HAPI investigation tool. Each nurse was responsible to meet one on one with the manager to review the information together. Next, all nurses working on the advanced care unit were administered a survey containing two standardized patient cases and were required to assign a Braden score based on each case. Nurses then completed an educational module detailing best practice on assessing skin breakdown risk and appropriate nursing interventions for preventing injury. In addition, nurses were required to complete a two-RN skin check utilizing a half-sheet paper tool passed on from nurse to nurse on all patients newly admitted or transferred to the unit and to conduct a 2-RN skin assessment during each shift report on patients with a Braden less than 18 or receiving any supplemental oxygen. Finally, three months after the interventions, nurses repeated the cases studies and assigned appropriate Braden scores. The nurse manager monitored for changes to unit HAPI rates as well as improvement in nursing accuracy for assigning the Braden score.
RESULTS: After implementation of the nursing education, the unit HAPI rate reduced to zero. The unit has sustained this rate for one year. In addition, nursing ability to assign appropriate Braden scores greatly improved. Results from case studies and quality outcomes were shared with staff.
CONCLUSIONS: Best practice interventions can greatly improve nursing ability to identify patients who are high-risk for pressure-related skin injury and appropriately intervene. Ensuring that nurses have proper training and confidence to assign an appropriate Braden score and implement corresponding clinical actions may be a first step to reducing patient harm related to HAPI's.
IMPLICATIONS FOR PRACTICE: Clinical nurses may benefit from receiving educational in-services on prevention of HAPI's. In addition, active support from nursing leadership and professional development specialists to enhance routine surveillance of skin health may assist with sustaining positive change in the acute care nursing setting.
-

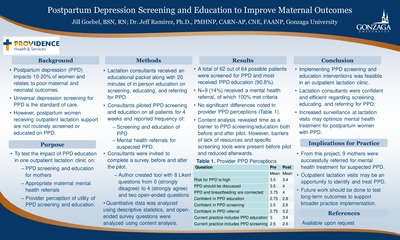
Postpartum Depression Screening to Improve Maternal Outcomes
Jill Goebel and Jeff Ramirez
Background: Postpartum depression (PPD) is correlated with worsened maternal and infant health outcomes, and an estimated10-20% of women experience this condition after giving birth. Universal depression screening for PPD in maternity and well-child appointments is the standard of care. However, PPD screening is not well-integrated into outpatient lactation visits which assist new moms with difficulties breastfeeding. To address this gap, routine PPD screening and education was implemented in an outpatient lactation clinic servicing postpartum women in Eastern Washington. Purpose: The purpose of this quality improvement project was to implement the use of PPD screening in a lactation clinic to increase appropriate maternal mental health referrals and enhance provider perception of the clinical need for PPD education in the lactation clinic setting. Methods: Lactation consultants working at a single outpatient clinic servicing postpartum women in Eastern Washington were invited via email to complete a pre-intervention survey on knowledge and confidence in screening and intervening for PPD symptoms in early 2021. Consultants then attended a training session offering information on how to screen for, provide education about, and appropriately refer patients for suspected PPD. The lactation consultants were then requested to incorporate a PPD screen on every patient receiving care in the clinic for a four-week period and to track on a sheet of paper the number of patients: presenting for an appointment, receiving PPD screen, receiving education on PPD, and receiving a referral for potential PPD. At the end of the four-week intervention, consultants were invited to repeat the initial survey. Data was collected and analyzed using descriptive statistics to quantify the providers’ perceptions of PPD before and after the intervention. Open-ended survey items were analyzed using content analysis. Results: 62 of 64 patients were screened during the data collection period meaning 96.9% of patients who attended the lactation clinic received screening for PPD. 90.6% of patients received PPD education, and 100% of patients who were screened were referred correctly for PPD. 14% of patients who were screened received a referral. There were no statistically significant differences in the pre and post-test in the perception of the lactation consultants. Content analysis revealed barriers to PPD screening and education were reduced following the training session, but lack of time was still seen as a barrier.
Conclusion: Incorporating PPD screening and education into the standard of care provided at lactation consultations is another avenue to offer women resources and support needed to cope with symptoms of PPD. In addition, the integration and normalization of this conversation during lactation visits may help reduce the negative stigma surrounding mental health conditions for vulnerable populations such as new mothers. Implications for Practice: This quality improvement project shows that lactation consultants can incorporate PPD screening and education into their practice to improve maternal care. Findings from this project may justify a permanent change to workflow in this clinic to continue routine PPD screening and educating. Future work should be done to advocate for similar lactation clinics to consider adopting this practice as well. -

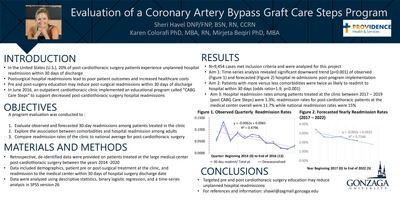
Evaluation of a Coronary Artery Bypass Graft Care Steps Program
Sheri Havel, Karen Colorafi, and Mirjeta Beqiri
Background: Across the U.S., 20% of cardiothoracic surgery patients who are discharged to home experience unplanned readmission within 30 days of discharge. Readmissions and postsurgical complications are associated with poor patient outcomes, increased mortality rates, and increased cost of healthcare. Evidence-based recommendations for reducing preventable readmission are limited, although there is some indication that high quality pre-operative and discharge education can reduce this burden. Providing appropriate patient education at time of discharge from acute care to home regarding medication adherence, prescheduled follow-up appointments, wound management and monitoring, and symptom management education is theorized to have a significant positive impact on patient outcomes.
Purpose/aims: The primary purpose of this program evaluation was to evaluate 30-day readmission rates at a large medical center in the Pacific Northwest prior to, during, and after the implementation of a comprehensive program of patient education designed to support patients undergoing elective cardiothoracic surgery at an outpatient cardiothoracic clinic staffed by cardiothoracic surgeons who performed operations at the medical center.
Methods/Approach: This program evaluation used an observational design. The retrospective analysis of a de-identified dataset included 9,454 patients (18-100 years of age) who underwent a cardiothoracic procedure (coronary artery bypass graft, valve replacement, valve repair, wedge resection, or lobectomy) with providers at the outpatient clinic between 2014 and 2020. The dataset included the following variables of interest: age, gender, BMI, race, ASA score (representing comorbidity), surgery type, length of surgery, marker of 30-day readmission, days since surgery, and occurrence of 30-day readmission as the dependent variable. Data were explored descriptively to assess variability and normalcy before performing a time series analysis to evaluate trends in readmission rates.
Results: There was a statistically significant (p=<0.001) 6% decrease between average readmissions prior to and post program implementation. Patients with comorbidities are twice as likely to experience readmission than those with a low co-morbidity index [1.9 (1, .074), p =<.001]. Hospital readmission rates fall below the national average at 13.8% vs. 15.2% overall and 11.7% vs. 14.9% for CABG.
Conclusion: The time series analysis represents the highest level of observational evidence available, and in this case, suggests that a decrease in readmissions is associated with the implementation of a comprehensive patient education program by the outpatient clinic. The results of this evaluation contribute to the small body of evidence currently available regarding methods to reduce unplanned readmission rates among surgical patients and may be helpful to other surgical clinics who wish to improve their preventable 30-day readmission rates.
Implications for practice: High quality, patient-centered nursing care is essential to meeting national healthcare goals related to patients post-surgery. The implementation of a comprehensive educational program at one cardiothoracic clinic appears to be helping patients avoid unnecessary hospital readmissions following open heart surgery.
-

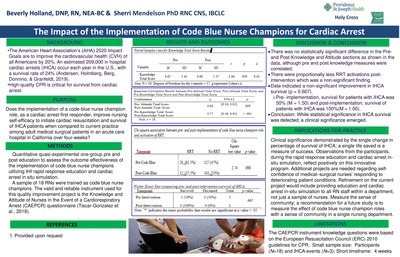
The Impact of the Implementation of Code-Blue Nurse Champions for Cardiac Arrest
Beverly Holland and Sherri Mendelson
Background: Delayed recognition of in-hospital cardiac arrest (IHCA) events can affect survival rates. At the project site, there was a failure to rescue in the medical-surgical population. Key elements of success include staff identifying at-risk patients combined with early interventions to prevent deterioration of cardiac arrest. Survival and favorable outcomes for IHCA (i.e., neurological sequelae) were shown to be highly dependent on several factors, such as a skilled resuscitation team, prompt initiation of cardiopulmonary resuscitation and defibrillation, and organizational structures to support resuscitation care; therefore, nurses are an integral part of an IHCA response.
Purpose / Aims: The purpose of this quantitative quasi-experimental quality improvement project was to determine if the implementation of Banks and Trull's code blue nurse champion role (CBNCR) would impact the nurses' knowledge and self-efficacy regarding cardiopulmonary resuscitation and patient IHCA survival rates at an acute care hospital in Southern California over four weeks. Bandura's self efficacy theory and the trans-theoretical model were theoretical underpinnings of the project.
Methods / Approach: A quantitative methodology was selected for this project to discover through statistical analysis, quantifiable, objective data related to the implementation of CBNCR on nurses' self efficacy to respond to cardiac arrest and survival of patients suffering IHCA before and after the intervention. The training for the CBNCR included IHI rapid response education and in-situ simulation on cardiac arrest scenarios. Results: Data on nurses' (N=18) cardiac arrest knowledge and self-efficacy were evaluated using the Knowledge and Attitude of Nurses in the Event of a Cardiopulmonary Arrest instrument. A paired t-test showed no statistically significant improvement in nurses' knowledge (p=.959) and self-efficacy (p=.910). The total patient population was 302, n=147 in the comparative (n=2 IHCA) and n=155 (n=1 IHCA). To analyze IHCA, a Fischer's exact test was used, which was not statistically significant (p=.667) (pre n=2, 50%; post n=1, 100%).
Discussion: Results indicated the CBNCRs may not improve nurses' knowledge and self-efficacy or IHCA rates. Although not statistically significant, clinical significance was demonstrated as the CBNCRs provided skills to improve early recognition of impending IHCA and enhanced nursing staff's awareness of patient's deterioration.
Conclusion: Simulation offers acute care nurses an opportunity to practice life-saving techniques in the clinical setting without patient harm. Simulation as a safety strategy focuses on developing positive attributes and productive capacities that underpin safety performance. Implementing dedicated nurse champions is a novel approach to improve recognition and response to deteriorating patients. Providing additional hands-on experience through cardiac arrest in-situ simulation could equip them to provide timely and effective CPR during cardiac arrest.
Implications for practice: The results provide insight into the innovative role of code blue nurse champions. Implementation of the CBNCR is predicated on providing educational training to a core group of medical-surgical nurses on rapid response roles, how to activate RRT, development of SBAR communication, and in-situ simulation on cardiac arrest. The recommendation for practice is to replicate and implement nurse CBNCRs throughout the medical-surgical units. Creating a hospital-wide CBNCR position may decrease nurses' anxiety, while increasing self-confidence and self-efficacy in recognizing patient deterioration and early initiation of CPR.
-

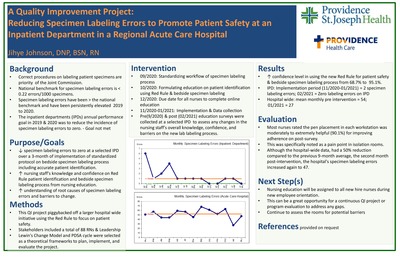
Reducing Specimen Labeling Errors to Promote Patient Safety: A Quality Improvement Project at an Inpatient Department in a Regional Acute Care Hospital
Jihye Johnson
Background: Mislabeled specimen can cause patient harm by delaying treatment or by inappropriately administering treatment based on incorrectly assigned results. National patient safety goals have consistently called for a reduction of these errors in the hospital setting to zero. The specimen labeling errors on one inpatient department (IPD) at an acute care hospital in Eastern Washington were noted to be elevated from 2019 to 2020, potentially threatening patient safety. An evidence-based technique called the Red Rule has been linked to an improvement in lab labeling performance in the hospital setting.
Purpose/aims: The primary purpose of the QI project was to reduce specimen labeling errors in the identified IPD. The clinical question was, "In an IPD at a large acute care hospital, does implementing a standardized specimen labeling workflow, nursing education on the Red Rule, and updating monthly performance data with nursing staff, compared to usual care, reduce the occurrence rate of specimen labeling errors over 3-month period of implementation?"
Methods/Approach: The project lead collaborated with the Red Rule Advisory Committee to implement a Doctor of Nursing Practice (DNP) project focusing on the selected IPD. Interventions and data collection consisted of the following: (1) Standardizing workflow of specimen labeling process by the end of September 2020, (2) Formulating nursing education on the Red Rule by the end of October 2020, (3) Assigning nursing education to all RNs through an online learning platform to complete by the end of December 2020, (4) Sharing monthly data on specimen labeling errors from November 2020 to January 2021, and (5) Administering Pre- and post-interventions surveys in September 2020 and in February 2021 respectively to assess nursing staff perspectives on the new lab labeling process. Descriptive statistics was used for data analysis.
Results: A total of 32 nurses took the pre-intervention survey and indicated a low level of awareness and confidence on using the new Red Rule and lab labeling process. The biggest barrier on the new labeling compliance was lack of a pen in each patient room. A total of 41 nurses completed postintervention survey and reported increased confidence in using Red Rule and applying the new labeling process. Furthermore, the majority of nurses rated the pen placement in each workstation as moderately to extremely helpful for improving adherence. Following the intervention, the incidence of lab mislabeling errors on the IPD reduced significantly.
Conclusion: On the IPD, the implementation of an evidence-based Red Rule program was effective in reducing specimen labeling errors. The identification of the nursing-reported need for a pen in each patient room in order to effectively implement the new labeling process was a surprisingly simple yet powerful gap that was easily filled by this project.
Implications for practice: This project highlights the importance of assessing nursing perspectives on barriers to implementing change and supports that the Red Rule may be helpful in reducing lab labeling errors. Opportunities exist for future work to address gaps in following the new lab labeling process.
-

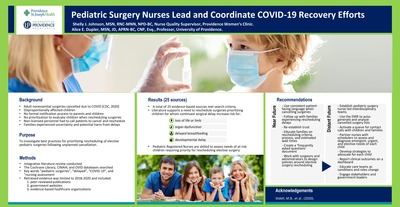
Pediatric Surgery Nurses Lead and Coordinate COVID-19 Recovery Efforts
Shelly Johnson and Alice E. Dupler
Background: In early 2020, the appearance of the novel COVID-19 virus became a global concern, infecting hundreds of thousands of people. To reduce the spread of the virus, the United States government instituted social distancing and required hospitals to take steps to create extra beds for patient with COVID. One method to increase hospital capacity was the cancellation of scheduled, elective surgeries. In one large pediatric hospital in the Pacific Northwest, there was no formal process in place for cancelling elective procedures or for prioritizing when or how to reschedule the case. Because nurses were being called on to provide direct patient care with increased volumes during the pandemic, non-licensed surgery schedulers were tasked with calling patients to cancel cases without ability to assess patient conditions or provide guidance on when the case might be rescheduled. As a consequence, children and their families who were impacted by cancellations experienced uncertainty and fear that, if left untreated and unevaluated, the underlying condition might worsen and lead to an emergency situation. Nurses in this pediatric surgery center therefore conducted a deep dive into the literature to identify best practices to inform when and how to resume elective surgeries in this vulnerable population.
Purpose/aims: To investigate the role of pediatric nurses following unexpected surgery cancellation for at-risk children.
Methods/Approach: An integrative literature review was conducted. The Cochrane Library, the Cumulative Index of Nursing and Allied Health Literature (CINAHL), and OVID databases were searched using the key words “pediatric surgeries”, “delayed”, “COVID-19”, and “nursing assessment”. Retrieved evidence was limited to peer-reviewed publications, government websites and reputable healthcare organizations published between January 2018 and September 2020. Results: A total of 25 articles and government-sponsored websites met search criteria. Evidence supported that the following criteria merit high priority for rescheduling surgeries for patients: risk for loss of life, limb, organ function, delayed breastfeeding, and developmental delay. Furthermore, nurses are uniquely trained to prevent illness, facilitate healing, and alleviate suffering, and are recommended to assess ongoing individualized care needs that could drive prioritization of surgery rescheduling following unexpected cancellation.
Conclusion: In pediatric patients awaiting non-emergent, elective surgery during the COVID-19 pandemic, literature supports that pediatric surgery nurses must provide ongoing assessment and care of each child affected by cancellation of an elective surgery. Appropriate and timely assessment of evolving family and child needs related to the cancelled surgery can reduce the likelihood of harm during the pre- and post-operative periods.
Implications for practice: Pediatric surgery nurses are uniquely positioned to minimize the impact of cancelled elective surgeries by advocating for rescheduling procedures based on assessment of evolving pediatric patients’ need for care. Moving forward, pediatric surgery nurses should collaborate with interdisciplinary teams to write specific institutional policies to guide decisions regarding how and when to resume and prioritize pediatric surgeries if elective procedures need to be delayed.
-

COVID in our backyard: The lived experiences of RN to BSN students facing a pandemic
Shelly Johnson, Alice E. Dupler, and Deanna J. Koepke
Background: Relationships exist between improved patient outcomes and Registered Nurse (RN) caregivers with an earned Bachelor’s degree or higher compared to those with an associate’s or diploma in nursing. However, nurses who are working and attending a bridge program to obtain a Bachelor of Science in Nursing (BSN) report high levels of stress which may increase risk for withdrawing from the program or quitting work. Furthermore, providing direct patient care during the COVID-19 pandemic may significantly increase stress among those who are concurrently finishing a nursing advanced degree. Little is known about how front-line caregivers perceive the experience of working at least three days per week during a pandemic such as COVID while also completing a full-time RN-BSN program.
Purpose/aims: To explore the lived experience of final-semester RN-BSN students working at least 0.6 full-time-equivalent in the healthcare setting during a global pandemic. Methods/Approach: A qualitative study using thematic content analysis was conducted to explore perceptions of working and going to school during the COVID-19 pandemic among graduating RN to BSN students working between 0.6-1.0 FTE concurrently during the program. Two weeks prior to graduation from the program, students from one cohort were required to write and submit a reflection with the following prompt, “Tell your story about working and going to school during the COVID-19 pandemic”. Analysis of the narratives was undertaken with automated content and thematic analysis by Leximancer software, an automated textual analysis technology, to identify and characterize emerging themes and concepts described in the narratives. The software produces a visual representation of the frequency of concepts reported in qualitative data, and draws lines to demonstrate how often certain terms are used in conjunction with others. The study received IRB approval from the primary investigator’s institution.
Results: A total of 42 students were part of the cohort and 35 submitted a reflection. All 35 were analyzed by the software with names and identifiers were removed. Based on the qualitative software output and validation of generated themes by two independent nurse scholars, three separate concepts arose: COVID-19, time, and family. Many students reported COVID being a major disruptor to all aspects of life during their experience in the program. For instance one student said, “It is like, sucking the life out of me.”
Conclusion: Participants in the study made distinctions between COVID-19, time and family in written assignments discussing their lived experiences of working and going to school during the pandemic. For our participants, work and social environments may play an important role in stress levels for working RN-BSN students which is intensified in the context of the pandemic.
Implications for Practice: College and healthcare leaders should partner to support the RN to BSN workforce to reduce stress and optimize individual capacity to provide effective care to patients and family. Nurses who are working full-time during the current pandemic should carefully consider the pros and cons to returning to school and create a plan for self-care to enhance success and maintain a worklife balance.
-

How Much is too Much: Examining Fluid Responsiveness in Septic Patients
Natalie Kitago, Lak Tuong, and Sarah Rosenberg
Background & Significance: The leading cause of death of critically ill patients is sepsis. The CDC reports that sepsis is estimated to be responsible for 1 of every 3-hospital deaths. Furthermore, in hospitals located in California for one large hospital system, a reported30.74% patients admitted to the ICU with sepsis died in the year 2017.
Purpose: The purpose of the study was to determine if utilizing non-invasive pulse contour technology (PCT) is a feasible intervention to manage fluid responsiveness and resuscitation specifically with septic patients in a community Intensive Care Unit in California. A secondary aim was to determine if use of PCT and a nurse-driven algorithm for fluid resuscitation could improve patient outcomes with respect to mortality rate, ICU length of stay in days, and ICU ventilator use days.
Methods: A single-cohort feasibility study with 50 participants was conducted. Subjects were admitted to ICU directly from the Emergency Department with primary diagnosis of sepsis/septic shock, and enrolled within 24 hours of admission. Subjects had the Pulse Contour Technology applied, remaining in place for 72 hours or until discharge from ICU. A nurse driven algorithm was utilized to determine when the patient was to be given IV fluids verses starting vasopressors based on fluid responsiveness. Retrospective and prospective data was collected using specific inclusion and exclusion criteria. A certified statistician consulting with our hospital analyzed all data using standard SPSS software.
Results: Out of the 50 patients enrolled in the prospective study the algorithm was applied 92.3% of the time. This indicates that a nursing driven protocol for fluid management is feasible in the community hospital ICU setting. We found that the PCT did guide fluid resuscitation. When comparing the prospective data to the retrospective data we found that mortality decreased from 31% to 22%, ventilation days decreased from 5.3 to 1.3, and length of stay decreased from 6.4 to 3.2 days. Finally, we assessed the prospective data, finding that 62% of patients were considered fluid overloaded per definition. There was no statistical significance between fluid overload and procedures performed.
Conclusion: Utilizing PCT and algorithm to guide fluid management in sepsis patients to determine if a patient needs vasopressors verses fluids demonstrated positive outcomes. Going further it can assist in bed selection from ER, or RRT; identifying if septic patient requires ICU for vasopressor therapy or step down unit for further fluid resuscitation. It would be beneficial to conduct a larger scale study to determine if the results translate beyond our community hospital setting.
-

Team Up Against Sepsis: Six Tasks in Sixty Minutes
Karin Kloppel and Barbara Richards
Background: Sepsis is the number one cause of mortality in hospitals nationwide. Our hospital system has identified sepsis mortality reduction as a top priority. Early recognition and treatment through improving sepsis bundle compliance was the selected focus in a 40-bed Emergency Department (ED) a community-based hospital.
Purpose: To evaluate the impact of a team response to sepsis alerts on sepsis outcomes in the ED in an acute care hospital.
Methods: Prior to implementing a team approach to sepsis alerts, ED staff were surveyed to describe awareness of SIRS and sepsis criteria and of sepsis bundle intervention metrics. Challenges identified were obtaining IV access, labs, 2 blood cultures, initiating IV fluid resuscitation and administering antibiotics in a timely manner. As a result, this quality improvement team created a team sepsis response, where two RNs respond to a room when a sepsis alert is called to "Team Up Against Sepsis". Together, the pair completes the following six evidence-based practice tasks within sixty minutes of the sepsis alert: 1) Blood collection: CBC, CMP, PT/INR, Procalcitonin, and Blood cultures x 2; 2) Lactate collected and placed on ice; 3) Urine collection; 4) Fluid resuscitation at 30 ml/kg; 5) Oxygen status is monitored/maximized; 6) Administer ordered antibiotic, if applicable. The pair will divvy up these six tasks including documentation to drive faster sepsis diagnosis and treatment. The quality improvement team educated nursing staff on using the new sepsis team response to every sepsis alert in the ED and also placed a card of the six sepsis tasks on all ED computers as a visual reminder of the project. Results: Pre-implementation was in the middle of the year 2019, and at that time, on average, the time from sepsis orders to antibiotic was 141.5 minutes; sepsis alert called to antibiotic administered was 221 minutes; blood culture order to collection was 53.32 minutes; IV fluids order to administration was 67.70 minutes. Post-implementation data was measured for the beginning of the year 2020 and all times decreased: Sepsis orders to antibiotic was 51 minutes on average; alert called to antibiotic was 79 minutes; blood culture order to collection was 59 minutes, and IV Fluids order to administration was 59 minutes. Last, there was a decrease in observed versus expected sepsis-related mortality from 1.15 at the beginning of the project to 0.66 at the post-implementation time point.
Conclusion: Teaming Up Against Sepsis had a positive impact in improving identification and treatment of sepsis in the ED with a significant reduction in observed versus expected sepsis related mortality rates. The team approach to sepsis alerts has been adopted as a best practice in this ED. Next steps include implementation of this approach at other ED’s within this hospital system and continual evaluation of sepsis outcomes.
-

Improving Primary Care Screening for Familial Hypercholesterolemia
Mary Nametka and Brenda Senger
Background: Familial Hypercholesterolemia (FH) is the most common genetic condition resulting in cardiovascular disease, a leading cause of death in the United States. FH is estimated to affect 1 in 250 individuals with elevated lipid levels present from birth. An estimated 90% of individuals with FH remain undiagnosed. '
Purpose: The purpose of this quality improvement project was to increase provider awareness and promote screening for FH among adults ages 20 years and older. '
Methods: This quality improvement project consisted of an online educational intervention for providers working at an outpatient clinic regarding FH. Outcomes included: 1) pre-intervention lipid screening practices at the point of admission and every five years; 2) pre-intervention treatment status for clients exceeding the LDL-C 190 mg/dl cut-point; and 3) post-intervention lipid screening practice changes. Assessment of providers' FH knowledge occurred with author created surveys, and a retrospective chart review provided information on documentation of lipid screening practices as well as the proportion of patients screened for FH before and after the educational intervention.
Results: Outcome measures of FH knowledge were reported using descriptive statistics. An independent samples t-test showed no statistically significant change in screening practices pre/post-intervention (p = 0.976), with a mean interval of 2.09 years between initial and subsequent testing. Regression analysis yielded a medium correlation effect between age and lipid testing intervals, decreasing by .028 years for every one-year increase in age. The proportion of clinic patients exceeding the expected population estimate for FH was significant (p<.001). Return of clinical impact survey data did not occur.
Conclusions: Electronic Medical Record data identified undiagnosed patients in the clinic population at risk for FH. Knowledge surveys identified themes for further provider FH education.
-

The effect of COVID-related changes in diet, exercise, sleep patterns, and mood on stress levels of RNs who work 12-hour shifts during the pandemic
Amber Norman, Trisha Saul, Ross Bindler, and Teresa Bigand
Background: Registered Nurses (RNs) working 12-hour shifts are regularly exposed to high stress situations which has intensified during the COVID-19 pandemic. Chronic stress exposure may lead to changes in health habits and impact sleep, exercise or diet, augmenting risk for adverse health outcomes and taking a negative emotional toll. While nursing staff educate patients on reducing stress and engaging in health promotion behaviors, there is little research on perceived stress and relationships to COVID-related changes in sleep, diet, exercise, and mood of nurses working full-time, 12-hour shifts during the pandemic.
Purpose: The purpose of this pilot study was to gain preliminary insight on perceived impacts of the COVID-19 pandemic on exercise, sleep, diet, mood, and stress in 12-hour shift RNs.
Methods/Approach: This observational descriptive study was composed of 12-hour shift RNs in the Western United States. This is an ongoing pilot study with the end goal of 60 participants. RNs completed surveys providing self-reported information on demographics, stress, and emotional and behavioral changes perceived in relation to the COVID-19 pandemic. Stress was measured with the valid and reliable Perceived Stress Scale short form, and author-created Likert scale questions evaluated whether diet quality, sleep quantity, sleep quality, exercise, stress, sadness, or anxiety worsened, remained unchanged, or improved since the onset of the COVID-19 pandemic. Data were analyzed using descriptive and frequency statistics as well as independent samples t-tests in SPSS version 26.
Results: At the time of preliminary analysis, 40 participants provided data on the variables of interest. Of these participants, there were no observed significant differences among self-reported stress levels when comparing: shift worked (night versus day); COVID-related exercise, sleep, anxiety, or stress changes; age; or gender. One significant preliminary finding was that RNs who reported worsening dietary habits related to COVID tended to have increased stress levels (p=0.005). Another finding was that higher levels of stress were reported among nurses with greater-perceived personal sadness related to the COVID pandemic (p=0.003).
Conclusion: RNs are called to help others yet may be at risk for high stress and poor health outcomes, especially in the context of working during the COVID pandemic. These preliminary data suggest trends in relationships between stress and self-reported COVID-related changes to dietary habits as well as personal sadness among RNs.
Implication to Practice: Nurses are front-line caregivers and optimal physical and emotional health is critical to delivering effective patient care. While this small pilot study is ongoing and acknowledges that these are preliminary findings, it is suggested that working full time, 12-hour shifts in the hospital setting during the pandemic may have an impact on stress of RNs which could negatively influence well-being.Future studies may benefit from more directly exploring relationships between diet, mood, and stress levels over time in this population.
See agenda for the June 14, 2021: Providence Nurses Supporting Health for a Better World here
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
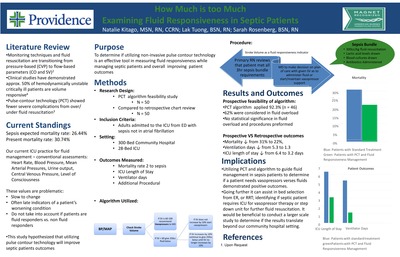{kind=link}
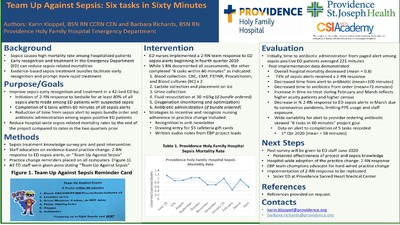{kind=link}
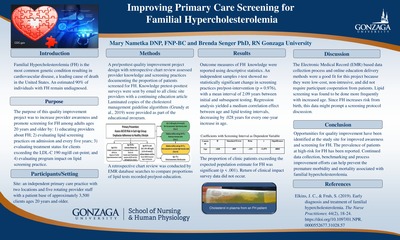{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
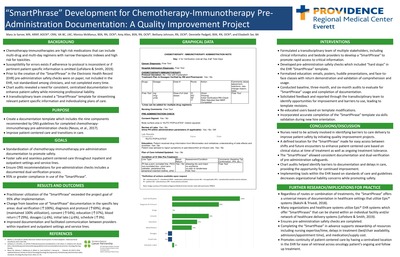{kind=link}
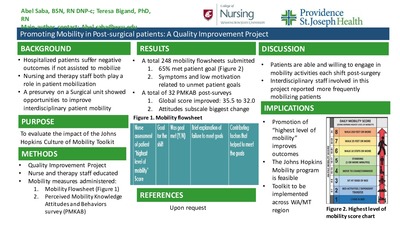{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
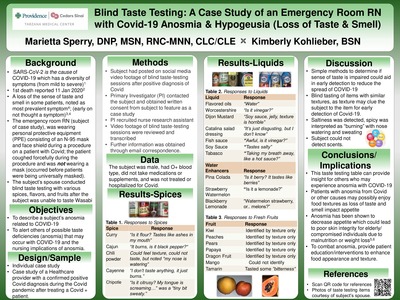{kind=link}
{kind=link}