
-

Effectiveness of Apfel Simplified Risk Score in Predicting Postoperative Nausea and Vomiting in Day Surgery Unit
Leni Alejo, Cherry de Guia, Cynthia Rodriguez, and Cassandra Luck-Bird
Background: Postoperative nausea and vomiting (PONV) continues to be a perioperative complication despite improvement in quality and safety of anesthesia care causing an increased overall healthcare cost and sometimes serious physical complications. The American Society of PeriAnesthesia Nurses (ASPAN) supports that risk assessment for PONV helps with its prevention which is in line with the Society of Ambulatory Anesthesia's (SAMBA) current guidelines for PONV management. Literature supports that PONV can be predicted and prevented in patients by assessing risk factors such as gender, smoking status, history of PONV and use of postoperative opioids, among others. At present there is no formal PONV risk assessment tool that will help the perioperative team prevent this unpleasant complication from surgery.
Purpose: The purpose of the study is to determine the effectiveness of APFEL Simplified Risk Score (SRS) in predicting PONV and apply this tool to help prevent PONV in patients undergoing surgery.
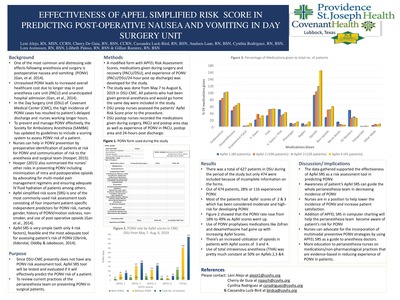
Methods: A group of nurses conducted a quality improvement study in the adult day surgery unit of a tertiary hospital in northwestern Texas was done from May 7, 2019 to August 2, 2019. The APFEL SRS (a PONV risk assessment tool) was used in the study because of its practicality and literature-supported effectiveness. A form was devised consisting of patient's APFEL SRS score from 0-4 (0 = no PONV risk, 1 = low PONV risk, 2 = moderate PONV risk and 3-4 = high PONV risk). A list of medications received before, during and after surgery including anesthesia, pain medicines and antiemetics and record of PONV experience after surgery and 24 hours post discharge was also collected. APFEL SRS scores were compared to the likelihood of developing PONV.
Results: A total of 474 patients who received general anesthesia and discharged the same day was included in the study. 17% of patients had an APFEL SRS of 1, 40% with APFEL SRS of 2, 34% with APFEL SRS of 3 and 9% with APFEL SRS of 4. The patients' experience of PONV increased as their risk scores went up. Data showed 18% PONV experience in patients with APFEL SRS of 1, 17% in APFELSRS of 2, 30% in APFEL SRS of 3 and 49% in APFEL SRS of 4. The results showed that the use of prophylaxis drugs for PONV did not correlate with APFEL SRS scores. It was noted that patients with higher APFEL SRS scores also received more narcotics.
Conclusion: The use of APFEL SRS is effective in predicting PONV and awareness of the patient's PONV risk will help the perioperative team prevent and manage its care.
Implications for practice: Since nurses are in position to assess the PONV risk of the patients, adapting APFEL SRS tool will ease the communication of the risk to the anesthesia and surgical team. Awareness of the patient's risk will help doctors do their part in preventing and treating PONV, whereas nurses can use nonpharmacological interventions an
-

Exploring the Relationship Between COVID-19 Unit Designation and Nurse Burnout Syndrome
Gisele Bazan, Tiffany Patterson, Kelsey Sawyer, Jamie Roney, Erin Whitley, Sahar Mihandoust, and JoAnn Long
Background: The COVID-19 pandemic impacted healthcare due to surges in infected patient and respiratory failure. Nursing burnout syndrome (NBS) results from occupational factors leading to mental health problems. Nurses working in intensive care units (ICUs) dedicated to caring for COVID-19infected individuals may be even more susceptible to NBS due to increased burdens of futile care delivery and high mortality rates within overstretched healthcare systems. Identifying socio-demographic, work-related, and psychological predictors of NBS may help organizations mitigate, or at least minimize, the negative psychological impact on ICU nurses working during future pandemics.
Purpose/Aims: The aim of this study was to compare burnout levels in ICU nurses providing direct care to COVID infected patients with nurses caring for non-COVID infected patients.
Methods: An observational descriptive study was conducted using 1) a case-controlled prospective quantitative comparative design to compare neonatal and pediatric ICU to cardiac and medical ICU survey scores measuring nurse burnout, work-related, and psychological predictors of NBS and 2) across-sectional longitudinal quantitative causal and comparative study design comparing NBS scores for nurses working in a cardiac and medical ICU captured in 2019 prior to the COVID-19 pandemic to scores captured in the same units after conversion to dedicated COVID-19 ICUs in 2020. This study will explore the relationship between three subscales(Emotional Exhaustion, Depersonalization, and Personal Accomplishment) of the Maslach Burnout Inventory (MBI) as "outcome variables" and exposure to COVID-19 infected patients during 12-hour shifts worked as "explanatory variables" in a subset regression model. The study will also measure four subscales (Vocation, Finances, Health, and Social Relationships) associated with post-traumatic stress disorder using the Well Being Instrument(WBI) as control variables. A convenience sample of direct care registered nurses working in four ICUs in a large tertiary care hospital will be recruited to participate in the study. Female nurses working day shifts were surveyed in February and March 2019in two ICUs. In November 2020, four ICUs were used for sampling of both male and female nurses working either day or night 12-hour shifts based on designation as COVID-19 ICUs.
Results: Researchers hypothesize burnout scores among nurses working in neonatal and pediatric ICUs will be less than burnout scores for nurses working in designated COVID ICUs. Additionally, investigators hypothesize nurse burnout measured in cardiac and medical ICUs in 2019 will be less than measurements obtained in 2020 after the same ICUs converted into COVID ICUs. This study will also analyze participant socio-demographic and work-related data for psychological predictors of NBS.
Conclusion: NBS has been identified as a global problem facing ICU clinicians. Pinpointing associations betweenCOVID-19 infection and nurse burnout may lead to innovative strategies to mitigate burnout in those caring for the most critically ill individuals during future pandemics.
Implications for practice: Further research is required to establish relationships between socio-demographic and work-related psychological predictors of NBS. Understanding relationships between these variables may guide development of strategies to build nurse resilience and decrease NBS in ICU settings impacted during pandemics.
-

Break habits of Registered Nurses working in the acute care setting during the COVID-19 pandemic
Michelle Bradberry, Gisele Nicole Bazan, Sahar Mihandoust, Jamie Roney, Marian Wilson, and Teresa Bigand
Background: Nurses report high levels of burnout and stress while working in the acute care setting, especially during the current COVID-19 outbreak. Evidence suggests that taking a restorative break during an extended, 12-hour shift may help mitigate stress and translate to better patient and caregiver outcomes. Yet, little is known about how Registered Nurses report taking breaks in the context of the pandemic.
Purpose/Aims: The purpose of this project was to describe the frequency of breaks reported by nurses working 12-hour shifts during the COVID-19 pandemic, and to test for demographic differences between nurses reporting fewer compared to more breaks on average during a shift.
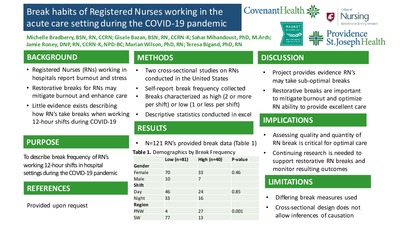
Methods/Approach: Registered Nurses delivering direct patient care in a 12-hour full-time position in the hospital setting in two different regions in the United States (U.S.) were recruited for two different studies during the peak of the COVID-19 outbreak. Demographic data were collected via self-report in both studies. To measure quantity of breaks taken during a shift, participants in the Southern U.S. region were asked, “What is the frequency of breaks you normally take during your shift between 0 (no breaks) to 4 (all provided breaks)?”. Nurse participants in the Pacific Coast study were asked, “In a typical shift, how many 15- minute breaks do you take?” and “In a typical shift, how many 30-minute breaks do you take?”. The numbers of breaks reported were summed to yield a total frequency of breaks taken by the participants in both studies. Data were analyzed using descriptive statistics to quantify the number of breaks reported, and bivariate tests assessed group differences between reporting high or low frequency of breaks.
Results: A total of 121 nurses working either in the Pacific Coast (n=31) or in the southern U.S. (n=90), were included. Across the dataset, the average number of breaks reported was 1.5 and nurses surveyed in the Southern U.S. were significantly more likely to report taking one or fewer breaks during their 12-hour shift compared to nurses working in states along the Pacific coast. There were no noted differences in education, age, gender, or shift type with respect to reported break frequency.
Conclusion This project provides an initial glimpse into self-reported breaks of nurses delivering frontline care in the hospital setting during the COVID pandemic. Nurses may not be taking all break opportunities while working during the pandemic, and efforts should be made to support the ability of frontline caregivers to consistently take all restorative breaks each shift.
Implications for Practice: Strategies for enhancing nurses’ abilities to take restorative breaks are critical, especially for nurses working on the front lines during the COVID-19 pandemic. Ensuring adequate quality and quantity of breaks for frontline caregivers may mitigate caregiver burnout and enhance well-being, potentially translating to delivery of optimal patient outcomes. Our findings are limited as strategies for measuring nursing breaks were not uniform across the two studies. Future work is needed to further characterize breaks and related outcomes among Registered Nurses providing direct patient care during COVID.
-

The benefits of fasting for patients who are immunocompromised and undergoing cancer treatment: An integrative research review
Lori Burnett
Background: In the past several decades, remarkable advances in the treatment of cancer have been made. However, a gap remains regarding best practice strategies to reduce the amount of short and long-term side effects and adverse or emergent events related to cancer treatment that may negatively impact patient quality of life. Recent evidence suggests that if patients undergoing cancer treatment fast for a period of time, they may experience reduced chemotherapy-related side effects and enhanced immune potential. Weight loss and malnutrition associated with cancer treatments highlight the importance of evidence appraisal associated with fasting prior to recommending this practice as part of an individualized cancer treatment plan.
Purpose: This review aimed to answer the clinical question: Among patients receiving active cancer treatment, does fasting enhance the immune system, increase efficacy of cancer treatment, and decrease chemotherapy-related side effects?
Methods: This review was created using Whittemore's Methodology of Integrated Research Reviews. A search of the articles using Cochran Library, PubMed, Medline, CINHAL, and Health Source: Nursing/Academic Edition was conducted. The key words used to perform the search were: "fasting" AND "immune system" AND "chemotherapy". Search criteria were limited to "free full text articles" between 2015 and 2020 except for PubMed. A total of sixteen articles resulted for review with ten more identified through bibliographic mining. All articles were critically appraised for level and strength of evidence using an evaluative checklist and the EBR (evidence-based readiness) tool.
Results: From the twenty-six unique articles identified, twelve were considered to be appropriate for the scope of this project. Of these twelve articles, two were rated to be level one, one as level two, three as level three, one as level four, and five as level five. All articles used to inform answering the clinical question reported a positive correlation with fasting and the efficacy of chemotherapy agents as well as an enhanced immune system. “Fasting” definitions varied across reviewed literature.
Conclusion: The current integrative literature review suggested that fasting may have a beneficial effect on the immune system and may mitigate adverse side effects associated with chemotherapy. Additionally, some evidence supported that among patients who fasted compared to those who did not, tumor growth was clinically decreased. While this combination of studies offered positive findings, more high-quality clinical research is needed to determine the benefits and potential harms of fasting among patients receiving active cancer treatment. Furthermore, research needs to indicate a clear definition of fasting, including optimal timing and type, before this practice can be effectively recommended in the clinical setting.
-

Exploring the relationship between exposure to nature while at work and burnout among female nurses on day shift
Jamie Roney, Sahar Mihandoust, and Stephanie Dunkle
Background: Registered Nurses working extended shifts in the hospital setting may report burnout, which reduces caregiver satisfaction, increases turnover, and potentially translates to delivery of suboptimal patient care. To align with the quadruple aim, efforts are needed to reduce nurse burnout. Limited literature suggests that visual access to nature, either via artwork or exterior landscaping, may reduce burnout. However, more research is needed to understand whether visual access to nature influences burnout among Registered Nurses delivering direct patient care.
Purpose/Aims: The purpose of this study was to explore the relationship between visual access to exterior landscaping or nature artwork and burnout among Registered Nurses.
Methods/Approach: This cross-sectional study recruited female nurses working dayshift in one large medical center to avoid potential confounders of gender and shift on burnout and exterior nature views. Participants were recruited from 6 different nursing units based on the pre-existing characteristics of unit break rooms: 1) exterior nature view and nature artwork(n=2 units; n=16 nurses);2) no exterior nature views but containing artwork of nature scenes (n=2 units; n=18 nurses); 3)no exterior nature view and no nature artwork (n=2 units; n=17 nurses).Nurses self-reported demographics as well as perceived frequency and duration of exterior nature views or nature artwork during an average shift at one point in time immediately following the end of a 12-hour shift. In addition, nurses provided burnout data by completing the Maslach Burnout Inventory (MBI),which characterizes burnout as emotional exhaustion, depersonalization, and personal achievement. Surveys were collected from February –March 2019. Data were analyzed descriptively and using a subset regression model to explore relationships between measured variables.
Results: A total of 51 Registered Nurses working 12-hour day shift in the hospital setting reported on average low to moderate burnout. In the multivariable model, nurses who self-reported more time viewing natural light during a shift reported lower burnout subscales of emotional exhaustion and depersonalization compared to those reporting less time viewing exterior nature during the shift. The subscale of personal achievement was not significantly related to nurses’ perception of nature views.
Conclusion: Our study supports that the amount of self-reported exposure to nature primarily through window views throughout 12-hour shifts may impact nurse burnout scores. However, the burnout subscale of personal achievement appeared to be independent of nature views, suggesting that future work should explore other factors that may support this nurse burnout sub-component.
Implications for Practice: Our study provides preliminary evidence that increasing nurse-perceived exposure to nature through window views of exterior landscaping during a 12-hour day shift may mitigate the amount of burnout reported. Nurses could partner with therapeutic architects to advocate for work and break areas containing windows, balconies, alcoves and indoor/outdoor gardens to enhance opportunities for nurses to view exterior landscaping for greater frequencies during a shift to decrease burnout. Future studies are needed to test long-term outcomes related to nurse views of nature and burnout, acknowledging that solutions to support burnout may require multifactorial approaches.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}