
-

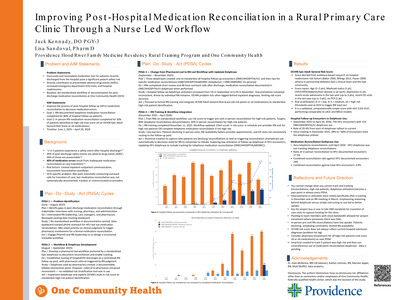
Improving Post-Hospital Medication Reconciliation in a Rural Primary Care Clinic Through an RN-Led Workflow
Jack Kennady
Context/background: Adverse events after hospital discharge are common and represent a major patient safety concern. Approximately 1 in 5 patients experience a safety event after discharge, and 39% of these events are adverse drug events (ADEs), with 26% considered preventable. Medication discrepancies during transitions of care contribute significantly to these events, with an estimated 40% of medication errors resulting from inadequate medication reconciliation. Rural primary care clinics face additional challenges, including limited communication between inpatient and outpatient systems and inconsistent reconciliation workflows. Improving medication reconciliation during the transition from hospital discharge to outpatient follow-up represents an important opportunity for family medicine practices to reduce preventable ADEs. Objective: To implement and evaluate a standardized RN-led workflow to improve medication reconciliation for patients discharged from the hospital and presenting for follow-up at One Community Health. Project goals included completion of telephone medication reconciliation for 80% of hospital follow-up patients and in-person RN medication reconciliation visits for 50% of patients identified as high risk. Methods: Quality improvement project conducted at One Community Health in Hood River, Oregon using sequential Plan-Do-Study-Act (PDSA) cycles from June 2025 to June 2026. • PDSA 1 (June–Aug 2025): Problem identification; stakeholder interviews (nursing leadership, care managers, pharmacists, administrators). Baseline: no standardized workflow or documentation for post-discharge medication reconciliation. • PDSA 2 (Aug–Sept 2025): Workflow design; development of standardized EHR dotphrase to document medication reconciliation and enable tracking. • PDSA 3 (Sept–Nov 2025): Implementation of documentation intervention. Hospital discharges (ED and inpatient) routed to a centralized follow-up pool. RN chart review and outreach calls within 48 hours; medication list review and reconciliation documented using dotphrase. • PDSA 4 (Dec 2025–Mar 2026): RN training and workflow integration. Standardized reconciliation during outreach calls and prior to follow-up visits scheduled within 7–14 days. • Next cycle: Audit outcomes, identify barriers, refine workflow to improve reconciliation rates toward target goals. • Data sources: EHR dotphrase utilization and hospital follow-up encounter chart review Results: Between September 2025 and February 2026, 462 hospital follow-up visits were identified. RN-led medication reconciliation documentation occurred in 100 encounters (21.6%). After dotphrase implementation in September, reconciliation rates increased from 1.6% in September to 13.6% in November. Following RN workflow training in December, telephone reconciliation documentation increased to 71.7% of follow-up visits that month and 54.4% in January. Further manual data analysis will be performed at the end of March and June to determine how many telephone medication reconciliations were completed and how many high risk patients had completed medication reconciliations in-person with RN prior to provider appointments. Discussion/conclusions: Medication discrepancies during care transitions are a major contributor to preventable ADEs in primary care. Implementation of a standardized RN-led medication reconciliation workflow improved the clinic’s ability to identify recently discharged patients and document reconciliation prior to follow-up visits. Early findings suggest nursing-led interventions and standardized EHR tools can strengthen transitional care processes in rural family medicine practices. Continued evaluation will assess how best to implement medication reconciliations in a team-based setting
-

Improving Recognition of Chronic Kidney Disease in a Federally Qualified Health Center Through a Quality Improvement Initiative
Rachel Monroe, Evan Saulino, and Kathleen McKenna
Context/background: Chronic kidney disease (CKD) affects approximately 15% of adults in the United States, yet nearly 90% of affected individuals are unaware of their diagnosis. Early identification in primary care enables interventions such as blood pressure optimization, renin –angiotensin system blockade, and kidney -protective medications that can significantly delay disease progression and postpone dialysis. Screening and diagnosis gaps disproportionately affect high -risk populations, including Latinx patients and immigrant agricultural workers commonly served in federally qualified health centers (FQHCs). National CKD screening rates among patients with diabetes or hypertension remain low, leaving many high -risk individuals unscreened for kidney disease. Improving CKD screening and recognition in primary care is critical to reducing disparities and preventing progression to advanced kidney disease. Objective: To identify system and provider barriers to CKD screening and diagnosis in a FQHC in Oregon and evaluate whether targeted workflow improvements and provider education improve CKD screening, recognition, and documentation in the electronic medical record (EMR). Methods: Quality improvement project conducted primarily in an FQHC in Hood River, Oregon using iterative Plan -Do-Study -Act (PDSA) cycles. PDSA cycle 1 established baseline CKD screening rates using EMR data among patients seen within the previous 18 months and at increased risk for CKD. Screening was defined as having both serum creatinine/eGFR and urine albumin test results in the EMR. Screening rates ranged from 53–68% across risk groups and 54% overall, substantially higher than national estimates. PDSA cycle 2 evaluated laboratory workflows affecting urine specimen collection for albuminuria testing and implemented process adjustments to improve specimen collection reliability. PDSA cycle 3 compared expected CKD prevalence in high -risk populations with documented diagnoses in the EMR, revealing lower -than- expected diagnosis rates (9.4% vs expected 25–30% among patients with hypertension and 12.3% vs expected 30–40% among patients with diabetes). PDSA cycle 4 surveyed clinicians regarding barriers to CKD diagnosis; 21 of 41 clinicians responded (12 MD/DO, 6 NP/PA, 3 residents). Areas of lowest confidence included explaining CKD diagnosis and prognosis, counseling on lifestyle modification, initiating SGLT2 inhibitors, and determining when to refer to nephrology. PDSA cycle 5 implemented a targeted educational session addressing these gaps, followed by a repeat survey (15 responses). Results: Post-intervention survey responses demonstrated increased provider comfort in several previously identified areas. The proportion of clinicians selecting the two highest Likert -scale categories increased for explaining CKD diagnosis and prognosis (71% [15/21] to 93% [14/15]), counseling patients on lifestyle modification (76% to 93%), and initiating SGLT2 inhibitors (81% to 93%). Preliminary EMR review suggests increasing CKD problem list documentation among high -risk patients following the intervention; additional pre/post analysis is ongoing. Discussion/conclusions: In this FQHC population with relatively strong CKD screening rates, underdiagnosis remained a significant care gap. A structured quality improvement approach addressing both workflow and provider barriers improved clinician confidence and may increase CKD recognition in primary care. Improving CKD documentation in the EMR supports earlier guideline -directed management and represents a feasible strategy for strengthening CKD care in community health centers.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}