
Files
Download Full Text (680 KB)
Publication Date
4-29-2026
Keywords
oregon, psvmc, psvmc gme, psvmc oaa
Disciplines
Gastroenterology | Medical Education | Oncology
Abstract
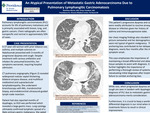
Pulmonary lymphangitic carcinomatosis (PLC) accounts for approximately 8% of pulmonary metastases and is primarily associated with breast, lung, and gastric cancers. Chest radiographs are often nonspecific and normal in approximately 50% of cases. We present a case of PLC as an initial presentation of metastatic gastric adenocarcinoma. A 57-year-old White woman with prior tobacco use, asthma, and multiple sclerosis on Natalizumab presented with three months of progressive dyspnea and cough. She was evaluated multiple times and treated with various antibiotics and inhalers for presumed bronchitis. Despite this, her symptoms worsened, prompting hospital evaluation. She was tachycardic and markedly hypoxemic on arrival. A high-resolution computed tomography (CT) scan revealed widespread nodular septal thickening, bilateral airspace disease, and multifocal mediastinal and supraclavicular lymphadenopathy most concerning for lymphoma or atypical infection. She underwent bronchoscopy with bronchoalveolar lavage, transbronchial biopsy, and endobronchial ultrasound guided lymph node resection. She also reported progressive dysphagia with solid foods and significant weight loss over the prior months, so esophagogastroduo denoscopy was performed with pathology showing a poorly differentiated adenocarcinoma. Lung cytology confirmed lymphatic spread of a likely primary gastric malignancy. She opted to discharge on hospice. Given our patient’s asthma and immunosuppressive therapy, her progressive dyspnea and cough were easily readily attributed to reactive airway disease or infection. Her chest imaging findings also clouded the picture somewhat and her demographics were not typical of gastric malignancy as it is half as common in women and has very low prevalence in the non-Hispanic White population. Natalizumab therapy was also not associated with increased risk of malignancy in a recent cohort study. This anchoring bias contributed to her delayed diagnosis, as her weight loss and dysphagia were not uncovered until she was hospitalized, four months after the initial symptom onset. In a similar case, a man presenting with respiratory symptoms whose imaging showed only bilateral ground-glass opacities was felt to have non-malignant disease until trans-bronchial biopsy revealed metastatic gastric adenocarcinoma. Both cases emphasize the importance of maintaining a broad differential and obtaining tissue samples to assist with diagnosis. Our case highlights the importance of performing a thorough review of systems and reevaluating initial diagnoses after initial treatment failure to combat anchoring bias. When progressive dyspnea and cough are seen in tandem with dysphagia, the otherwise very rare diagnosis of PLC due to metastatic gastric adenocarcinoma merits consideration.
Area of Special Interest
Digestive Health
Area of Special Interest
Cancer
Specialty/Research Institute
Graduate Medical Education
Specialty/Research Institute
Internal Medicine



