
Files
Download Full Text (1.2 MB)
Publication Date
4-29-2026
Keywords
oregon, psvmc, psvmc gme, psvmc gme pharmacy
Disciplines
Medical Education
Abstract
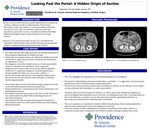
Introduction: The most common cause of ascites is portal hypertension secondary to cirrhosis and accounts for nearly 75% of cases. In contrast, pancreatic ascites is a rare presentation of ascites and occurs in less than 1% of patients. Because of its low prevalence, pancreatic ascites is often excluded from the initial differential diagnosis and rarely assessed in ascitic fluid analysis. This is a case in which pancreatic ascites was considered and ultimately confirmed based on the overall clinical picture, challenging the initial assumption of portal hypertension and cirrhosis. Case Presentation: A 47-year-old man with ongoing alcohol use disorder presented to the emergency department with abdominal pain. Initial work-up revealed a lipase >1000 U/L, multiple pancreatic calcifications, large-volume ascites, and portal vein thrombosis on abdominal CT scan. A diagnosis of alcohol -related acute-on-chronic pancreatitis, cirrhosis, and portal vein thrombosis were suspected. Diagnostic paracentesis showed a serum-ascites-albumin gradient (SAAG) of 1.2, supporting portal hypertension, though notably close to the cutoff of 1.1. He was discharged on diuretics and outpatient follow-up for presumed new alcohol related cirrhosis despite CT showing normal-appearing liver. Three weeks later, he returned with persistent abdominal pain and worsening ascites. Repeat CT demonstrated pancreatic head calcifications and a developing pseudocyst. A second paracentesis was performed, and ascitic fluid lipase was ordered, resulting >7000 U/L-- confirming a pancreatic fluid leak. A nasojejunal (NJ) tube was placed for enteral nutrition to allow pancreatic rest, with plans for serial imaging prior to NJ removal. Discussion: This case highlights the importance of reconsidering diagnostic assumptions and recognizing cognitive biases. The patient’s initial findings of portal vein thrombosis and SAAG >1.1 suggested ascites from portal hypertension. The history of chronic alcohol use led to the assumption of cirrhosis as the ultimate cause of both ascites and portal vein thrombosis, with ongoing alcohol use to explain pancreatitis. However, his lack of response to diuresis, as well as pancreatic pseudocysts on imaging, our team investigated other potential causes of ascites, including pancreatic leak. Checking a lipase in the ascitic fluid was essential to ensure the patient received the appropriate treatment, as pancreatic rest would not have otherwise been considered. This case represents an important reminder to think critically about all tests being ordered for a patient and avoid premature closure on diagnostic reasoning. Clinicians should consider adding lipase or amylase to peritoneal fluid studies if there is a suspicion for pancreatic component, even if there is another etiology to explain the ascites
Specialty/Research Institute
Graduate Medical Education
Specialty/Research Institute
Pharmacy



