
Files
Download Full Text (843 KB)
Publication Date
4-29-2026
Keywords
oregon, psvmc, psvmc gme, psvmc oaa
Disciplines
Medical Education
Abstract
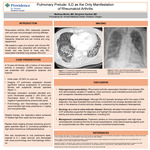
Abstract: Rheumatoid arthritis (RA), a systemic autoimmune disorder, classically presents with joint pain and prolonged morning stiffness. Extra-articular pulmonary manifestations are frequently observed but can be the primary initial presentation. We present a case of a women with chronic RA in remission who presented with shortness of breath and was found to have new RA-associated interstitial lung disease (RA-ILD). A 74-year-old female with a history of rheumatoid arthritis in remission, chronic obstructive pulmonary disease, and recent admission for septic shock presented with progressive dyspnea and hypoxia. Initial vitals noted an oxygen saturation in the low 80s. CT pulmonary angiography excluded pulmonary embolism but demonstrated significant interval progression of basilar predominant pulmonary fibrosis with subpleural reticular opacities compared to imaging seven months prior. Pulmonology was consulted and recommended high-dose prednisone (1 mg/kg). Serologic evaluation revealed elevated anti-cyclic citrullinated peptide(> 250 U/ml) and rheumatoid factor(> 500 IU/ml), with a negative hypersensitivity pneumonitis panel. Rheumatology agreed with mycophenolate monotherapy given lack of synovial involvement. Despite therapy, her respiratory status declined, necessitating heated high-flow nasal cannula support. Repeat chest imaging showed worsening ground-glass opacities, prompting escalation to high-dose intravenous methylprednisolone, which led to gradual clinical improvement. She transitioned to an oral prednisone taper, weaned to 6 L nasal cannula, and discharged with close pulmonology and rheumatology follow-up. RA-ILD chest CT findings are variable but most commonly demonstrate usual interstitial pneumonia (UIP) or nonspecific interstitial pneumonia (NSIP) patterns, although organizing pneumonia and rheumatoid nodules are also well described. While RA-ILD typically develops within five years of RA onset, our patient exhibited pulmonary manifestations decades after diagnosis, highlighting the marked heterogeneity in disease presentation. Furthermore, the absence of articular involvement further distinguishes this case, as most patients with RA-ILD exhibit at least some degree of joint disease. The presence of markedly elevated rheumatoid factor and anti-cyclic citrullinated peptide (anti-CCP) antibodies supported the diagnosis in this case and aligned with known associations between serologic activity and extra-articular disease expression. Current treatment strategies for RA-ILD emphasize systemic steroids and DMARDs, and like our patient, most receive high-dose steroids for management of acute flare, though augmentation with mycophenolate was selected given the predominance of pulmonary involvement. Since there are no dedicated randomized controlled trials in this area, treatment is based on observational data and expert opinion and should include a multidisciplinary approach to optimize patient outcomes.
Specialty/Research Institute
Graduate Medical Education
Specialty/Research Institute
Internal Medicine



