
-

Inpatient Registered Nursing Use of Evidence-Based Practice Tools to Manage Withdrawal Symptoms among Adults Hospitalized with Acute Alcohol or Opioid Withdrawal: A Needs Assessment
Julie Baker and Teresa Bigand
Background: Patients who suffer from alcohol or opioid use disorder face unpleasant and potentially life-threatening complications related to substance withdrawal when hospitalized. Evidence suggests that the use of a standardized tool to rate withdrawal severity and direct treatment, including score-driven medication dosing to alleviate withdrawal, leads to improved clinical outcomes. However, clinical nurses working in the inpatient medical-surgical specialty in a large medical center questioned whether all nurses were effectively using evidence-based practice (EBP) tools to assess and treat alcohol or opiate withdrawal severity.
Purpose/Aims: To understand nursing practice at one hospital regarding use of ministry-specific evidence-based practice tools for rating symptom severity for alcohol and opioid withdrawal.
Methods/Approach: A needs assessment using a cross-sectional survey was conducted to understand nursing practice regarding use of two EBP tools for rating withdrawal symptom severity: the Clinical Institute Withdrawal Assessment for Alcohol (CIWA), and the Clinical Opioid Withdrawal Scale (COWS). Two fictitious withdrawal case studies were developed: one illustrating an inpatient withdrawing from alcohol, and the other depicting withdrawal from opiates. Professional Development Specialists collaborated to enact the scenarios and video recorded each patient case. Nurses working on adult medical-surgical units received an electronic survey link containing the written and recorded patient cases. Nurse participants were instructed to first read and watch each case, then to calculate either a CIWA or COWS score based on the presented cases.
Results: A total of 61 Registered Nurses completed the survey out of a possible 191 eligible nurses. Of these, 97% correctly scored the case illustrating opiate withdrawal using the COWS tool. However, only 35% correctly assigned the CIWA score based on the alcohol withdrawal exemplar. In all, 60% of participants assigned a higher symptom severity than expected using the CIWA tool. The CIWA items with the most inconsistent scores were anxiety, agitation, and visual hallucinations.
Conclusion: Nurses at our ministry responded positively to completing a survey featuring written and videotaped case scenarios to identify gaps in practice using the CIWA and COWS tools. Our innovative needs assessment pointed to a gap in standard practice for using the CIWA but not the COWS tools. Targeted education on enhancing nursing assessment of anxiety, agitation, and visual hallucinations in this population may optimize symptom rating and subsequent protocol-driven treatment.
Implications for Practice: Improper scoring with the CIWA tool could trigger an inappropriate medication dose administered to the patient. A future opportunity to educate nurses in our ministry could lead to an improvement in appropriate alcohol withdrawal symptom rating and treatment.
-

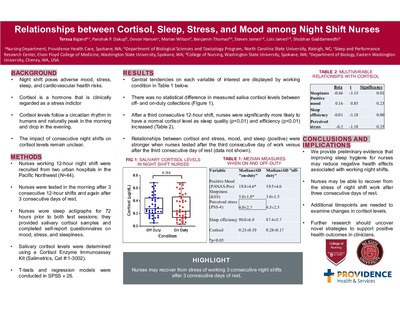
Relationships between Cortisol, Sleep, Stress, and Mood among Night Shift Nurses
Teresa Bigand, Panshak P. Dakup, Devon Hansen, Marian Wilson, Benjamin Thomas, Steven James, Lois James, and Shobhan Gaddameedhi
Background: Working night shift is a physical and emotional stressor related to negative health outcomes. Cortisol is a biomarker that has been related to an increased risk for metabolic syndrome among adults. Cortisol levels follow a circadian rhythm in humans; levels reach a peak in the early morning and drop to the lowest level in the late evening. Changes in cortisol levels have been related to changes in mood or sleep and to exposure to stressful situations. In a group of Registered Nurses, the impact of consecutive 12-hour night shifts on relationships between cortisol levels, sleep, stress, and mood, was not well-defined.
Purpose: To determine relationships between cortisol, sleep, and self-reported mood and stress among nurses working 12-hour night shift after a third consecutive day of work and after a third consecutive day of rest. Methods: Nurses working 12-hour shifts were recruited from two major hospitals in an urban city in the Pacific Northwest to participate in a variety of tests immediately after finishing a third consecutive 12-hour shift and again after a third consecutive day off work. Nurses wore wrist actigraphs for 72 hours prior to both test sessions as an objective measure of sleep. During each test session, nurses completed self-report questionnaires to describe mood, stress, and sleep quality and also provided saliva samples from which cortisol levels were measured. Results: A total of 44 night shift nurses met criteria for data analysis. After a third consecutive 12-hour shift, nurses were significantly more likely to have a normal cortisol level as sleep quality (p<0.01) and efficiency (p<0.01) increased. Expected relationships between cortisol and stress, mood, and sleep were stronger when nurses were tested after the third consecutive day of work versus after the third consecutive day of rest.
Conclusion: We provide preliminary evidence that improving sleep hygiene for nurses may reduce negative health effects associated with working night shifts. Furthermore, nurses may be able to recover from the stress of night shift work after three consecutive days of rest.
Implications for practice: Registered Nurses need to provide 24-hour care to hospitalized patients, and further research should uncover strategies to support positive health outcomes for these clinicians. While our sample was small, we hypothesize that improving sleep hygiene for nurses working consecutive 12-hour night shifts may support health outcomes. Future studies with more frequent cortisol measures are needed to examine time-sensitive changes in cortisol levels.
-

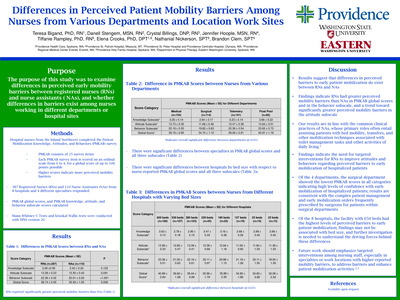
Differences in Perceived Patient Mobility Barriers Among Nurses from Various Departments and Location Work Sites
Teresa Bigand, Danell Stengem, Crystal Billings, Jennifer Hoople, Tiffanie Rampley, Elena Crooks, Nathaniel Nickerson, and Brandon Clem
Background: Hospitalized patients suffer negative outcomes related to lack of mobilization activities such as falls with injury or infection. Mobility requires a multi-disciplinary team approach including Registered Nurses (RNs), Certified Nursing Assistants (NA-Cs), and Physical/Occupational Therapists (PT/OTs) to promote best patient outcomes. The Johns Hopkins Culture of Mobility toolkit provides evidence-based practices for integrating multi-disciplinary mobilization efforts for hospitalized patients. This toolkit had not been implemented on a busy orthopedic post-operative nursing unit in one large hospital.
Purpose/aims: To test the impact of the culture of mobility toolkit on caregiver perceptions of mobility barriers and evaluate the implementation of the toolkit on a surgical acute care unit.
Methods/Approach: This quality improvement project was implemented on an orthopedic post-surgery inpatient unit in a large medical center in the Pacific Northwest. A pre-survey was administered to RNs, NA-C's and PT/OTs prior to the implementation of this project, and those findings guided the development of an educational intervention. The education was a poster on the Johns Hopkins Culture of Mobility toolkit with focus on using the toolkit's mobility screening tool presented to RN's, NAC's and PT/OT's. Caregivers were also informed to complete a form each shift on the following: the patient's Highest Level of Mobility score, the patient's mobility goal for the shift, whether the patient met the personal goal, and barriers/facilitators to the patient's ability to meet personal goals. Staff were directed to complete tracking sheets each shift for each patient during a 6-week period. After the intervention, all staff were invited to complete the post-survey to re-assess perceived mobility barriers.
Results: More than 90 caregivers completed the pre-intervention perceived mobility barriers survey, which suggested that staff felt that patient mobilization efforts were time-intensive and posed an injury risk for caregivers. After the education was provided, over 240 mobility tracking sheet were submitted by mainly RN's working night shift, and 65% of caregivers reported that the patient's self-reported mobility goal was met by the end of the shift. Barriers to achieving patient-created mobility goals included inadequate symptom management, reduced patient-specific motivation to move, and lack of adequate resources to safely mobilize patients. A total of 32 caregivers responded to the post-project mobility survey, revealing a significant decrease in overall perceived mobility barriers from preintervention levels. PT/OTs reported significantly less barriers compared to nursing staff at both time points.
Conclusion: This project demonstrated that multi-disciplinary staff working on a busy orthopedic postsurgical floor can adopt evidence-based practice tools to promote mobility which may facilitate increased patient mobilization activities. Future projects may include greater adoption of the toolkit throughout the medical center.
Implications for practice: Hospital-based mobility programs such as the Johns Hopkins Culture of Mobility toolkit can mitigate functional decline of adults following hospitalization. Inpatient mobility activities may be enhanced by engaging patients to set and attain mobility goals each shift, partnering with PT/OTs, identifying patient motivation to mobilize, and optimizing symptom management.
-

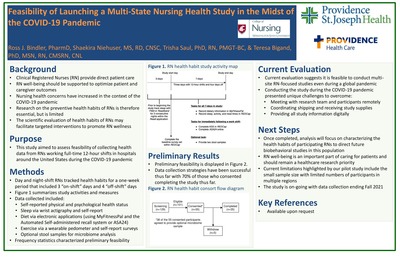
Feasibility of launching a multi-state nursing health study in the midst of the COVID-19 pandemic
Ross Bindler, Shaekira Niehuser, Trisha Saul, and Teresa Bigand
Background: The Quadruple Aim recommends that healthcare institutions support clinician well-being as a strategy to improve patient and caregiver outcomes. During the COVID-19 global pandemic, Registered Nurses (RNs) working full-time, 12-hour shifts have reported increasing health concerns. Therefore, research documenting objective information on preventive health habits of RN’s is needed to support nursing well-being. Yet, conducting bio-behavioral research in this population, especially during the pandemic, presents with unique challenges. Purpose: The purpose of this pilot study to assess the feasibility of collecting and evaluating health data from RNs working full-time, 12-hour shifts across the United States during the COVID-19 pandemic. Methods/Approach: This observational descriptive study recruited 12-hour shift RNs working in a large health system in the United States. RNs wore a wrist actigraph for 10 days, maintained a seven-day electronic food diary, tracked daily step counts using a wrist pedometer, and optionally provided two stool samples for sequencing analysis. Nurses completed an online screening form to assess for study eligibility, and were contacted by a research team member to provide consent if they met eligibility criteria. Research staff created and shared a digital workbook to explain the protocol as well as an interactive online course to provide standardized education on completing electronic food diaries. Participants were mailed devices for tracking health habits. Research staff were available to participants via phone call or email to answer questions at any point during the study. Participants were invited to complete an optional post-study feedback survey to describe the experience of being involved in the study. Recruitment began in October 2020 and the study is still open for participant enrollment. Results: At this time, 82 nurses met study criteria and 49 consented to participate (n=27day shift and n=22night shift). Of these, 37 volunteered to provide a stool specimen. Of the consented nurses, a total of 5 have withdrawn for reasons such as family or school issues. Out of 32 nurses who have completed the study, 22 provided a stool specimen, 2 forgot to collect despite consenting, and9 nurses provided feedback where 66% reported reviewing the online module course. Of those who completed the study, 100% successfully captured sleep data using the wrist actigraph, yet 15.6% required research staff assistance with documenting some aspect of the food diaries. Conclusion: Preliminary findings suggest that it is feasible for nurses to provide objective health information in the context of working full-time, 12-hour shifts during a global pandemic. Future work is needed to understand best strategies for conducting bio-behavioral research among RNs providing direct patient care in the hospital setting. Implication to Practice: Research is needed to characterize health habits of nurses, particularly those providing full-time, direct patient care, to support caregiver well-being and facilitate optimal patient outcomes. Preliminary findings suggest that while barriers exist that restrict nursing involvement in bio-behavioral studies, especially during the pandemic, nurses may successfully participate in studies which could leverage understanding of short and long-term health needs for this population.
-

Pain Management Trends among Adults Hospitalized with Cellulitis: An Evidence-based Practice Project
Nonna Dobyns, Teresa Bigand, Kristopher Darath, and Denise Ogorek
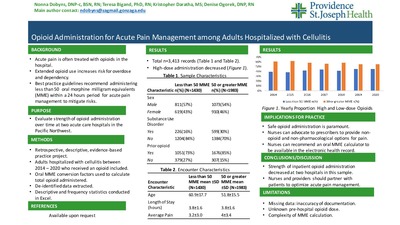
Background: Cellulitis is an acute infection of the skin resulting in acute pain and often requires pharmacological analgesics. Past studies revealed that more than half of patients receiving inpatient medical care in the United States received opioid analgesics for pain management during the hospital stay. While opioids are regarded as the strongest analgesic available to ease physical pain, these are habit-forming drugs that contribute to negative outcomes such as opioid use disorder and increased risk for accidental overdose and death. Recommendations for acute pain management in the hospital setting include prescribing less than 50 morphine milligram equivalents (MME's) per day to avoid negative outcomes. Although it is known that opioids should be administered at low doses to treat acute physical pain in the hospital, it is unclear how opioid administration practices have evolved over time to align with best practices in two acute care hospitals in the Pacific Northwest.
Purpose/aims: Our purpose was to evaluate how inpatient opioid administration evolved between the years 2014 and 2020 in two acute care hospitals for a model population with acute pain: adults with cellulitis.
Methods/Approach: Retrospective, de-identified data were extracted from the electronic health records for adults with a primary diagnosis of cellulitis. Records included in the analysis reflected patients age 18 years and older, hospitalized with cellulitis for at least 24 hours but no more than 7 days, treated at one of two hospitals in the Pacific Northwest between the years 2014 and 2020, and administration of an opioid medication during the encounter. Data were analyzed in Excel using descriptive and frequency statistics.
Results: A total of 3,413 inpatient records were included in the analysis. In this sample, adults who received high-dose opioids during the hospital stay were younger, more likely to have a documented substance use disorder, more likely to report taking an opioid within 30 days of the hospital encounter, and reported more pain than those who received low-dose opioids. The proportion of adults receiving high-dose opioids during the hospital stay for cellulitis decreased over time from 61% to 55%.
Conclusion: This project supports that opioid administration has evolved over time to align with best practice guidelines for alleviating acute pain. Future work is needed to further characterize what factors influence the strength of opioids administered in the hospital to manage acutely painful conditions such as cellulitis.
Implications for practice: Safe opioid prescribing is paramount to ensure effective short and long-term patient outcomes. It is important for nurses to advocate to prescribers to ensure all appropriate non-opioid analgesics and non-pharmacological pain management techniques are available to ease patient suffering as well as reduce high-dose opioid administration to avoid potential patient harms.
-

Implementing IDEAL Discharge Planning: A Quality Improvement Project on an Inpatient Unit
Dawn Doud, Brenda Senger, Karen Colorafi, and Teresa Bigand
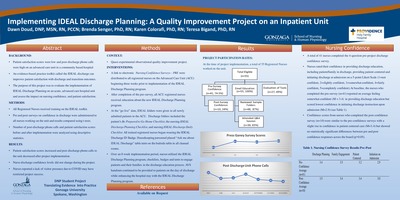
Background: Effective discharge teaching reduces 30-day hospital readmissions, decreases unnecessary emergency room visits, improves patient satisfaction, and is cost effective for hospitals by improving the Centers for Medicare and Medicaid Services (CMS) measures for reimbursement. Evidence suggests that standardized discharge teaching templates embedded within the electronic health records lack patient engagement and can fail to meet individual patient discharge education needs. A need was identified to improve the discharge planning process on an advanced care unit in a community based hospital.
Purpose: The purpose of this project was to evaluate and assess the implementation of an evidence based toolkit, IDEAL Discharge Planning, on an acute, advanced care hospital unit.
Methods: This quality improvement project included surveys that were electronically sent to measure both nursing confidence and nursing perception of the IDEAL tool kit effectiveness. Nursing Confidence Survey scores including brief demographic data (years as an RN, nursing education level, and current FTE position) were collected using an automated response tool (REDCap)both before the implementation of the toolkit and after. Over an 8-week implementation period, nurses utilized the IDEAL Discharge Planning program to engage patients and their families in the discharge education process. Standard of care “after visit summary”(AVS) handouts continued to be provided to patients on the day of discharge although these were enhanced by the IDEAL Discharge Planning program. The number of patient phone calls to the unit were tallied and compared 3 months pre and post-intervention. Patient satisfaction scores, specifically Press Ganey -Patient Discharge Care at Home were collected as a quarterly measure before and after the intervention. Nurses' perceptions of the use and effectiveness of the IDEAL checklists, badge cards, and table tents was collected from the Evaluation of IDEAL Tool Survey using REDCap. Likert-scaled and open-ended responses were collected.
Results: A total of 55 registered nurses received education on the IDEAL Discharge Planning toolkit. Of these, 27 provided feedback on the use of the tools and 10 provided pre and post confidence scores. Statistical analysis demonstrated no change in nursing confidence pre and post implementation. Post discharge phone calls to the unit significantly decreased and patient satisfaction scores significantly increased during the post implementation time frame. Nurses reported low frequency of tool usage primarily related to COVID-19 pandemic.
Conclusion: Evidence demonstrates that effective discharge education requires engagement with the patient and family during the patient's entire hospital stay. Nurses reported barriers from visitor restrictions that negatively impacted implementation of the IDEAL Discharge Planning toolkit.
Implications for practice: This quality improvement project demonstrated some positive impacts on patient satisfaction and should be re-trialed when the visitor restrictions from COVID-19 have been removed
-

Reducing Hospital Acquired Pressure Injuries on an Advanced Care Unit
Dawn Doud and Lynn Stapleton
BACKGROUND: Hospital-acquired pressure injuries (HAPIs) are increasing nationwide. HAPIs are a negative outcome of hospitalization and these conditions are not eligible for reimbursement, resulting in billions of dollars of healthcare costs to hospitals. HAPI rates were noted to climb on an advanced care unit in a community-based hospital in the Pacific Northwest. In order to reduce this patient harm event, the nurse manager partnered with the nursing professional development specialist to lead a HAPI prevention quality improvement plan.
PURPOSE: To decrease HAPI rates on the Advanced Care Unit.
METHODS: The nurse manager conducted a deep dive on all HAPI events on the unit and identified a wide variance of scores assigned using the evidence-based practice tool for assessing risk for skin breakdown: the Braden Scale. The nurse manager required all nurses who were involved in the care of patients who developed a HAPI in 2020 to complete a facility-specific HAPI investigation tool. Each nurse was responsible to meet one on one with the manager to review the information together. Next, all nurses working on the advanced care unit were administered a survey containing two standardized patient cases and were required to assign a Braden score based on each case. Nurses then completed an educational module detailing best practice on assessing skin breakdown risk and appropriate nursing interventions for preventing injury. In addition, nurses were required to complete a two-RN skin check utilizing a half-sheet paper tool passed on from nurse to nurse on all patients newly admitted or transferred to the unit and to conduct a 2-RN skin assessment during each shift report on patients with a Braden less than 18 or receiving any supplemental oxygen. Finally, three months after the interventions, nurses repeated the cases studies and assigned appropriate Braden scores. The nurse manager monitored for changes to unit HAPI rates as well as improvement in nursing accuracy for assigning the Braden score.
RESULTS: After implementation of the nursing education, the unit HAPI rate reduced to zero. The unit has sustained this rate for one year. In addition, nursing ability to assign appropriate Braden scores greatly improved. Results from case studies and quality outcomes were shared with staff.
CONCLUSIONS: Best practice interventions can greatly improve nursing ability to identify patients who are high-risk for pressure-related skin injury and appropriately intervene. Ensuring that nurses have proper training and confidence to assign an appropriate Braden score and implement corresponding clinical actions may be a first step to reducing patient harm related to HAPI's.
IMPLICATIONS FOR PRACTICE: Clinical nurses may benefit from receiving educational in-services on prevention of HAPI's. In addition, active support from nursing leadership and professional development specialists to enhance routine surveillance of skin health may assist with sustaining positive change in the acute care nursing setting.
-

Postpartum Depression Screening to Improve Maternal Outcomes
Jill Goebel and Jeff Ramirez
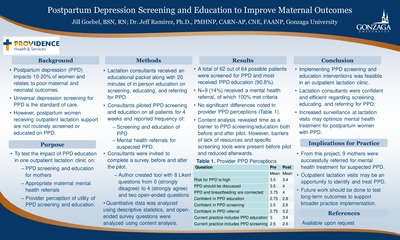
Background: Postpartum depression (PPD) is correlated with worsened maternal and infant health outcomes, and an estimated10-20% of women experience this condition after giving birth. Universal depression screening for PPD in maternity and well-child appointments is the standard of care. However, PPD screening is not well-integrated into outpatient lactation visits which assist new moms with difficulties breastfeeding. To address this gap, routine PPD screening and education was implemented in an outpatient lactation clinic servicing postpartum women in Eastern Washington. Purpose: The purpose of this quality improvement project was to implement the use of PPD screening in a lactation clinic to increase appropriate maternal mental health referrals and enhance provider perception of the clinical need for PPD education in the lactation clinic setting. Methods: Lactation consultants working at a single outpatient clinic servicing postpartum women in Eastern Washington were invited via email to complete a pre-intervention survey on knowledge and confidence in screening and intervening for PPD symptoms in early 2021. Consultants then attended a training session offering information on how to screen for, provide education about, and appropriately refer patients for suspected PPD. The lactation consultants were then requested to incorporate a PPD screen on every patient receiving care in the clinic for a four-week period and to track on a sheet of paper the number of patients: presenting for an appointment, receiving PPD screen, receiving education on PPD, and receiving a referral for potential PPD. At the end of the four-week intervention, consultants were invited to repeat the initial survey. Data was collected and analyzed using descriptive statistics to quantify the providers’ perceptions of PPD before and after the intervention. Open-ended survey items were analyzed using content analysis. Results: 62 of 64 patients were screened during the data collection period meaning 96.9% of patients who attended the lactation clinic received screening for PPD. 90.6% of patients received PPD education, and 100% of patients who were screened were referred correctly for PPD. 14% of patients who were screened received a referral. There were no statistically significant differences in the pre and post-test in the perception of the lactation consultants. Content analysis revealed barriers to PPD screening and education were reduced following the training session, but lack of time was still seen as a barrier.
Conclusion: Incorporating PPD screening and education into the standard of care provided at lactation consultations is another avenue to offer women resources and support needed to cope with symptoms of PPD. In addition, the integration and normalization of this conversation during lactation visits may help reduce the negative stigma surrounding mental health conditions for vulnerable populations such as new mothers. Implications for Practice: This quality improvement project shows that lactation consultants can incorporate PPD screening and education into their practice to improve maternal care. Findings from this project may justify a permanent change to workflow in this clinic to continue routine PPD screening and educating. Future work should be done to advocate for similar lactation clinics to consider adopting this practice as well. -

Evaluation of a Coronary Artery Bypass Graft Care Steps Program
Sheri Havel, Karen Colorafi, and Mirjeta Beqiri
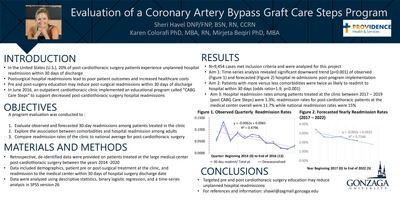
Background: Across the U.S., 20% of cardiothoracic surgery patients who are discharged to home experience unplanned readmission within 30 days of discharge. Readmissions and postsurgical complications are associated with poor patient outcomes, increased mortality rates, and increased cost of healthcare. Evidence-based recommendations for reducing preventable readmission are limited, although there is some indication that high quality pre-operative and discharge education can reduce this burden. Providing appropriate patient education at time of discharge from acute care to home regarding medication adherence, prescheduled follow-up appointments, wound management and monitoring, and symptom management education is theorized to have a significant positive impact on patient outcomes.
Purpose/aims: The primary purpose of this program evaluation was to evaluate 30-day readmission rates at a large medical center in the Pacific Northwest prior to, during, and after the implementation of a comprehensive program of patient education designed to support patients undergoing elective cardiothoracic surgery at an outpatient cardiothoracic clinic staffed by cardiothoracic surgeons who performed operations at the medical center.
Methods/Approach: This program evaluation used an observational design. The retrospective analysis of a de-identified dataset included 9,454 patients (18-100 years of age) who underwent a cardiothoracic procedure (coronary artery bypass graft, valve replacement, valve repair, wedge resection, or lobectomy) with providers at the outpatient clinic between 2014 and 2020. The dataset included the following variables of interest: age, gender, BMI, race, ASA score (representing comorbidity), surgery type, length of surgery, marker of 30-day readmission, days since surgery, and occurrence of 30-day readmission as the dependent variable. Data were explored descriptively to assess variability and normalcy before performing a time series analysis to evaluate trends in readmission rates.
Results: There was a statistically significant (p=<0.001) 6% decrease between average readmissions prior to and post program implementation. Patients with comorbidities are twice as likely to experience readmission than those with a low co-morbidity index [1.9 (1, .074), p =<.001]. Hospital readmission rates fall below the national average at 13.8% vs. 15.2% overall and 11.7% vs. 14.9% for CABG.
Conclusion: The time series analysis represents the highest level of observational evidence available, and in this case, suggests that a decrease in readmissions is associated with the implementation of a comprehensive patient education program by the outpatient clinic. The results of this evaluation contribute to the small body of evidence currently available regarding methods to reduce unplanned readmission rates among surgical patients and may be helpful to other surgical clinics who wish to improve their preventable 30-day readmission rates.
Implications for practice: High quality, patient-centered nursing care is essential to meeting national healthcare goals related to patients post-surgery. The implementation of a comprehensive educational program at one cardiothoracic clinic appears to be helping patients avoid unnecessary hospital readmissions following open heart surgery.
-

Reducing Specimen Labeling Errors to Promote Patient Safety: A Quality Improvement Project at an Inpatient Department in a Regional Acute Care Hospital
Jihye Johnson
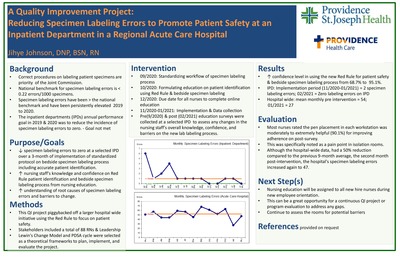
Background: Mislabeled specimen can cause patient harm by delaying treatment or by inappropriately administering treatment based on incorrectly assigned results. National patient safety goals have consistently called for a reduction of these errors in the hospital setting to zero. The specimen labeling errors on one inpatient department (IPD) at an acute care hospital in Eastern Washington were noted to be elevated from 2019 to 2020, potentially threatening patient safety. An evidence-based technique called the Red Rule has been linked to an improvement in lab labeling performance in the hospital setting.
Purpose/aims: The primary purpose of the QI project was to reduce specimen labeling errors in the identified IPD. The clinical question was, "In an IPD at a large acute care hospital, does implementing a standardized specimen labeling workflow, nursing education on the Red Rule, and updating monthly performance data with nursing staff, compared to usual care, reduce the occurrence rate of specimen labeling errors over 3-month period of implementation?"
Methods/Approach: The project lead collaborated with the Red Rule Advisory Committee to implement a Doctor of Nursing Practice (DNP) project focusing on the selected IPD. Interventions and data collection consisted of the following: (1) Standardizing workflow of specimen labeling process by the end of September 2020, (2) Formulating nursing education on the Red Rule by the end of October 2020, (3) Assigning nursing education to all RNs through an online learning platform to complete by the end of December 2020, (4) Sharing monthly data on specimen labeling errors from November 2020 to January 2021, and (5) Administering Pre- and post-interventions surveys in September 2020 and in February 2021 respectively to assess nursing staff perspectives on the new lab labeling process. Descriptive statistics was used for data analysis.
Results: A total of 32 nurses took the pre-intervention survey and indicated a low level of awareness and confidence on using the new Red Rule and lab labeling process. The biggest barrier on the new labeling compliance was lack of a pen in each patient room. A total of 41 nurses completed postintervention survey and reported increased confidence in using Red Rule and applying the new labeling process. Furthermore, the majority of nurses rated the pen placement in each workstation as moderately to extremely helpful for improving adherence. Following the intervention, the incidence of lab mislabeling errors on the IPD reduced significantly.
Conclusion: On the IPD, the implementation of an evidence-based Red Rule program was effective in reducing specimen labeling errors. The identification of the nursing-reported need for a pen in each patient room in order to effectively implement the new labeling process was a surprisingly simple yet powerful gap that was easily filled by this project.
Implications for practice: This project highlights the importance of assessing nursing perspectives on barriers to implementing change and supports that the Red Rule may be helpful in reducing lab labeling errors. Opportunities exist for future work to address gaps in following the new lab labeling process.
-

Team Up Against Sepsis: Six Tasks in Sixty Minutes
Karin Kloppel and Barbara Richards
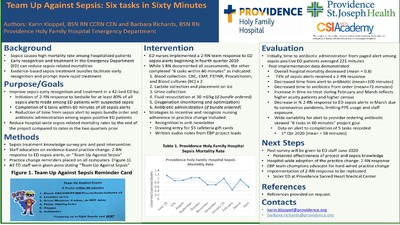
Background: Sepsis is the number one cause of mortality in hospitals nationwide. Our hospital system has identified sepsis mortality reduction as a top priority. Early recognition and treatment through improving sepsis bundle compliance was the selected focus in a 40-bed Emergency Department (ED) a community-based hospital.
Purpose: To evaluate the impact of a team response to sepsis alerts on sepsis outcomes in the ED in an acute care hospital.
Methods: Prior to implementing a team approach to sepsis alerts, ED staff were surveyed to describe awareness of SIRS and sepsis criteria and of sepsis bundle intervention metrics. Challenges identified were obtaining IV access, labs, 2 blood cultures, initiating IV fluid resuscitation and administering antibiotics in a timely manner. As a result, this quality improvement team created a team sepsis response, where two RNs respond to a room when a sepsis alert is called to "Team Up Against Sepsis". Together, the pair completes the following six evidence-based practice tasks within sixty minutes of the sepsis alert: 1) Blood collection: CBC, CMP, PT/INR, Procalcitonin, and Blood cultures x 2; 2) Lactate collected and placed on ice; 3) Urine collection; 4) Fluid resuscitation at 30 ml/kg; 5) Oxygen status is monitored/maximized; 6) Administer ordered antibiotic, if applicable. The pair will divvy up these six tasks including documentation to drive faster sepsis diagnosis and treatment. The quality improvement team educated nursing staff on using the new sepsis team response to every sepsis alert in the ED and also placed a card of the six sepsis tasks on all ED computers as a visual reminder of the project. Results: Pre-implementation was in the middle of the year 2019, and at that time, on average, the time from sepsis orders to antibiotic was 141.5 minutes; sepsis alert called to antibiotic administered was 221 minutes; blood culture order to collection was 53.32 minutes; IV fluids order to administration was 67.70 minutes. Post-implementation data was measured for the beginning of the year 2020 and all times decreased: Sepsis orders to antibiotic was 51 minutes on average; alert called to antibiotic was 79 minutes; blood culture order to collection was 59 minutes, and IV Fluids order to administration was 59 minutes. Last, there was a decrease in observed versus expected sepsis-related mortality from 1.15 at the beginning of the project to 0.66 at the post-implementation time point.
Conclusion: Teaming Up Against Sepsis had a positive impact in improving identification and treatment of sepsis in the ED with a significant reduction in observed versus expected sepsis related mortality rates. The team approach to sepsis alerts has been adopted as a best practice in this ED. Next steps include implementation of this approach at other ED’s within this hospital system and continual evaluation of sepsis outcomes.
-

Improving Primary Care Screening for Familial Hypercholesterolemia
Mary Nametka and Brenda Senger
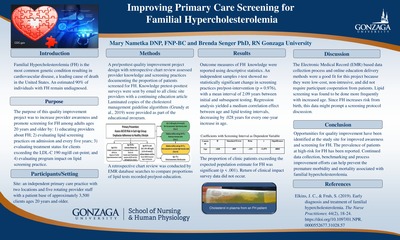
Background: Familial Hypercholesterolemia (FH) is the most common genetic condition resulting in cardiovascular disease, a leading cause of death in the United States. FH is estimated to affect 1 in 250 individuals with elevated lipid levels present from birth. An estimated 90% of individuals with FH remain undiagnosed. '
Purpose: The purpose of this quality improvement project was to increase provider awareness and promote screening for FH among adults ages 20 years and older. '
Methods: This quality improvement project consisted of an online educational intervention for providers working at an outpatient clinic regarding FH. Outcomes included: 1) pre-intervention lipid screening practices at the point of admission and every five years; 2) pre-intervention treatment status for clients exceeding the LDL-C 190 mg/dl cut-point; and 3) post-intervention lipid screening practice changes. Assessment of providers' FH knowledge occurred with author created surveys, and a retrospective chart review provided information on documentation of lipid screening practices as well as the proportion of patients screened for FH before and after the educational intervention.
Results: Outcome measures of FH knowledge were reported using descriptive statistics. An independent samples t-test showed no statistically significant change in screening practices pre/post-intervention (p = 0.976), with a mean interval of 2.09 years between initial and subsequent testing. Regression analysis yielded a medium correlation effect between age and lipid testing intervals, decreasing by .028 years for every one-year increase in age. The proportion of clinic patients exceeding the expected population estimate for FH was significant (p<.001). Return of clinical impact survey data did not occur.
Conclusions: Electronic Medical Record data identified undiagnosed patients in the clinic population at risk for FH. Knowledge surveys identified themes for further provider FH education.
-

Employed Mothers’ Satisfaction with the Breastfeeding Provisions in the Patient Protection and Affordable Care Act in Two Northwestern U.S. hospitals
Rebecca Penders
Background: Breastfeeding is the gold standard for infant nutrition. Many workplace barriers to lactation exist for mothers returning to work after the birth of an infant. In 2010 the Breastfeeding Provisions in the Patient Protection and Affordable Care Act (BP-PPACA) was enacted as the first federal breastfeeding law which outlined specifically break time and a place to pump for businesses with over 50 employees who employed hourly wage workers. There is little known about the satisfaction of hospital employees pumping/lactation experience after the BP-PPACA.
Purpose/Aims: The purpose of this study was to determine the extent to which employed mothers' perceived satisfaction in their breastfeeding experiences after the BP-PPACA. A major aim is to determine the extent to which the health policy allows employed mothers to combine breastfeeding and employment at two Northwestern U.S. hospitals since the 2010 law. Data were from self-reported breastfeeding initiation/duration and pumping experiences.
Methods/Approach: This 43-item survey in REDCap-Research Electronic Data Capture was exploratory and descriptive and sent out to all female employees at 2 hospitals in July 2020. The survey included demographic questions, occupation, as well as five Likert-scale satisfaction questions related to the experience with the BP-PPACA. Results: N=215 returned surveys from one large (over 500-bed) hospital and one medium (100-499 bed) hospital. Employees represented a variety of areas: administrate (non-clinical), clinical pharmacy, food service/dietary (other), phlebotomy/ other lab, EKG/other licensed techs, sterile processing, switchboard/ other communications, however most participants were from nursing. Most responses indicated satisfaction 1) with the BP-PPACA, 2) in their own breastfeeding duration and 3) exclusive use of breastmilk, however there were diverse positive and negative experiences 4) in the actual break time and 5) places to pump.
Conclusions: The BP-PPACA are a start for increasing breastfeeding in the U.S. among employed mothers however other policy considerations include support for PUMP for Mothers Act (S. 3170 and H.R.5592), and future building construction to include lactation spaces. Future research should explore paid maternity leave, on-site daycare/bring baby to work, occupational types, salaried employees, tax deductions for businesses for better workplace accommodations, ideal milk expression times for full milk expression and other satisfaction level research for whom these policies are aiming to support.
-

Pain Management Trends among Adults Hospitalized with Cellulitis: An Evidence-based Practice Project
Syndey Pham, Teresa Bigand, Brenda Senger, Kenn Daratha, and Kris Daratha
Background: Cellulitis is an infection of the skin causing swelling and acute pain. Two and a half to three and a half million adults seek care in the emergency department annually for this condition. Opioid medications are commonly administered and prescribed for pain, especially following the Joint Commission’s campaign in 2001 characterizing “pain as the 5th vital sign”. An estimated 22% of older adults hospitalized with a painful medical condition receive a new prescription for an opioid medication. Evidence suggests that there is no difference in pain outcomes among adults prescribed opioid versus non-opioid medications for acute pain conditions in the ambulatory setting. Conversely, outcomes favor the use of non-opioids, particularly acetaminophen and non-steroidal anti-inflammatories (NSAIDs), compared to opioids in the treatment of acute pain. Furthermore, best practice guidelines for acute pain management published in 2018 recommend maximizing the use of non-opioids and minimizing the use of opioids. In two acute care hospitals in the Pacific Northwest, prescription pain management for adults treated for cellulitis was previously unknown.
Purpose/aims: Our aim was to determine whether the rate of inpatient analgesics administered to manage pain related to cellulitis changed between the years 2014- 2020 at two acute care hospitals before and after local opioid stewardship efforts.
Methods/Approach: Data were extracted and de-identified from two hospitals in the Pacific Northwest for adults 18 years and older admitted with primary or secondary diagnosis of cellulitis between the years of 2014 and 2020 for a length of stay between 1-7 days. These data were retrospectively analyzed using descriptive statistics, chi-square analyses, and t-tests in excel.
Results:A total of 4,523 records met criteria were included in analysis. In the sample, rate of inpatient opioid administration significantly decreased from 91% to 73% (p
Conclusion: Opioid administration significantly decreased over time in our sample, and non-opioids, particularly acetaminophen, were frequently administered. In these two hospitals, it appears that local opioid stewardship efforts led to decreased opioid administration in alignment with best practice guidelines for managing acute pain for adults hospitalized with cellulitis. Future work should be done to compare pain management strategies over time for other acutely painful, non-surgical conditions treated in the hospital, and to characterize pharmacological pain management strategies post-hospitalization for an acutely painful, non-surgical conditions.
Implications for practice: Nurses should educate patients on best practice guidelines for pharmacological treatment of acute, non-surgical pain. Nurses could also advocate to prescribers to optimize non-opioid pain medications, particularly NSAIDS if patients meet criteria, to manage acute pain in the hospital setting.
-

Development of a SmartPhrase in the electronic health record to promote chemotherapy and immunotherapy safety
Mary Jo Sarver, Monica McManus, Amy Allen, Bethany Johnson, Dennielle Padgett, and Elizabeth Ser
Background: Chemotherapy-immunotherapies are high risk medications that can include multi-drug and multi-day regimens with narrow therapeutic indexes and high risk for toxicities. Susceptibility for errors exists if adherence to protocol is inconsistent or if pertinent patient specific information is omitted. Prior to the creation of the "SmartPhrase" in the Electronic HealthRecord (EHR) pre-administration safety checks were on paper, not included in the EHR, not standardized among clinicians, and not completed every time. Chart audits revealed a need for consistent, centralized documentation to enhance patient safety while minimizing professional liability. A trans-disciplinary team created a "SmartPhrase" template for streamlining relevant patient specific information and individualizing plans of care. The template created, included the nine components recommended by the Oncology Nursing Society (ONS) guidelines and recommendations for practice in correlation to chemotherapy-immunotherapy pre-administration checks. Purpose & Goal: Improve patient-centered care and transitions in care while standardizing chemotherapy-immunotherapy pre-administration documentation. Collaborate with inpatient and outpatient settings and service lines to have buy in and continuity related to content and location in the EHR. Ensure ONS recommendations for pre-administration checks included a documented dual verification process in the EHR. Methods: A baseline chart audit was conducted to determine if pre-administration safety checks were within the electronic health record. Based on findings a trans-disciplinary team of multiple stakeholders, including clinical informatics and bedside providers developed a "SmartPhrase" to promote rapid access to critical information. Safety checks included "hard stops" in the "SmartPhrase" template. Formalized education for providers included emails, posters, huddle presentations, job aids, and face-to-face classes with return demonstration and validation of comprehension and usage. Post implementation a three-month EHR audit was preformed, and feedback was solicited from end users to identify opportunities for improvement which lead to template revisions. Re-educated was initiated based on template modifications. Six-month audits re-evaluated usage and completion of documentation. Upon completion of the project the "SmartPhrase" was incorporated into new hire orientation. Results: Practitioner utilization of the "SmartPhrase" exceeded the project goal of 95% after implementation. Change from baseline use of "SmartPhase" documentation were noted in the following specific key areas: dual verification (↑100%),diagnosis and protocol (↑69%), drugs (maintained 100% utilization), consent (↑54%), patient education (↑37%), blood return from venous access device (↑29%), dosages (↓6%), initial labs (↓6%), schedule (↑3%). Implications for practice: Nurses need to be actively involved in identifying barriers to care delivery to improve safety by initiating quality improvement projects. A defined location for the "SmartPhrase" in the EHR made for easy access between shifts and future encounters to enhance patient centered care based on clinical status at time of treatment as well as ongoing treatment tolerance. The "SmartPhrase" allowed consistent documentation and dual verification of pre-administration safeguards. Implementing tools within the EHR based on standards and guidelines decreases organizational liability concerns while promoting safety. Completing the "SmartPhase" in advance supports stewardship of resources including nursing expertise/time, delays in treatment (bed/chair availability, admission/appointment time), and medication/supply cost. Many organizations and healthcare systems utilize Epic® EHR systems which offer "SmartPhrases" that can be shared within an individual facility and/or network of healthcare delivery systems. Standardized documentation promotes continuity of patient centered care in the EHR for ease of retrieval across oncology patient's initial, ongoing and follow up treatment
-

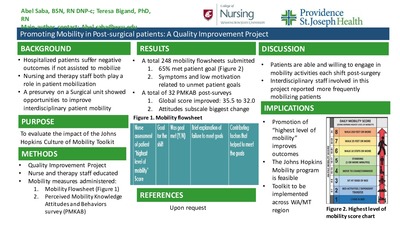
Promoting Mobility in Post-Surgical Patients: A Quality Improvement Project
Abel Sawa and Teresa Bigand
Background: Hospitalized patients suffer negative outcomes related to lack of mobilization activities such as falls with injury or infection. Mobility requires a multi-disciplinary team approach including Registered Nurses (RNs), Certified Nursing Assistants (NA-Cs), and Physical/Occupational Therapists (PT/OTs) to promote best patient outcomes. The Johns Hopkins Culture of Mobility toolkit provides evidence-based practices for integrating multi-disciplinary mobilization efforts for hospitalized patients. This toolkit had not been implemented on a busy orthopedic post-operative nursing unit in one large hospital.
Purpose/aims: To test the impact of the culture of mobility toolkit on caregiver perceptions of mobility barriers and evaluate the implementation of the toolkit on a surgical acute care unit.
Methods/Approach: This quality improvement project was implemented on an orthopedic post-surgery inpatient unit in a large medical center in the Pacific Northwest. A pre-survey was administered to RNs, NA-C's and PT/OTs prior to the implementation of this project, and those findings guided the development of an educational intervention. The education was a poster on the Johns Hopkins Culture of Mobility toolkit with focus on using the toolkit's mobility screening tool presented to RN's, NAC's and PT/OT's. Caregivers were also informed to complete a form each shift on the following: the patient's Highest Level of Mobility score, the patient's mobility goal for the shift, whether the patient met the personal goal, and barriers/facilitators to the patient's ability to meet personal goals. Staff were directed to complete tracking sheets each shift for each patient during a 6-week period. After the intervention, all staff were invited to complete the post-survey to re-assess perceived mobility barriers.
Results: More than 90 caregivers completed the pre-intervention perceived mobility barriers survey, which suggested that staff felt that patient mobilization efforts were time-intensive and posed an injury risk for caregivers. After the education was provided, over 240 mobility tracking sheet were submitted by mainly RN's working night shift, and 65% of caregivers reported that the patient's self-reported mobility goal was met by the end of the shift. Barriers to achieving patient-created mobility goals included inadequate symptom management, reduced patient-specific motivation to move, and lack of adequate resources to safely mobilize patients. A total of 32 caregivers responded to the post-project mobility survey, revealing a significant decrease in overall perceived mobility barriers from pre-intervention levels. PT/OTs reported significantly less barriers compared to nursing staff at both time points.
Conclusion: This project demonstrated that multi-disciplinary staff working on a busy orthopedic post-surgical floor can adopt evidence-based practice tools to promote mobility which may facilitate increased patient mobilization activities. Future projects may include greater adoption of the toolkit throughout the medical center.
Implications for practice: Hospital-based mobility programs such as the Johns Hopkins Culture of Mobility toolkit can mitigate functional decline of adults following hospitalization. Inpatient mobility activities may be enhanced by engaging patients to set and attain mobility goals each shift, partnering with PT/OTs, identifying patient motivation to mobilize, and optimizing symptom management.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}