
-
 In Acute Chest Syndrome by Natalie Bolton, MD and Omar Pandhair")
Extracorporeal Membrane Oxygenation (ECMO) In Acute Chest Syndrome
Natalie Bolton, MD and Omar Pandhair
Introduction: Acute chest syndrome (ACS) is a severe complication of sickle cell disease. Rarely, it may progress to acute respiratory distress syndrome (ARDS). Inability to oxygenate despite mechanical ventilation necessitates consideration of extracorporeal membrane oxygenation (ECMO). Case Summary: A 31-year-old man with sickle cell disease presented with low back pain similar to prior pain crises. Vital signs were normal, and his hemoglobin level was 10.2 g/dL, with a reticulocyte index of 0.05. He was admitted for pain control and rehydration. That night, he developed fever, tachypnea, and hypoxemia with imaging showing a right lower lobe infiltrate, consistent with ACS. He was treated with broad-spectrum antibiotics and escalated to high flow nasal cannula. Hematology recommended transfer to a center capable of exchange transfusion, and he was admitted to the intensive care unit in the interim. Repeat hemoglobin level decreased to 8.0 g/dL and a stat transfusion was ordered. Despite noninvasive ventilation, he remained hypoxemic and endotracheal intubation was performed; however, he remained hypoxemic and suffered a cardiac arrest with successful resuscitation within three minutes, though he developed shock. His hemoglobin level rapidly dropped to 4.3 g/dL. He received multiple transfusions and vasopressor support and remained persistently hypoxemic and with worsening lactic acidosis. He was found to have severe right heart failure on echocardiography and underwent placement of a Protek Duo right ventricular assist device before transferring to a tertiary center. Continuous renal replacement therapy was started and despite transition to veno-arterial-venous ECMO for new onset left ventricular failure, he suffered a ventricular tachycardia arrest and expired. Discussion: This case highlights the need for early recognition and management of both acute vaso-occlusive crisis requiring transfusion support and refractory ARDS potentially needing ECMO. Our patient’s hemoglobin level was not re-checked until he arrived in the ICU, by which time it dropped significantly. Earlier supportive transfusion may have provided benefit, targeting a goal hemoglobin level of at least 10g/dL. Employment of ECMO for management of ACS is rare, and limited data suggests cohorts including adults have a lower survival rate compared to exclusively pediatric cases (27% vs. 52%). Due to this rarity, there are no official guidelines on if or when to use ECMO in ACS. With advances in this therapy, including awake ECMO, we advocate for further study to determine whether earlier initiation of ECMO may be beneficial in saving the lives of young, otherwise healthy sickle cell patients such as ours.
-

GLP-1 Medication Risk Assessment
Brendan Bu, PharmD
GLP‑1 receptor agonists are increasingly prescribed across diverse clinical settings. As overall utilization of these drugs increase, there has also been an associated uptick in reported patient safety concerns. Some of these reports have been associated with unconventional dosing schedules, product transitions, and evolving therapeutic uses. To assess these risks within PMG Oregon, a Common Cause Analysis (CCA) was conducted to evaluate all GLP‑1– related medication safety events reported between September 2023 and September 2025. A total of 27 events were identified, including near misses, precursor events, and patient‑reaching errors, and were analyzed by event type, MERP stage, contributing human factors, and system-level vulnerabilities. Most safety events originated during the prescribing or ordering stage, highlighting early workflow vulnerabilities related to incorrect dose selection, titration errors, and inappropriate starting doses when switching GLP‑1 products. Dispensing events represented the second most common category, while transcription errors occurred less frequently. These errors resulted in a range of patient outcomes—from no harm to significant gastrointestinal illness, dehydration, acute kidney injury, and emergency department visits. Human factor analysis demonstrated that consciousness-related lapses (IE: slips, inattention, interruptions) were the most frequently reported contributors, followed by critical thinking and competency-related errors. System-level contributors were dominated by policy and procedure gaps, process breakdowns, and technology limitations such as inappropriate EHR defaults and lack of automated guardrails. Issues related to storage and handling of Medication Assistance Program (MAP) products further reflected workflow vulnerabilities at individual clinics. Unfortunately, limited or incomplete documentation within the HRP events limits the ability to assess and identify patterns and characteristics fully. However, the analysis shows that GLP‑1 medication errors arise from intersecting human, workflow, and system factors. Opportunities for improvement include standardizing titration workflows, implementing EHR‑based safeguards, strengthening MAP handling processes, and clarifying caregiver roles to create a safer prescribing environment for GLP‑1 therapies. (IRB Exempt)
-
Evaluation of blood culture contamination: impact on antibiotic use and clinical outcomes
Natalie Hart, PharmD; Nyles Fowler; and Emily Fox
Abstract: Blood cultures are one of the most frequently ordered microbiological tests in the hospital. While this diagnostic tool is necessary for determining management of certain infections, contaminated samples often lead to unnecessary antibiotic administration. Blood culture contamination is a critical aspect of antimicrobial stewardship, as previous literature has shown that treatment of a blood culture contaminant is associated with increased hospital costs, length-of-stay, morbidity, and mortality rates. To better understand the impact of blood culture contamination on patients within our facility, we evaluated antibiotic use and other patient outcomes associated with contaminated blood cultures. This was a single-center retrospective cohort study at a tertiary care hospital. Adult patients with two sets of blood cultures drawn within 24 hours of presentation to the hospital from March to August 2025 were screened for inclusion. Patients were excluded if only one set of blood cultures is drawn, if patient was not admitted to hospital, if true-positive blood culture not meeting microbiological contaminant definition, or neutropenic defined as absolute neutrophil count less than 500 cells/uL. The primary outcome was overall days of inpatient antibiotics in patients with contaminated blood cultures in comparison to patients with negative blood cultures. Secondary outcomes included in-hospital mortality, hospital length-of-stay, incidence of repeat blood cultures obtained, incidence of antibiotic escalation (addition of anti-MRSA therapy), and transthoracic echocardiograms performed. Patients were identified utilizing the electronic health record (EHR) and chart review was performed to record patient demographics (age, sex, BMI), patient characteristics (comorbidities, infection type), and evaluate the primary and secondary outcomes. Statistical analysis was performed utilizing student t-tests for continuous variables, chi-squared tests for categorical variables. A P-value of less than 0.05 was considered statistically significant. Results and conclusions will be shared when the project is completed. (IRB approved) Learning Objectives: Describe and evaluate clinical outcomes associated with contaminated blood culture results. Presentation Category: Antibiotic Stewardship
-
GENT-le Dosing: Evaluating the Safety of Gentamicin at Higher Doses for Late Preterm and Term Neonates
Jason Hector, D. Erin Wilson, Aiyana Ooki-Knutson, and Jennifer Conley
Abstract: In June 2024, Providence St Joseph Health updated the standard gentamicin dose in the Pediatric and Neonatal Aminoglycoside protocol from 4 mg/kg to 5 mg/kg every 24 hours for late preterm and term neonates. This project aims to evaluate late preterm and term neonatal patients who received gentamicin for empiric sepsis coverage within the first seven days of life, at 4 mg/kg/dose or 5 mg/kg/dose, to assess the safety of the standardized 5 mg/kg dosing for late preterm and term neonates after the protocol change. This study is a multicenter retrospective pre-/post-intervention analysis at a multistate health system spanning 51 hospitals. Term neonatal patients who received either 4 mg/kg/dose every 24 hours or 5 mg/kg/dose every 24 hours for empiric sepsis will be included. Further inclusion criteria include receipt of at least one dose of gentamicin, gestational age of at least 35 weeks, and delivery at a hospital within the Providence St Joseph Health system. The pre-intervention group will include patients who meet inclusion criteria that were born from October 1, 2022, through September 30, 2023, while the post-intervention group will include qualifying patients born from October 1, 2024 to September 30, 2025. Primary endpoints include urine output and urine occurrences per 24 hours for a 4-day period following the first dose of gentamicin. Secondly, endpoints include daily serum creatinine values when available and duration of gentamicin dosing. Serum gentamicin levels are not routinely collected in this patient population, as duration of therapy is often limited, and standard practice is to avoid drawing blood when not entirely necessary. For patients who received gentamicin long enough to warrant drawing a trough and/or peak, a subgroup analysis will be performed to evaluate if the higher dosing regimen resulted in significantly higher levels. This will be evaluated not only based on numeric serum concentration values reported but also based on the incidence of sub- and supra-therapeutic levels. Descriptive statistics will be used to describe the baseline characteristics of the study population. A p-value of less than 0.05 will be considered statistically significant. Results and Conclusions will be reported and shared when the project is complete. (IRB approved) Learning Objectives: Describe the difficulties of gentamicin dosing in late preterm and term neonates. Evaluate the safety of gentamicin when dosed at 4 mg/kg/dose vs 5 mg/kg/dose for late preterm and term neonates. Presentation Category: Pediatrics and Neonates
-
Emergency department prepack implementation at Providence Portland Medical Center
Bowei Liu PharmD; Jessica Dizon Scheer; and Mac Ovenell, PharmD, MS
Introduction: Providence Portland Medical Center (PPMC) implemented a multiphase ‑quality improvement‑ project to standardize the emergency department (ED) prepack program with the Providence Oregon region. Background/Purpose: Prior to the project, ED prepack dispensing lacked a uniform process; individual sites stored and labeled medications differently, reconciliation was paper based, and staff were unclear on regulatory limits. Oregon Board of Pharmacy rules allow prepack medications for outpatient use only when the supply does not exceed a ‑48-hour‑ course, with limited exceptions. Each prepack must also carry a unique serial number, and a label specifying the hospital’s pharmacy’s contact information, drug name and strength, manufacturer, expiration date, and other required elements. To bring PPMC into alignment with the regional standard operating procedure, the team established a structured program that encompassed formulary alignment, translation/accessibility improvements, and a reconciliation process. Methods: In Phase 1, pharmacy informatics specialists (RXI) and operations staff compared PPMC’s medication list to the approved Oregon ED prepack formulary. For each prepack, the electronic prescribing (ERX) build in Epic was reviewed and modified to ensure that the ERX identifier, the custom National Drug Code (NDC), and the automated dispensing system (Pyxis) entries matched exactly. A secure storage area was designated in the ED and prepacks were labeled with date b‑ased serial numbers as described in the policy, ensuring that documentation in the medication administration record captured the unique prepack number, drug details, and prescriber information. In Phase 2, the team discovered a knowledge gap: central pharmacy staff were unfamiliar with how to use Epic translation functions and TelRx to support patients with limited English proficiency‑ or visual impairments. Finally, because each facility had been reconciling prepack usage differently, the project created a reconciliation process from scratch. Paper reconciliation was replaced by an electronic method. Results: Phase 1 led to accurate ED prepack orders from Epic to Pyxis and a consistent formulary list with the OR region. Phase 2 improved staff knowledge in translation and TelRx. Preliminary reconciliation data show that documentation errors improved from 20-30% to less than 5%. Additional outcome measures such as staff feedback, workflow efficiency, and medication error rates will be assessed; final results will be presented at the conference. Conclusions: Standardizing the ED prepack program required aligning the local formulary and dispensing systems with regulatory expectations, addressing communication and accessibility barriers, and instituting a working reconciliation process. The project demonstrates that electronic tools, staff education, and process redesign can bring PPMC’s ED prepack practices into compliance with Oregon administrative rules and a regional standard operating procedure. Future work will evaluate long-term‑ effects on patient safety and operational efficiency. IRB status: Exempt
-
Short duration antimicrobial therapy for non-staphylococcal Gram-positive bacteremia (SHORT-STOP)
Mason Melbuer, PharmD; Gregory B. Tallman, PharmD, MS, BCPS, BCIDP; Emily Fox; and Soraya Hobart, PharmD
Recent clinical trials have demonstrated non-inferiority of shorter antibiotic courses for many infections, including gram-negative bacteremia. Longer courses were associated with numerically fewer deaths in the gram-positive subgroup of the BALANCE trial; however, only ~15% of the cohort had streptococcal or enterococcal bacteremia. Conversely, other retrospective studies have demonstrated comparable mortality in uncomplicated streptococcal or enterococcal bacteremia but many of these studies targeted narrow populations, limited pathogens, or were susceptible to confounding variables. The purpose of this study is to determine if patients with uncomplicated non-staphylococcal gram-positive bacteremia can be safely managed with short course antimicrobial therapy. This is a retrospective, multicenter cohort study examining adult (age >= 18 years) patients admitted for an uncomplicated non-staphylococcal gram-positive bloodstream infection blood stream infection from 9/1/2024 to 9/1/2025 at 8 hospitals within a multistate health system. Patients were excluded if they were diagnosed with an active infection requiring prolonged duration of therapy (eg. endocarditis, osteomyelitis), presence of prosthetic material or endovascular grafts, if blood cultures suggest contamination, or if diagnosed with polymicrobial bacteremia. The primary outcome was 30-day all-cause mortality. Secondary outcomes include recurrent bacteremia and Clostridioides difficile infections; all outcomes were assessed at 30 and 90 days. Patient sex, age, ethnicity, comorbidities, organism identified, length of hospital stay, source of infection, and formal infectious disease consult will be collected as well. Patient characteristics were summarized with descriptive statistics. Differences between short and long course therapy were compared using chisquare, Fisher’s exact, Wilcoxon rank-sum, and Student’s t-tests as appropriate. Multivariable logistic regression will be used to model the relationship between treatment duration and outcome, with results reported as odds ratios and associated 95% confidence intervals. Variable selection was determined a priori based on expert input. Approximately 693 patients were examined; preliminary data was collected through electronic extraction and manual chart review of patients’ electronic health records. Approximately 61.6% of patients were male and the most common organisms isolated were Streptococcus pyogenes, Streptococcus pneumoniae, and Enterococcus faecalis. Full results and conclusions will be shared when the project is completed. The study was determined to be exempt from IRB review. Learning objective: Identify the optimal antimicrobial duration in those diagnosed with uncomplicated, non-staphylococcal, Gram-positive bacteremia. Category: Infectious disease
-
Evaluation of SAVED/IMPEDE risk assessment models for VTE prophylaxis in multiple myeloma patients
Rina Mullendore, PharmD and Ian Ingram, PharmD, BCOP
Abstract: Venous thromboembolism (VTE) is a significant complication in patients with multiple myeloma. The National Comprehensive Cancer Network (NCCN) Multiple Myeloma guidelines recommend administering VTE prophylaxis for eligible patients if there are no contraindications to anticoagulation or antiplatelet agents. Current VTE prophylaxis recommendations are guided by the SAVED and IMPEDE scores, which are tools used to predict the risk of VTE in patients with multiple myeloma. The primary purpose is to determine the incidence of VTE, stratified by IMPEDE/SAVED score, in patients with multiple myeloma receiving treatment at Providence Cancer Institute Franz Clinic. EPIC will be queried using SlicerDicer to identify patients diagnosed with multiple myeloma who are actively receiving treatment at Providence Cancer Institute Franz Clinic. Exclusion criteria include research participants, patients already on an anticoagulation or antiplatelet agent for other prescribed indications, and patients not being actively treated for multiple myeloma. A report will be generated that includes potential patients for study inclusion. Additional reports will be generated to identify patients who have a VTE diagnosis, on aspirin or an anticoagulation agent, and other variables that are important for IMPEDE/SAVED score calculation such as age, immunomodulatory drug therapy, Asian race, BMI, pelvic/hip/femur diagnosis, surgery within the last 90 days, erythropoiesis-stimulating agents, dexamethasone dose, doxorubicin, tunneled line or central venous catheter, and existing thromboprophylaxis (therapeutic or prophylaxis). The IMPEDE/SAVED score will be calculated for patients to identify whether patients were on an appropriate prophylactic agent, indexed to their Cycle 1, Day 1 treatment, based on the calculated IMPEDE/ SAVED score per NCCN guidelines. For patients with a VTE diagnosis, it will be determined if the VTE occurred before or after the initiation of multiple myeloma treatment. Adverse events related to VTE prophylaxis (clinically relevant bleeding) will also be reported. IRB status is exempt. Data is currently being collected. Results and conclusions will be shared when the project is completed. Presentation category: Hematology/oncology/immunology/transplant
-
Impact of restricting medication auto-verification on patient safety in the emergency department
Anthony Nguyen, PharmD; Savita Bathija, PharmD, BCEMP; and Jessica Dizon-Scheer, PharmD, MHA, BCPS
Abstract: When Providence Portland Medical Center (PPMC) first transitioned to an electronic health record system, most Emergency Department (ED) medication orders were signed by licensed prescribers and bypassed pharmacist review. Only a small list of high‑risk medications required pharmacist verification prior to dispensing. While this workflow supported rapid medication availability, it also introduced potential patient‑safety risks due to limited pharmacist oversight. In August 2024, PPMC revised its ED medication verification policy. Under the new process, nearly all medications require pharmacist review before dispensing, with exceptions for a small group of low‑risk, time‑sensitive emergent agents that may still be auto‑verified. This change aimed to enhance medication safety while preserving ED efficiency. However, the impact of this policy shift has not been evaluated. This IRB‑approved, single‑center pre–post observational study assessed the effects of this revised process. A preliminary review of reports from Providence’s medication event reporting system identified ceftriaxone as the medication most frequently associated with safety events at PPMC’s ED. We included and compared ED ceftriaxone orders for adults (≥18 years) that were auto‑verified between August 2023–August 2024 and pharmacist‑verified ceftriaxone orders between August 2024–August 2025. Orders were excluded if the patient did not receive ceftriaxone in the ED or was younger than 18 years from our analysis. Primary outcomes included surrogate safety measures: total medication safety events associated with ceftriaxone pre and post revised verification process. Secondary outcomes included ceftriaxone safety events per 1,000 medication orders or ED visits, safety event type (duplication, incorrect dose, incorrect indication, incorrect timing), number of number of documented pharmacist antimicrobial stewardship interventions number and percentage of ED orders prospectively reviewed by a pharmacist, and time from verification to ceftriaxone administration pre and post implementation. This study is currently ongoing. Results and conclusions will be shared when the project is completed. Presentation Category: Medication safety/quality improvement
-
Evaluating the clinical, operational, and financial opportunities for developing a pharmacist-led iron infusion clinic
Yasasvi Obeyesekera, PharmD; Stephanie Matta, PharmD, BCOP; and Shuntao Cai, PharmD
-

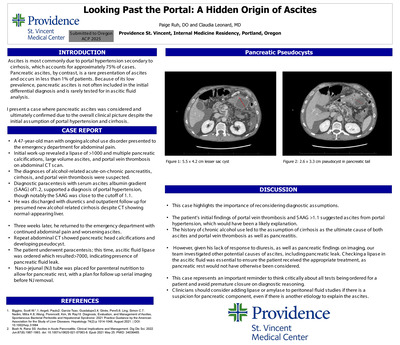
Looking Past the Portal: A Hidden Origin of Ascites
Paige Ruh, DO and Claudia Leonard, MD
Introduction: The most common cause of ascites is portal hypertension secondary to cirrhosis and accounts for nearly 75% of cases. In contrast, pancreatic ascites is a rare presentation of ascites and occurs in less than 1% of patients. Because of its low prevalence, pancreatic ascites is often excluded from the initial differential diagnosis and rarely assessed in ascitic fluid analysis. This is a case in which pancreatic ascites was considered and ultimately confirmed based on the overall clinical picture, challenging the initial assumption of portal hypertension and cirrhosis. Case Presentation: A 47-year-old man with ongoing alcohol use disorder presented to the emergency department with abdominal pain. Initial work-up revealed a lipase >1000 U/L, multiple pancreatic calcifications, large-volume ascites, and portal vein thrombosis on abdominal CT scan. A diagnosis of alcohol -related acute-on-chronic pancreatitis, cirrhosis, and portal vein thrombosis were suspected. Diagnostic paracentesis showed a serum-ascites-albumin gradient (SAAG) of 1.2, supporting portal hypertension, though notably close to the cutoff of 1.1. He was discharged on diuretics and outpatient follow-up for presumed new alcohol related cirrhosis despite CT showing normal-appearing liver. Three weeks later, he returned with persistent abdominal pain and worsening ascites. Repeat CT demonstrated pancreatic head calcifications and a developing pseudocyst. A second paracentesis was performed, and ascitic fluid lipase was ordered, resulting >7000 U/L-- confirming a pancreatic fluid leak. A nasojejunal (NJ) tube was placed for enteral nutrition to allow pancreatic rest, with plans for serial imaging prior to NJ removal. Discussion: This case highlights the importance of reconsidering diagnostic assumptions and recognizing cognitive biases. The patient’s initial findings of portal vein thrombosis and SAAG >1.1 suggested ascites from portal hypertension. The history of chronic alcohol use led to the assumption of cirrhosis as the ultimate cause of both ascites and portal vein thrombosis, with ongoing alcohol use to explain pancreatitis. However, his lack of response to diuresis, as well as pancreatic pseudocysts on imaging, our team investigated other potential causes of ascites, including pancreatic leak. Checking a lipase in the ascitic fluid was essential to ensure the patient received the appropriate treatment, as pancreatic rest would not have otherwise been considered. This case represents an important reminder to think critically about all tests being ordered for a patient and avoid premature closure on diagnostic reasoning. Clinicians should consider adding lipase or amylase to peritoneal fluid studies if there is a suspicion for pancreatic component, even if there is another etiology to explain the ascites
-
Financial impact of hepatitis B screening for subsequent chemotherapy
Shaye Suzuki, PharmD and Shuntao Cai, PharmD, BCOP
Abstract: The American Society of Clinical Oncology (ASCO) released an opinion that all patients on systemic anticancer therapy should be tested for hepatitis B virus (HBV) but gave no formal guidance on additional HBV testing if the initial HBV test is negative. It is unknown whether performing these tests is resulting in significant costs. The aim of this retrospective chart review is to determine the cost associated with HBV testing through various definitions of “unnecessary testing”. The rates of new potentially actionable HBV tests during retesting defined by HBV core antibody and surface antigen positive will also be determined. This is a multi-center, retrospective chart review that was performed across 4 Providence Health Plan oncology clinics in Oregon. Electronic medical records of patients with a chemotherapy treatment plan between May 2025-July 2025 were reviewed. The data collected were demographics (age, gender, ethnicity, type of cancer), HBV test results (for all tests performed), line of treatment (1st, 2nd, 3rd , etc), time each test was taken, and the use of a CD20 chemotherapy medication. For the results, the cost per test was multiplied by the number of tests that were determined to be unnecessary, through various definitions, and compared to the cost of all tests performed. Rates of new potentially actionable HBV tests were also calculated. A total of 565 patient charts were reviewed, and there were 265 new hepatitis B tests performed. This correlates to a cost of $25,600. On average, the time between treatments, when a new test was performed, was about 25 months compared to about 10 months between treatments when new tests were not done. When looking at patients who had a potentially actionable hepatitis B test result, there were 5 total patients (< 1%) who were not on CD20 therapy that had a new potentially actionable HBV test. Of these 5 patients, there were no consistent patterns in patient demographics, chemotherapy regimen, or type of cancer that would increase one’s risk of having a new potentially actionable HBV result. From this data, we cannot recommend changing the current practice regarding repeating hepatitis B testing. The inherent risk of having a new potentially actionable hepatitis B result still exists for all patients, on CD20 therapy or not. The monetary cost of missing a new potentially actionable result and the complications that may arise leading to a hospital admission outweigh the cost of our current practice for repeat HBV testing. (IRB exempt) Learning Objectives: Determine the financial impact of subsequent HBV testing through various definitions of “unnecessary testing”. Presentation Category: Medication Safety/Quality Improvement
-

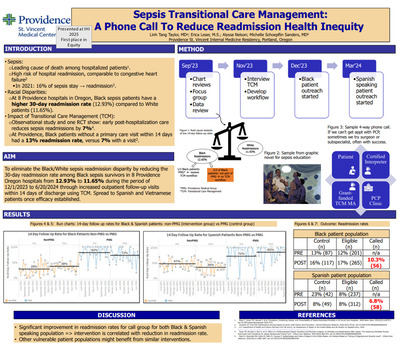
Sepsis Transitional Care Management: A Phone Call to Reduce Readmission Health Inequity
Linh Tang Taylor, MD; Erica Leser, MS; Alyssa Nelson; and Michelle Schopeflin Sanders, MD
Introduction: Sepsis accounts for 52% of hospital admissions in the United States and is the leading cause of death among hospitalized patients1 . However, disparity exists among sepsis survivors with race being reported as a determinant of recovery2 . Such disparity exists in Providence Oregon 8 hospitals: Providence Black patients have higher sepsis readmission rates than White (12.93% vs 11.65%). Using modified community-based participatory research, data analysis, and stakeholder interviews, we identified one potential root cause of the disparity: Black patients being readmitted are not receiving our system's Transitional Care Management (TCM) services. We aim to eliminate the Black/White sepsis readmission disparity by reducing the 30-day readmission rate among Black sepsis survivors in 8 Providence Oregon hospitals from 12.93% to 11.65% during the period of 12/1/2023 to 6/20/2024 through increased outpatient follow-up visits within 14 days of discharge by delivering TCM intervention to those who are not eligible for one with our health system. Methods: In PDSA 1, a resident physician & nurse coordinator delivered TCM phone call intervention for Black sepsis patients who don’t qualify for the system TCM intervention due to insurance status. With these phone calls, patients are reminded to follow up with their PCP, finish their antibiotics, and given sepsis education material via either MyChart or mail delivery. If patient doesn’t have a PCP, we referred them to a federally qualified health center to get established, or to a free clinic. In PDSA 2, 1 medical student and 1 Spanish-speaking grant-funded medical assistant are added to the team to continue delivering intervention to Black sepsis patients. With Spanish-speaking patients, we helped them navigate complex phone trees of clinic that are sometimes only in English. Results: Results showed improvement in 14-day follow up rates for Black patients population (up to 38% from 28%) but not for Spanish-speaking patient population (down to 36% from 47%). Readmission rate increased significantly for both groups: readmission rates for the intervention group for Black patients decreased to 10.3% from 16%. Readmission rate for the intervened group for Spanish-speaking patients decreased to 6.8% from 8%. Conclusion: Promising results in reducing sepsis readmission rates for both Black and Spanish-speaking patients is an indication that TCM intervention may be correlated with reducing sepsis readmission health inequity.
-
Evaluation of patient outcomes after implementation of remdesivir restriction criteria
Evonie Claire Villarete, PharmD; Emily Fox, PharmD, BCIDP; and Gregory B. Tallman, PharmD, BCPS, BC
Abstract: Remdesivir has demonstrated inconsistent clinical benefit in randomized trials, with the greatest efficacy observed in hospitalized patients requiring low-flow oxygen and no clear mortality benefit in patients requiring invasive mechanical ventilation. In the era of widespread SARS-CoV-2 immunity, evolving viral variants, and reduced disease severity, the role of routine remdesivir use remains uncertain. Continued prescribing may expose patients to unnecessary therapy, prolong hospitalization, and increase healthcare costs without clear incremental benefit. In June 2025, Providence Oregon hospitals implemented restriction criteria limiting remdesivir use to selected high-risk populations, including elderly, immunocompromised, or critically ill patients presenting within seven days of symptom onset. The purpose of this study is to evaluate the clinical and financial impact of implementing remdesivir restriction criteria across Providence Oregon hospitals. This study is a multi-center retrospective cohort analysis of adult patients hospitalized with nasopharyngeal PCR confirmed SARS-CoV-2 identified through the electronic medical record. Patients hospitalized at one of eight Providence Oregon hospitals between July 15, 2024 and October 15, 2024 (pre-restriction period) and July 15, 2025 and October 15, 2025 (post restriction period) were included to allow comparison of outcomes before and after the intervention. Demographic, clinical, and treatment data were collected through chart review. Variables collected include age, sex, body mass index, race or ethnicity, oxygen saturation, oxygen device, baseline vital signs, immunocompromised status, comorbidities, days from symptom onset, intensive care unit admission status, medications (corticosteroids, remdesivir, and antibiotics), vaccination status, prior SARS-CoV-2 infection, and presence of sepsis at admission. The primary outcome is the need for supplemental oxygen or escalation in home oxygen therapy requirements. Secondary outcomes include hospital length of stay, intensive care unit admission, mechanical ventilation, 30-day readmission, in-hospital mortality, adherence to the restriction policy, and financial impact associated with remdesivir utilization. Continuous variables will be analyzed using Student’s t-test or Mann-Whitney U test, and categorical variables will be analyzed using chi-square or Fisher’s exact tests as appropriate. Results and conclusions will be shared when the project is completed. (IRB exempt) Learning Objective: Assess the clinical and financial impact of recently implemented remdesivir restriction criteria. Presentation Category: Infectious Diseases
-

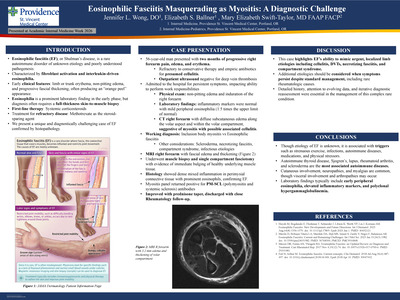
Eosinophilic Fasciitis Masquerading as Myositis: A Diagnostic Challenge
Jennifer L. Wong, DO; Elizabeth S. Ballner, DO; and Mary Elizabeth Swift-Taylor
Introduction: Eosinophilic fasciitis (EF), or Shulman’s disease, is a rare disorder of unknown etiology and poorly understood pathogenesis. It is characterized by fibroblast activation and interleukin-driven eosinophilia. Early clinical features include limb or trunk erythema, non-pitting edema, and progressive fascial thickening, often producing an “orange peel” appearance. Eosinophilia is a prominent laboratory finding in the early phase, but diagnosis often requires a full-thickness skin-to-muscle biopsy. Systemic corticosteroids are first-line therapy, with methotrexate as the steroid -sparing agent for refractory disease. We present a unique and diagnostically challenging case of EF confirmed by histopathology. Case Presentation: A 56-year-old man presented with two-months of progressive right forearm pain, edema, and erythema refractory to conservative therapy and empiric antibiotics for presumed cellulitis. An outpatient ultrasound excluded deep vein thrombosis (DVT) and worsening symptoms prompted hospital admission. Examination revealed non-pitting edema and induration of the right forearm; inflammatory markers were normal and mild peripheral eosinophilia (1.5 times the upper limit of normal) was noted. CT showed diffuse subcutaneous edema along the volar aspect of his right forearm. Necrotizing fasciitis and compartment syndrome were considered but deemed unlikely given benign clinical findings by General and Orthopedic Surgery. His workup included evaluation for myositis, eosinophilic fasciitis, and scleroderma, among other diagnoses. MRI demonstrated fascial edema and thickening, resulting in a muscle biopsy and single compartment fasciotomy with evidence of immediate bulging of healthy underlying muscle tissue. Histology showed dense mixed inflammation in perimysial connective tissue with prominent eosinophils, confirming EF. Lastly, his myositis panel returned positive for PM-SCL antibodies. The patient improved on a prednisone taper and was discharged with close Rheumatology follow-up. Discussion: Though the etiology of EF is unknown, it is associated with triggers such as strenuous exercise, infections, autoimmune diseases, medications, and physical stressors. Autoimmune thyroid disease, Sjogren’s, lupus, rheumatoid arthritis, and scleroderma are the most associated autoimmune diseases to EF. Cutaneous involvement, neuropathies, and myalgias are common, though visceral involvement and arthropathies may occur. Laboratory findings typically include early peripheral eosinophilia, elevated inflammatory markers, and polyclonal hypergammaglobuline mia. This case highlights EF’s ability to mimic urgent, localized limb etiologies including cellulitis, DVTs, necrotizing fasciitis, and compartment syndrome. Additional etiologies should be considered when symptoms persist despite standard management, including rare rheumatologic causes. Detailed history, attention to evolving data, and iterative diagnostic reassessment were essential in the management of this complex rare condition.
-

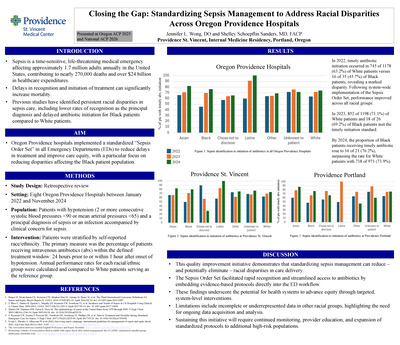
Closing the Gap: Standardizing Sepsis Management to Address Racial Disparities Across Oregon Providence Hospitals
Jennifer Wong, DO and Shelley Schoepflin Sanders, MD, FACP
Introduction: Sepsis is a time-sensitive, life-threatening medical emergency affecting approximately 1.7 million adults annually in the United States, contributing to nearly 270,000 deaths and over $24 billion in healthcare expenditures. Delays in recognition and initiation of treatment can significantly increase mortality. Previous studies have identified persistent racial disparities in sepsis care, including lower rates of recognition as the principal diagnosis and delayed antibiotic initiation for Black patients compared with White patients. In alignment with Providence’s mission to provide compassionate, equitable care, Oregon Providence hospitals implemented a standardized “Sepsis Order Set” in all Emergency Departments (ED) to reduce treatment delays and improve care equity, with a particular focus on reducing disparities affecting the Black patient population. Methods: A retrospective review was conducted using ED encounter data from eight Oregon Providence hospitals between January 2022 and November 2024. Eligible encounters included patients with a principal diagnosis of sepsis or an infection accompanied by clinical concern for sepsis. Patients were stratified by self reported race/ethnicity. The primary measure was the percentage of patients receiving intravenous (IV) antibiotics within the defined timely treatment window: 24 hours prior to or within 1 hour after onset of hypotension. Annual performance rates for each racial/ethnic group were calculated and compared, with White patients serving as the reference group. Results: In 2022, timely antibiotic initiation occurred in 63.2% of White patients versus 45.7% of Black patients, revealing a marked disparity. Following system wide implementation of the Sepsis Order Set, performance improved across all racial groups. In 2023, 71.1% of White patients and 69.2% of Black patients met the timely initiation standard. By 2024, the proportion of Black patients receiving timely antibiotics rose to 76.2%, surpassing the rate for White patients, 73.9%. Discussion: This quality improvement initiative demonstrates that standardizing sepsis management can reduce—and potentially eliminate—racial disparities in care delivery. The Sepsis Order Set facilitated rapid recognition and streamlined delivery of antibiotics by embedding evidence-based protocols directly into the ED workflow. These findings underscore the potential for health systems to advance equity through targeted, system-level interventions. Limitations include incomplete or underrepresented data for Latinx and “Other” racial groups, highlighting the need for ongoing data quality improvement and further analysis. Sustaining these gains will require continued monitoring, provider education, and expansion of standardized protocols to additional high-risk populations.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}