
-

Supplement Risk
Allison Connor, BS; Linh Tang Taylor, MD; and Jeffrey Youker, MD
Introduction: Increasingly, it is the case that patients are using a variety of supplements. About half of American adults use supplements. ¹. The purpose of this case report is to consider the impact of surreptitious supplement use on clinical presentation and under score the value in gathering a robust patient history. Case report: A 58-year-old man with prior history of infective endocarditis (IE) resulting in bioprosthetic aortic valve replacement (2 years prior) presented with worsening left lumbar pain and low-grade fever. He was found to have Methicillin resistant Staphylococcus aureus bacteremia with L4/5 vertebral osteomyelitis and a left psoas abscess. The bacteremia etiology was unclear, and patient denied active drug use; urine drug screen was positive for the medications the patient had been given at urgent care. Cardiology was consulted with concern for IE given his past medical history. Upon further probing however, the patient disclosed 2 months of bidaily subcutaneous injection of a peptide supplement obtained from the internet without medical guidance. There were no clear signs of intravenous substance use or IE stigmata on exam and subsequent workup with transesophageal echocardiography was negative. Bloodstream inoculation was presumed to be from self-injection of the supplement complicated by hematogenous seeding. The patient Was treated with 6 weeks of IV vancomycin home infusion. Discussion: Although this patient denied injection drug use, he was consistently injecting an unregulated internet-sourced peptide supplement that he was not asked about until the cardiology service saw him several days into his hospital course. Were this not discovered, the source of his bacteremia and resultant sequelae may have remained unclear. As such, the patient may have unknowingly returned to supplement injection without counseling of the inherent risk; hence, continuing the vicious cycle of introducing nidus for recurrent bacteremiaDietary supplement use is common and increasing among patients¹. However, less is known about the vetting of supplement sources and non-oral methods of administration. Dubious vendors of products and information are especially concerning in an era of unparalleled electronic accessibility concomitant with limited supplement oversight. Harms of self-administration may result from poor injection technique as well as product contaminants—e.g., bacterial and fungal pathogens². Pharmaceutical adulterants are another possible source of injury³. Although supplement use holds clinical significance, it is an oft-neglected portion of history in the inpatient setting in particular⁴. Conclusion --- There are 2 takeaways from this case. 1) Collecting a thorough history is an invaluable means of uncovering diagnostically significant information missed in prior interviews. 2) Physicians play a critical role in combatting medical misinformation and counseling patients on safe and appropriate supplement use. This is of considerable importance as public usage continues to uptrend in a poorly regulated supplement industry catalyzed by the surge of e-commerce.
-

Diagnostic Overlap in HUS: an Atypical Case
Ryan Daily, Med, DO and Andrea Roast, MD
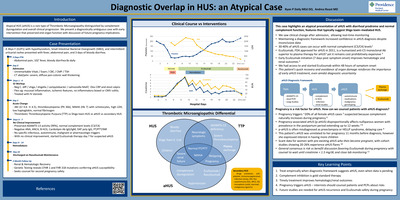
Introduction: Atypical HUS (aHUS) is a rare type of Thrombotic Microangiopathy distinguished by complement dysregulation and overall clinical progression. We present a diagnostically ambiguous case with early intervention that preserved end-organ function with discussion of future pregnancy implications. Case Presentation: A 36yo F (G2P1) with hypothyroidism, Small Intestinal Bacterial Overgrowth (SIBO), and intermittent urticarial rashes presented with fever, abdominal pain, and 3 days of bloody diarrhea. Discussion: This case highlights an atypical presentation of aHUS with diarrheal prodrome and normal complement function, features that typically suggest Shiga toxin–mediated HUS. We saw clinical change after admission, allowing real-time monitoring. Maintaining a diagnostic framework increased confidence in aHUS diagnosis despite inconclusive data. 30-40% of aHUS cases can occur with normal complement (C3/C4) levels. Eculizumab, FDA approved for aHUS in 2011, is a humanized anti-C5 monoclonal Ab superior to plasma therapy for aHUS2 yet it remains cost prohibitively expensive. Early Eculizumab initiation (7 days post symptom onset) improves hematologic and renal outcomes. We had access to and started Eculizumab within 48 hours of symptom onset, This patient's quick recovery and avoidance of organ damage reinforces the importance of early aHUS treatment, even amidst diagnostic uncertainty
-
 Gan, DO")
Beyond the Negative Serologies: A Case of Fulminant Vasculitis, Multiorgan Dysfunction, and an Uncharacteristic Infection
Guo Hui (Greyson) Gan, DO
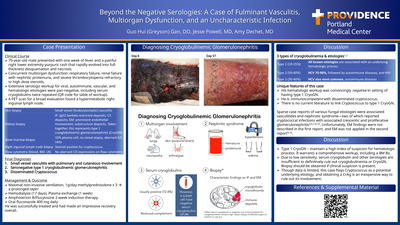
Case Presentation: 70-year-old male presented with one week of fever and a painful right lower extremity purpuric rash that rapidly evolved into fullthickness desquamation and necrosis. Concurrent multiorgan dysfunction: respiratory failure, renal failure with nephritic proteinuria, and severe thrombocytopenia refractory to high dose steroids. Extensive serologic workup for viral, autoimmune, vascular, and hematologic etiologies were pan-negative, including serum cryoglobulins twice repeated (QR code for table of workup). A PET scan for a broad evaluation found a hypermetabolic right inguinal lymph node. Discussion: Unique features of this case: His hematologic workup was convincingly negative in setting of having type 1 CryoGN. He is immunocompetent with disseminated cryptococcus. There is no current literature to link Cryptococcus to type 1 CryoGN. Sparse case reports of various fungal etiologies were associated vasculitides and nephrotic syndrome—two of which reported cryptococcal infections with associated crescentic and proliferative glomerulonephritis5,6,7,9,10. Unfortunately, EM findings were not described in first report and EM was not applied in the second report. Type 1 CryoGN – maintain a high index of suspicion for hematologic process. It warrants a comprehensive workup, including a BM Bx. Due to low sensitivity, serum cryoglobulin and other serologies are insufficient to definitively rule out cryoglobulinemia or CryoGN. Biopsy should be obtained if clinical suspicion is present. Though data is limited, this case flags Cryptococcus as a potential underlying etiology, and obtaining a CrAg is an inexpensive way to rule out its involvement.
-

A case of sweet Syndrome in a patient with Myelodysplastic Syndrome
Malia’ka Hall, DO and Elizabeth Hutshinson, MD
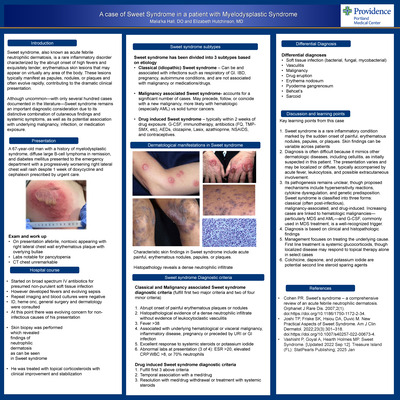
Introduction: Sweet syndrome, also known as acute febrile neutrophilic dermatosis, is a rare inflammatory disorder characterized by the abrupt onset of high fevers and exquisitely tender, erythematous skin lesions that may appear on virtually any area of the body. These lesions typically manifest as papules, nodules, or plaques and often evolve rapidly, contributing to the dramatic clinical presentation. Although uncommon—with only several hundred cases documented in the literature—Sweet syndrome remains an important diagnostic consideration due to its distinctive combination of cutaneous findings and systemic symptoms, as well as its potential association with underlying malignancy, infection, or medication exposure. Presentation: A 67‑year‑old man with a history of myelodysplastic syndrome, diffuse large B‑cell lymphoma in remission, and diabetes mellitus presented to the emergency department with a progressively worsening right lateral chest wall rash despite 1 week of doxycycline and cephalexin prescribed by urgent care. Discussion: Key learning points from this case; Sweet syndrome is a rare inflammatory condition marked by the sudden onset of painful, erythematous nodules, papules, or plaques. Skin findings can be variable across patients. Diagnosis is often difficult because it mimics other dermatologic diseases, including cellulitis, as initially suspected in this patient. The presentation varies and may be localized or diffuse, typically accompanied by acute fever, leukocytosis, and possible extracutaneous involvement.Its pathogenesis remains unclear, though proposed mechanisms include hypersensitivity reactions, cytokine dysregulation, and genetic predisposition. Sweet syndrome is classified into three forms: classical (often post‑infectious), malignancy‑associated, and drug‑induced. Increasing cases are linked to hematologic malignancies— particularly MDS and AML—and G‑CSF, commonly used in MDS treatment, is a well‑recognized trigger. Diagnosis is based on clinical and histopathologic findings Management focuses on treating the underlying cause. First line treatment is systemic glucocorticoids, though localized disease may respond to topical therapy alone in select cases Colchicine, dapsone, and potassium iodide are potential second line steroid sparing agents
-

Lemierre Syndrome: From Scalp to Cerebrum
Jack Hildenbrand, MD and Brinton Clark, MD
Background: Lemierre syndrome is a rare but severe infection, most commonly caused by Fusobacterium species originating from head and neck sources. Intracranial complications occur in only 11% of cases and are particularly uncommon in the absence of internal jugular vein thrombosis or endocarditis. Case Presentation: A 32-year-old previously healthy woman was admitted with sepsis due to Fusobacterium necrophorum bacteremia. Three weeks earlier, she had been hospitalized for sore throat and community-acquired pneumonia; blood and bronchoscopy cultures were negative, and she was discharged on amoxicillin-clavulanate. On readmission, blood cultures were positive for Fusobacterium necrophorum and evaluation revealed a right parietal scalp abscess, which was surgically drained. Transthoracic e chocardiography showed no valvular vegetations, and CT imaging revealed no thrombosis or thrombophlebitis of the head or neck. She was treated with ceftriaxone and metronidazole and discharged in stable condition on oral antimicrobials. Two days later, she re-presented with acute left-sided sensory changes and weakness. Neuroimaging demonstrated a right frontoparietal brain abscess and parietal meningitis with thrombosis of the right calvarial subarachnoid veins. She underwent craniectomy and surgical evacuation of the brain abscess, followed by four weeks of intravenous antibiotics. Despite aggressive management, she was left with partial left-sided hemiparesis and required inpatient rehabilitation for significant functional deficits. Discussion: Lemierre syndrome classically presents as oropharyngeal infection with subsequent septic thrombophlebitis. This case is notable for its atypical progression: likely unrecognized Fusobacterium pneumonia, followed by bacteremia, extracranial scalp abscess, and ultimately contiguous intracranial abscess with hemiparesis, despite timely source control and appropriate antibiotics. In the largest series of over 700 Lemierre syndrome cases, 17% developed early complications after diagnosis and treatment, with 3.8% developing septic intracranial lesions. In this patient, the brain abscess was contiguous with the scalp abscess, suggesting spread via emissary veins connecting scalp veins to the dural venous sinuses. Multiple imaging studies failed to demonstrate internal jugular vein thrombosis, but thrombosis of subarachnoid veins near the abscess was identified, supporting local contiguous spread. This case underscores the persistence and severity of Fusobacterium infections and highlights the risk of serious complications despite aggressive therapy. It emphasizes the need for vigilance, follow-up imaging, and consideration of prolonged therapy in Fusobacterium bacteremia. Conclusion: Clinicians should maintain a high index of suspicion for intracranial extension in patients with Fusobacterium bacteremia, even in the absence of classic findings such as endocarditis or internal jugular vein thrombosis. Early recognition, aggressive management, and appropriate antimicrobial duration are essential to mitigate neurologic morbidity.
-

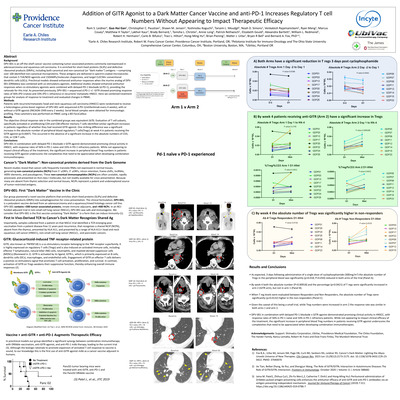
Addition of GITR Agonist to a Dark Matter Cancer Vaccine and anti-PD-1 Increases Regulatory T cell Numbers Without Appearing to Impact Therapeutic Efficacy
Rom S. Leidner1, Guo Hui Gan1, Christopher C. Paustian, and Shawn M. Jensen
Background: DPV-001 is an off-the-shelf cancer vaccine containing tumor associated proteins commonly overexpressed in adenocarcinoma and squamous cell carcinoma. It is enriched for short-lived proteins (SLiPs) and defective ribosomal products (DRiPs), including both canonical and non-canonical (or “dark matter”) antigens —comprising over 100 identified non-canonical microproteins. These antigens are delivered in spectrin-coated microvesicles that contain 5 TLR/ NOD agonists and 15DAMPs/molecular chaperones, and target CLEC9A+ conventional dendritic cells (cDCs). Preclinical models showed enhanced antitumor responses when the murine analog of DPV-001 (DRibbles) was combined with co -stimulatory agonists. Additional studies showed enhanced antitumor responses when co-stimulatory agonists were combined with delayed PD-1 blockade (d.PD1), providing the rationale for this trial. As presented previously, DPV-001 + sequenced d.PD-1 +/- GITR showed promising response rates of 56% (PD-1naïve) and 33% (PD-1 refractory) in recurrent/ metastatic HNSCC. Here we combined treatment groups for analysis of response to treatment and evaluated changes in PBMC. Methods: Patients with recurrent/metastatic head and neck squamous cell carcinoma (HNSCC) were randomized to receive a heterologous prime-boost regimen of DPV-001 with sequenced d.PD-1(retifanlimab every 4 weeks), with or without a GITR agonist (INCAGN-1949 every 2 weeks). Serial blood samples were obtained for immunologic profiling. Flow cytometry was performed on PBMC using a BD FacsCalibur. Results: The objective clinical response rate in the combined groups was equivalent (4/9). Evaluation of T cell subsets, specifically activated or proliferating CD4 and CD8 effector memory T cells identified similar significant increases in patients regardless of whether they had received GITR agonist. One striking difference was a significant increase in the absolute number of peripheral blood regulatory T cells(Tregs) at week 4 in patients receiving the GITR agonist (p=0.0007). This occurred in the absence of a significant increase in the absolute numbers of CD3, CD4, or CD8 T cells. Conclusions: DPV-001 in combination with delayed PD-1 blockade ± GITR agonist demonstrated promising clinical activity in HNSCC, with response rates of 56% in PD-1 naïve and 33% in PD-1 refractory patients. While not appearing to impact clinical efficacy of the treatment, the significant increase in peripheral blood Treg numbers in patients receiving GITR agonist underscores the complexities that need to be appreciated when developing combination immunotherapies.
-

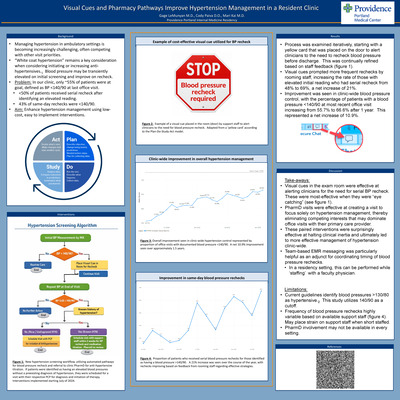
Visual Cues and Pharmacy Pathways Improve Hypertension Management in a Resident Clinic
Gage LeMunyan M.D.; Cody Paiva, DO; and Mari Kai, MD
Background: Managing hypertension in ambulatory settings is becoming increasingly challenging, often competing with other visit priorities. “White coat hypertension” remains a key consideration when considering initiating or increasing anti-hypertensives. Blood pressure may be transiently elevated on initial screening and improve on recheck. Problem: In our clinic, only ~55% of patients were at goal, defined as BP < 140/90 at last office visit. • < 50% of patients received serial recheck after identifying an elevated reading. • 43% of same-day rechecks were < 140/90. Aim: Enhance hypertension management using low-cost, easy to implement interventions. Results: Process was examined iteratively, starting with a yellow card that was placed on the door to alert clinicians to the need to recheck blood pressure before discharge. This was continually refined based on staff feedback. Visual cues prompted more frequent rechecks by rooming staff, increasing the rate of those with elevated initial reading who had serial recheck from 48% to 69%, a net increase of 21%. Improvement was seen in clinic-wide blood pressure control, with the percentage of patients with a blood pressure < 140/90 at most recent office visit increasing from 55.7% to 66.6% after 1 year. This represented a net increase of 10.9%. Discussion: Visual cues in the exam room were effective at alerting clinicians for the need for serial BP recheck. These were most-effective when they were “eye catching”. PharmD visits were effective at creating a visit to focus solely on hypertension management, thereby eliminating competing interests that may dominate office visits with their primary care provider. These paired interventions were surprisingly effective at halting clinical inertia and ultimately led to more effective management of hypertension clinic-wide. Team-based EMR messaging was particularly helpful as an adjunct for coordinating timing of blood pressure rechecks. In a residency setting, this can be performed while ‘staffing’ with a faculty physician. Limitations: Current guidelines identify blood pressures >130/80 as hypertensive. This study utilizes 140/90 as a cutoff. Frequency of blood pressure rechecks highly variable based on available support staff. May place strain on support staff when short staffed. PharmD involvement may not be available in every setting
-

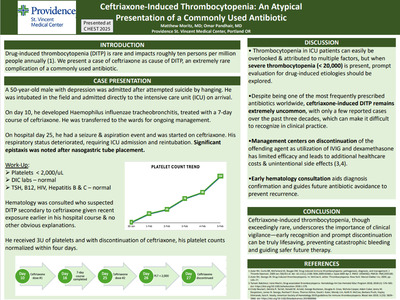
Ceftriaxone-Induced Thrombocytopenia: An Atypical Presentation of a Commonly Used Antibiotic
Matthew Moritz and Omar Pandhair
INTRODUCTION: Drug-induced thrombocytopenia (DITP) is rare and impacts roughly ten persons per million people annually (1). Over one-hundred medications have been identified as possible offenders, with immune response occurring within one to two weeks of drug exposure (2). Here we present a case of ceftriaxone as cause of DITP, an extremely rare complication of a commonly used antibiotic. CASE PRESENTATION: A fifty-year-old male with diabetes and depression initially presented after attempted suicide by hanging. He was intubated in the field and admitted directly to the intensive care unit (ICU). He remained in the ICU due to persistent encephalopathy which was confounded by polysubstance withdrawal and brain anoxia. His course was complicated by Haemophilus influenzae tracheobronchitis which was treated with a seven-day course of ceftriaxone. This was completed on day sixteen of his hospital course. He was eventually extubated and transferred to the hospitalist service. On hospital day twenty-five, he suffered a seizure and suspected aspiration event, and again ceftriaxone was administered to cover for potential aspiration pneumonia. He became more tachypneic, lethargic, and febrile so was transferred back to the ICU and reintubated. Epistaxis was noted after nasogastric tube placement. The following morning, his laboratory studies revealed a platelet count of< 2,000/uL. His heparin-induced thrombocytopenia (HIT) "4T" score suggested a low probability of HIT and additional studies ruled out disseminated intravascular coagulation; TSH, B12, HIV, Hepatitis C, and Hepatitis B were all negative as well. Hematology was consulted who felt this was most consistent with DITP due to ceftriaxone given recent exposure earlier in his hospital course. He received three units of platelets and with discontinuation of ceftriaxone, his platelet counts normalized within four days. DISCUSSION: Thrombocytopenia occurs frequently in patients admitted to the intensive care unit and is often attributed to sepsis, critical illness, and bone marrow suppression. However, a platelet count< 20,000/uL should raise suspicion for a more sinister process. Despite being one of the most used antibiotics, ceftriaxone is rarely the culprit of DITP, with only a handful of case reports identified in the literature over the past thirty years. Our case emphasizes the importance of discontinuation of the offending agent (i.e ceftriaxone) with as-needed platelet transfusions to avoid bleeding complications. Contrary to previous case reports, utilization of intravenous immunoglobulin and dexamethasone, which has only shown to be beneficial in case reports of DITP and primary ITP respectively, is unnecessary and can lead to additional healthcare costs and unintentional side effects (3,4). We also demonstrated benefits of early hematology consultation, which supported the management approach and helped confirm the DITP diagnosis, particularly emphasizing the avoidance of ceftriaxone in the future to prevent a potentially fatal recurrence. CONCLUSIONS: Thrombocytopenia is a commonly encountered diagnosis; however, ceftriaxone-induced thrombocytopenia is extremely rare. DITP should be on the differential diagnosis especially when platelet counts drop below 20,000/uL. When suspected, offending medications should be promptly discontinued to avoid serious, life-threatening bleeding complications.
-

Acquired Amegakaryocytic Thrombocytopenia and Pure Red Cell Aplasia as Initial Presentation Of Thymoma
Nidhi Patel, MD and Natasha Edwin, MD
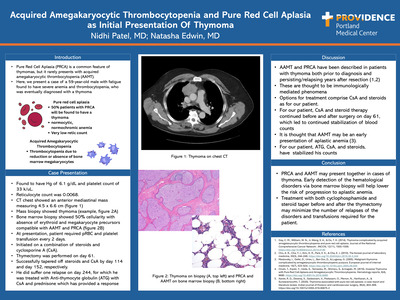
Introduction: Pure Red Cell Aplasia (PRCA) is a common feature of thymomas, but it rarely presents with acquired amegakaryocytic thrombocytopenia (AAMT). Here, we present a case of a 59-year-old male with fatigue found to have severe anemia and thrombocytopenia, who was eventually diagnosed with a thymoma Case Presentation: Found to have Hg of 6.1 g/dL and platelet count of 33 k/uL; Reticulocyte count was 0.0068. CT chest showed an anterior mediastinal mass measuring 4.5 x 6.6 cm. Mass biopsy showed thymoma. Bone marrow biopsy showed 50% cellularity with absence of erythroid and megakaryocyte precursors compatible with AAMT and PRCA. At presentation, patient required pRBC and platelet transfusion every 2 days. Initiated on a combination of steroids and cyclosporine A (CsA). Thymectomy was performed on day 61. Successfully tapered off steroids and CsA by day 114 and day 152, respectively. He did suffer one relapse on day 244, for which he was treated with Anti-thymocyte globulin (ATG) with CsA and prednisone which has provided a response Discussion: AAMT and PRCA have been described in patients with thymoma both prior to diagnosis and persisting/relapsing years after resection. These are thought to be immunologically mediated phenomena. Options for treatment comprise CsA and steroids as for our patient. For our patient,CsAand steroid therapy continued before and after surgery on day 61, which led to continued stabilization of blood counts. It is thought that AAMT may be an early presentation of aplastic anemia. For our patient, ATG, CsA, and steroid, have stabilized his counts Conclusion: PRCA and AAMT may present together in cases of thymoma. Early detection of the hematological disorders via bone marrow biopsy will help lower the risk of progression to aplastic anemia. Treatment with both cyclophosphamide and steroid taper before and after the thymectomy may minimize the number of relapses of the disorders and transfusions required for the patient
-

Postpartum Spontaneous Coronary Artery Dissection with Multivessel Arteriopathy
Devon Schaefer, DO and Cody Paiva, DO
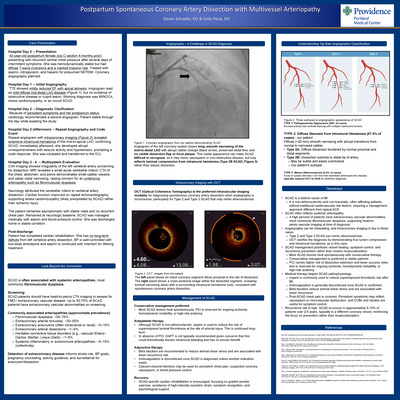
Case Presentation: Hospital Day 0 – Presentation: 43-year-old postpartum female (s/p C-section 4-months prior) presenting with recurrent central chest pressure after several days of intermittent symptoms. She was hemodynamically stable but had diffuse T‑wave inversions and a marked troponin rise. Treated with aspirin, nitroglycerin, and heparin for presumed NSTEMI. Coronary angiography planned. Hospital Day 1 -- Initial Angiography: TTE showed mildly reduced EF with apical akinesis. Angiogram read as mild diffuse mid-distal LAD disease (Figure 1), but no evidence of obstructive disease or culprit lesion. Working diagnosis was MINOCA, stress cardiomyopathy, or an occult SCAD. Hospital Day 2 -- Diagnostic Clarification: Because of persistent symptoms and her postpartum status, cardiology recommended a second angiogram. Patient stable through the day while awaiting the study. Hospital Day 2 (Afternoon) -- Repeat Angiography and Code Event: Repeat angiogram with intracoronary imaging (Figure 2) revealed extensive intramural hematoma of the mid‑to‑apical LAD, confirming SCAD. Immediately afterward, she developed abrupt unresponsiveness with seizure activity and hypotension, prompting a code response. She was intubated and transferred to the ICU. Hospital Day 2 - 4 -- Multisystem Evaluation CVA imaging showed irregularity of the left vertebral artery concerning for dissection. MRI revealed a small acute cerebellar infarct. CTA of the chest, abdomen, and pelvis demonstrated small‑caliber vessels and celiac ostial narrowing, raising concern for an underlying arteriopathy such as fibromuscular dysplasia. Neurology attributed the cerebellar infarct to vertebral artery dissection. Cardiac function improved on repeat echocardiography, supporting stress cardiomyopathy (likely precipitated by SCAD) rather than ischemic injury. The patient remained asymptomatic with stable vitals and no recurrent chest pain. Remained at neurologic baseline. SCAD was managed medically with aspirin and blood‑pressure control. She was discharged home in stable condition. Post-discharge: Patient has completed cardiac rehabilitation. She has no long-term deficits from left vertebral artery dissection. BP is well-controlled with low-dose amlodipine and aspirin is continued with intention for lifelong treatment. Takeaways: SCAD is a distinct cause of MI It is non-atherosclerotic and non-traumatic, often affecting patients without traditional cardiovascular risk factors, requiring a management approach different from typical ACS. SCAD often reflects systemic arteriopathy A high percent of patients have extra coronary vascular abnormalities, most commonly fibromuscular dysplasia, supporting head-to-pelvis vascular imaging at time of diagnosis Angiography can be misleading, and intracoronary imaging is key in these cases Type 2 and Type 3 SCAD can mimic atherosclerosis. OCT clarifies the diagnosis by demonstrating true lumen compression and intramural hematoma, as in this case. SCAD management prioritizes vessel healing, symptom control, and recurrence prevention rather than routine revascularization Most SCAD lesions heal spontaneously with conservative therapy. Conservative management is preferred in stable patients PCI carries higher risk of dissection extension and lower success rates, and is reserved for ongoing ischemia, hemodynamic instability, or high‑risk anatomy. Medical therapy targets SCAD pathophysiology Aspirin is commonly used to reduce superimposed thrombotic risk after MI. Anticoagulation is generally discontinued once SCAD is confirmed. Beta blockers reduce arterial shear stress and are associated with lower recurrence Post‑SCAD chest pain is common. Persistent symptoms may reflect vasospasm or microvascular dysfunction, and CCBs and nitrates are useful for symptom control. Recurrence risk is high. SCAD re-occurs in approximately 5-15% of patients over 2-5 years, typically in a different coronary vessel, reinforcing the focus on prevention rather than revascularization.
-

Individuals deemed low risk for cardiotoxicity with HER2-directed antibody therapy developed modest incidences of treatment-related LVEF decline and heart failure across a large Western US hospital system
Cameron Smith1, David Page1, Michael Layoun, and Li Hsin-Fang
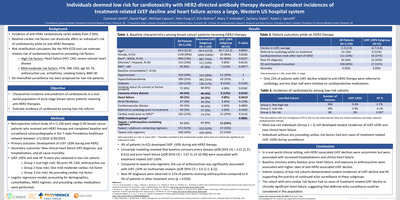
Background: Incidence of anti-HER2 cardiotoxicity varies widely from 3-30%. Baseline cardiac risk factors can drastically affect an individual's risk of cardiotoxicity while on anti-HER2 therapies. Risk stratification calculators like the HFA-ICOS tool can estimate relative risk of cardiotoxicity based on preceding risk factors. High risk factors: Heart failure (HF), CAD, severe valvular heart disease. Mild-moderate risk factors: HTN, DM, CKD, age 65-79, anthracycline use, arrhythmia, smoking history, BMI>30. De-intensified surveillance has been proposed for low-risk patients. Objective: Characterize incidence and predictors of cardiotoxicity in a real world population of early-stage breast cancer patients receiving anti-HER2 therapies. Evaluate incidence of cardiotoxicity among low-risk cohorts. Methods: Retrospective cohort study of n=1,156 early stage (I-III) breast cancer patients who received anti-HER2 therapy and completed baseline and surveillance echocardiography in the 7-state Providence healthcare network between 1/1/2016-3/20/2024. Primary outcome: Development of LVEF < 50% during anti-HER2. Secondary outcomes: New clinical heart failure (HF) diagnosis, any hospitalization, and all-cause mortality. LVEF ≤50% and new HF % were also obtained in low-risk cohorts: Group 1 (not high risk): No prior HF, CAD, anthracycline use; Group 2 (low-risk): One mild-moderate cardiac risk factor; Group 3 (no-risk): No preceding cardiac risk factor. Logistic regression models accounting for demographics, comorbidities, HER2 regimen, and preceding cardiac medications were performed. Conclusions: In a real-world clinical setting, anti-HER2-associated LVEF declines were uncommon but were associated with increased hospitalizations and clinical heart failure. Baseline coronary artery disease, prior heart failure, and exposure to anthracyclines were associated with higher rates of anti-HER2- associated LVEF decline. Interim analysis of low-risk cohorts demonstrated modest incidences of LVEF decline and HF, supporting the practice of continued echo surveillance in these subgroups. The cohort with zero cardiac risk factors had no cases of treatment-related LVEF decline or clinically significant heart failure, suggesting that deferred echo surveillance could be considered in this population.
-

Revolutionizing hematology/oncology education with visual storytelling and “Gamification” for internal medicine residents
N Smith1, A Patel1, J Dechet, and C Powell
Introduction: Hematology/oncology ranks among the lowest scoring sections on in-training exams for internal medicine residents. Prior resident feedback expressed a need for an improved didactic curriculum that was applicable to internal medicine residents and board examinations Aim: To enhance curriculum through multimodal education by integrating traditional didactic presentations along with specific lectures utilizing visual storytelling, memory palaces, and gamification. Methods: Trainees completed a 5-point Likert scale survey on their perceptions of hematology and oncology with a 16-question quiz before and after the curriculum. Multimodal lecture series created using "murder mystery" and "jewel heist" to teach hemolytic anemia, team-based Jeopardy-style format to teach pertinent testable topics, and additional didactics lectures from specialists. Unpaired t-test used for data analysis Conclusions: A multimodal didactics curriculum using visual storytelling, memory palaces, and gamification may improve residents' knowledge on commonly tested topics in hematology and oncology. Resident confidence in encountering heme/onc scenarios and enjoyment in the specialty also increased with this format. Based on these findings, we aim to design a year-long, multimodal curriculum to elevate interest in heme/onc and improve internal medicine resident knowledge in this field.
-

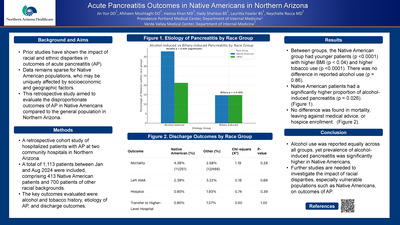
Acute Pancreatitis Outcomes in Native Americans in Northern Arizona
Jin Yun DO1; Afsheen Moshtaghi DO2; Hamza Khan, MD2; Hady Shahbaz BS2; Yoshinobu Koguchi; Tarsem L. Moudgil; Noah D. Simons; and Venkatesh Rajamanickam
Background and Aims: Prior studies have shown the impact of racial and ethnic disparities in outcomes of acute pancreatitis (AP). Data remains sparse for Native American populations, who may be uniquely affected by socioeconomic and geographic factors. This retrospective study aimed to evaluate the disproportionate outcomes of AP in Native Americans compared to the general population in Northern Arizona. Methods: A retrospective cohort study of hospitalized patients with AP at two community hospitals in Northern Arizona. A total of 1,113 patients between Jan and Aug 2024 were included, comprising 413 Native American patients and 700 patients of other racial backgrounds. The key outcomes evaluated were alcohol and tobacco history, etiology of AP, and discharge outcomes. Results: Between groups, the Native American group had younger patients (p < 0.0001) with higher BMI (p < 0.04) and higher tobacco use (p < 0.0001). There was no difference in reported alcohol use (p = 0.86). Native American patients had a significantly higher proportion of alcohol-induced pancreatitis (p = 0.026). No difference was found in mortality, leaving against medical advice, or hospice enrollment. Conclusion: Alcohol use was reported equally across all groups, yet prevalence of alcohol-induced pancreatitis was significantly higher in Native Americans. Further studies are needed to investigate the impact of racial disparities, especially vulnerable populations such as Native Americans, on outcomes of AP.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.




{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}