
-

What Health Care Leaders Can Learn From Amazon
Amy Compton-Phillips and Goran Henricks
Leading change in the internet economy takes different thinking and skills then those that got us the healthcare miracles we have today. Tech companies learned they needed to perfect the product, get serious about costs, remove friction, control the last mile, and accelerate careers to disrupt their industry. Healthcare leaders, and the systems they run, can use the same concepts to re-think our entrenched care models of today. Design thinking coupled with a scrupulous focus on value can help create the nimble systems we all want to work (and receive care) in. Learn how to go from idea to action in this interactive, energizing session.
-

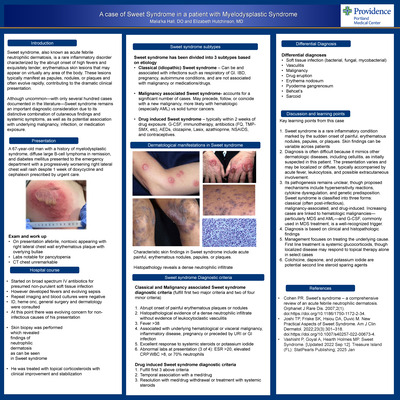
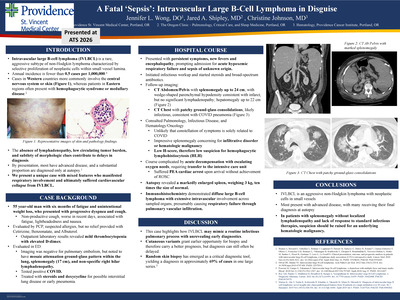
Teamwork, Communication, and Data: 3 Keys to Large- Scale Practice Change in Opioid Prescribing
Linda Cruz and Ryan Dix
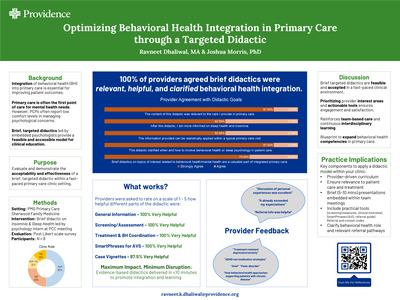
This session will share lessons learned from the four-year implementation of a pain-care pathway across 45 patient-centered medical home (PCMH) clinics in Oregon. Leveraging the PCMH team, communication, and data to improve pain management and reduce risk, Providence Medical Group was able to realize a 68% reduction of patients on high-dose opioids. After this presentation you will be able to:
- Explain a scalable approach, using CDC guidelines, to implement a pathway to reduce opioid prescribing in primary care
- Discuss three key principles of implementing a pain-care pathway in a team-based care environment
- Develop an opioid care pathway action plan at an organization.
-

Hospital Libraries: A Path Forward
Basia Delawska-Elliott and Wm. Brian Elliot
Program Description: Despite our profession’s constant evolution to address the changing needs of our users, many health sciences libraries, particularly hospital libraries, are under scrutiny by their institutions. Many of these libraries are facing closure. In fact, a recent study of health sciences library closings [Schwartz, Elkin 2017] found that from 1989-2006 approximately 23-34% of US health sciences libraries closed. Furthermore, between 2011 and 2015, 613 libraries closed, for an average of 115 closings per year [Thibodeau, Funk 2009]. But why? What was the rationale for these closings? Was the decision based solely on economic reasons, or were there other underlying motives? How will providers who lack library services fill their information needs? How can we prevent the closing of additional libraries? This Special Content Session will focus on the ongoing challenges faced by health sciences libraries to remain relevant in an ever-changing world. A panel of speakers will share their experiences with library closures and strategies and best practices for remaining vigilant and promoting library staff, resources, and services effectively. The panel will be followed by an open forum discussion of health sciences library closings in general.
-

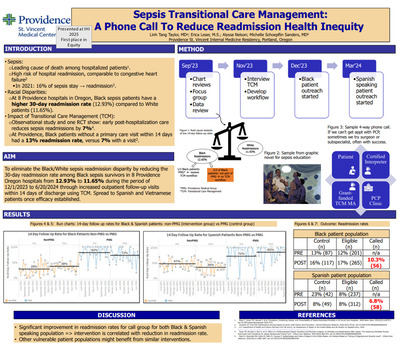
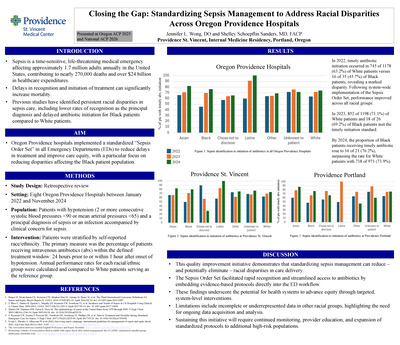
250 Miles Apart, Saving Lives Together: Stop Sepsis
Ann C. Eells, Christiana Paul, Caroline Williams, Robert Fitting, Mauren Disbot, Bradley Shroeder, Jenifer Rofkahr, and Amy Samolis
-

High Reliability + Value Improvement = Learning Organization
Sheri Feeney, Liga Mezaraups, Douglas Meyer, Glenda Battey, and Linda Severs
Experience how the 3rd largest nonprofit health-system is becoming a learning organization. Engaging frontline staff in high reliability and improvement skills is critical to a High Reliability Learning Organization (HRLO). Leaders and staff pursuing daily improvement deliver greater value to patients, each other, business operations, and their communities. Participants will learn how to combine HRO and improvement science so everyone has the skills, will, and freedom to provide more affordable care and attain zero harm.
Objectives:
- Identify successful elements and challenges of implementation and spread of our high reliability behaviors.
- Demonstrate how HRO behaviors are the foundation for daily improvement across a large organization.
- Apply Clinical Value Improvement to empower employees to improve their job, quality, and affordability.
- Learn how HRO and CVI are integral to PSJH’s strategic plan and leadership development.
-

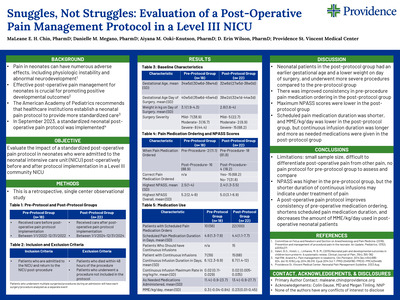
Caring for Newborns With Transitional Hypoglycemia: Best Practices for Education Healthcare Providers and Families
Emelia C. Garcia, JoAnn D. Long, and Monica T. Foster
A number of fetal-maternal conditions predispose infants to hypoglycemia. Consensus on postnatal glucose screening and management is mixed contributing to ineffective communication during level of care transition. This project presents evidence informing best practices in how to educate healthcare providers and families of newborns with hypoglycemia.
-

Moving Slow to Move Fast-Nursing Handovers-Implementing Electronic to ED Report to Improve Throughput
Dawn Gilbert, Roni Lyons, Patrick Mugrage, and Linda Severs
-

Integrate Behavioral Health in the ED and Upstream
Katie Gilligan and Heidi Beazizo
This interactive session will describe the changes being tested by 10 hospitals in the Integrating Behavioral Health in the ED and Upstream Learning Community, convened by IHI and Well Being Trust, to achieve meaningful improvements for patients with mental health and substance abuse conditions, their families, and ED staff. Participants will learn from experts and participating team members, share learning with other participants, and develop action plans for bringing this critical work to their organizations.
After this presentation you will be able to:
- Describe a theory of change and set of core measures to improve patient outcomes, experience, and staff safety while reducing avoidable ED re-visits
- Explain key changes tested by a range of health care organizations and results that can be achieved
- Identify strategies and ideas to test at any organization
-
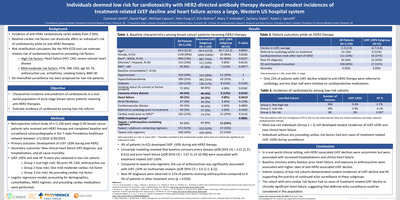
 order to reduce inappropriate utilization by Ty J. Gluckman, Maulin P. Shah, Nicole E. Ondoworth, Stephanie C. Fine, Jonathan V. Laius, Wendy W. Yu, Janelle D. Stevens, Shelley L. Schoepflin Sanders, Ruben O. Halperin, Braden W. Batkoff, Robert M. Dressler, and Mark L. Sanz")
Implementation of an EMR-based continuous electrocardiographic monitoring (CEM) order to reduce inappropriate utilization
Ty J. Gluckman, Maulin P. Shah, Nicole E. Ondoworth, Stephanie C. Fine, Jonathan V. Laius, Wendy W. Yu, Janelle D. Stevens, Shelley L. Schoepflin Sanders, Ruben O. Halperin, Braden W. Batkoff, Robert M. Dressler, and Mark L. Sanz
-

Implementation of an EMR-based cardiovascular discharge checklist to close gaps in care
Tyler J Gluckman, Maulin P. Shah, Elizabeth A. Widhalm, Daniel J. Weidert, Stephanie C. Fine, Jonathan V. Laius, Braden Batkoff, and Mark L. Sanz
-

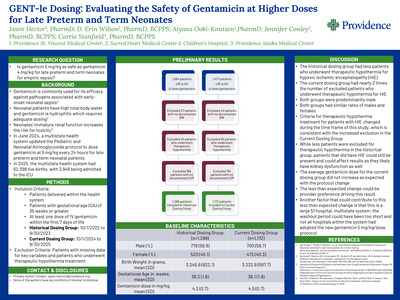
Where's the Money? Revenues associated with 3000 Lung Cancer Screens
John Handy Jr., Courtney Wood, Erika Rauch, Kevin Olson, Roshanthi Weerasinghe, Rachel Sanborn, and Micheal Skokan
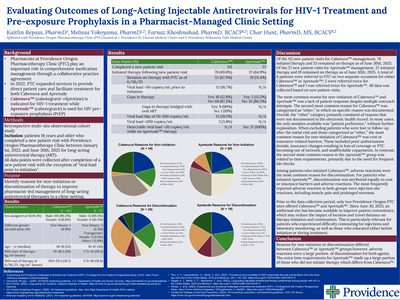
Objective: Since the National Lung Screening Trial (NLST), lung cancer screening (LCS) has been widely implemented but little is known about LCS finances. We describe revenues associated with screening and immediate downstream clinical activity.
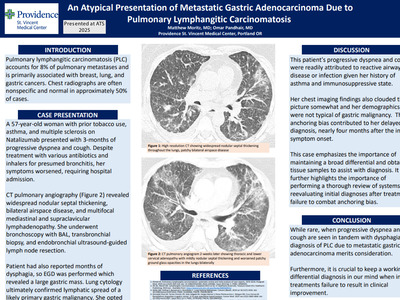
Methods: A lung cancer screening (LCS) program began in November 2013 incorporating 7 hospitals (2 non-university tertiary and 5 community medical centers) and 3 free standing imaging centers. Candidates were referred by primary care providers (PCP). LCS was carried out using the Center for Medicare & Medicaid Services modified NLST eligibility criteria. Dedicated radiologists at the tertiary centers interpreted all LCS, assigning Lung RADS categories. Every Lung RADS 4 LCS was reviewed by the multidisciplinary thoracic disease conference, generating management recommendations. The program coordinator recorded all imaging, procedures, adverse events, pathology, staging and ensured follow up LCS. Clinical and administrative data bases were combined, examining 2013 - May 2017. Weighted average payment (to account for payer differences) and average total costs (direct + indirect) were analyzed. Downstream clinical activity was identified from the index event (LCS) and examining subsequent clinical encounters using relevant ICD10 codes (neoplasm, tobacco use, oncology, etc).
Results: 1950 people underwent initial CT screening, 1160 underwent follow up LCS, totaling 3110 scans. Payers comprised Medicare-65%, commercial-20% and Medicaid-14%. 55 cancers were diagnosed, including 40 non-small cell (stage I-26; stage II-5; stage III- 4 and stage IV-5), 6 small cell and 9 extra-thoracic cancers. Lung cancer detection rate was 2.3%. Intervention included additional imaging (CT, XR, PET, US, MRI, bone scan, mammogram) in 483 (15.5%) and 111 procedures (5.6%). Invasive diagnostic procedures included bronchoscopy (27), CT-guided biopsy (19) and ultrasound guided biopsy (18). 47 surgeries were performed (1.5%). Thoracic surgeries included thoracoscopic lobectomy (21), thoracoscopic wedge resection (6), thoracoscopic anatomic segmentectomy (4) and thoracoscopic pneumonectomy (1). Adverse event rate for procedures was 10.8% (0.6% of all screened patients). One lobectomy patient died, yielding a 2.1% surgical mortality. LCS Revenues Events Average Total Cost Average Total Payment Net Margin LCS 2781 $357,493 $393,491 9.1% Additional imaging resulting from LCS 483 $129,492 $187,138 30.8% Downstream clinical activity 263 $654,340 $703,448 7%
Of the downstream clinical activity, thoracic surgery contributed 34%, medical oncology 21%, general surgery 19%, and pulmonology 14%.Conclusion: Beyond the substantial human and financial benefits of identifying curable early stage lung cancer, a low dose CT lung cancer screening program is profitable. 55% of payment results from downstream clinical activity while the LCS itself and additionally generated imaging generated 45%. This information can be used to allocate costs of a LCS program to clinical services and radiology.
-

#Work2BeWell Powered by Providence Health & Services
Robin Henderson and Mary Renouf-Hanson
Improving mental health and emotional well-being is the focus of many community health assessments and prevention efforts. This session will focus on innovative ideas that engage youth and their families where they are—in schools, communities and while seeking healthcare. Learn from healthcare leaders at Bellin Health, Cincinnati Children’s, Providence St Joseph Health and East London NHS Foundation Trust and their community partners as they share their successful efforts to change the conversation with today’s youth.
-

Changing Culture One PDSA at a Time: The Creation of an Innovation Unit
Jennifer Hoople, Gale Arnold, Jennifer Bletscher, Shawna Bolgen, Andy Branca, Tana Case, Matthew Dietz, Jennifer Ferenczy, Heather Haake, Janine Holbrook, Ingrid Jonely, Liga Mezaraups, Jessica Osantowski, Jessica Sehorn, Linda Severs, and Dina Shepelyuk
An inpatient unit in an acute care hospital was designated as an Innovation Unit. This unit was challenged with the creation of culture change in regards to process improvement. The team learned to use Improvement Science to facilitate rapid and innovative process improvements. These changes have enhanced the quality of healthcare provided while decreasing cost. The poster highlights some of the Improvement Science processes, forms, and roles of the team as well as some of the projects and successes.
-
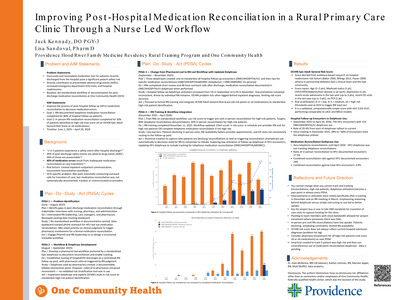
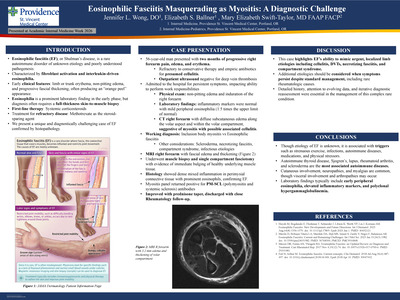
A Systematic Review and Meta-Analysis of Dual Antiplatelet Therapy Versus Antiplatelet Monotherapy After Coronary Artery Bypass Graft Surgery
Leonardo Knijnik, Rhanderson Cardoso, Manuel Rivera, Gilson Costa Fernandes Filho, Amanda Fernandes, John McEvoy, Seamus Whelton, Tyler J Gluckman, and Roger Blumenthal
Background
The role of dual antiplatelet therapy (DAPT) after coronary artery bypass grafting (CABG) is controversial, particularly among patients with stable ischemic heart disease (IHD).
Methods
We performed a systematic review and meta-analysis comparing DAPT to antiplatelet monotherapy following CABG. Subgroup analyses were performed in randomized trials (RCTs), stable IHD, extended duration DAPT (≥ 6 months), and long-term follow-up (≥ 2 years).
Results
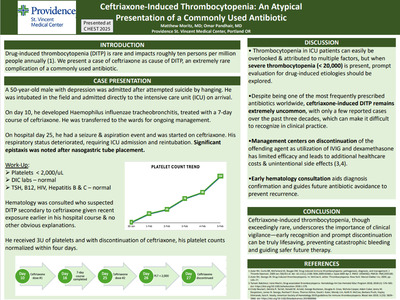
Twenty studies and 19,795 patients were included, of which 7301 (37%) received DAPT after CABG. Overall, DAPT was associated with a significant reduction in cardiovascular (CV) mortality (OR 0.66; p=0.01; Fig 1A) and a trend towards lower all-cause mortality (0.78; p=0.08). There were no between group differences in total mortality, CV mortality, myocardial infarction, or stroke in thesubanalyses of RCTs, stable IHD, extended DAPT, and long-term follow-up. Vein graft occlusion up to 1 year after CABG was significantly lower with DAPT in the overall analysis (OR 0.64; p=0.01; Fig 1B) and in RCTs (OR 0.58; P
Conclusion
Although DAPT is associated with a lower CV mortality in an unselected population after CABG, our findings suggest that routine DAPT after CABG does not improve clinical endpoints when evaluated in RCTs or in patients with stable IHD, but does reduce rates of early vein graft occlusion.
-

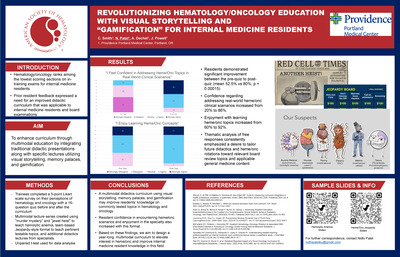
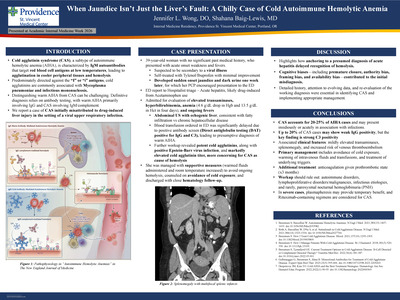
Bridging the Gap: An Innovative Web-Based Approach for Evaluating EBP Readiness in Direct Care Nurses
JoAnn D. Long, Stacey L. Spradling, Karen Baggerly, Nikki L. Galaviz, and Jamie Roney
The provision of universal and equitable access to safe and effective healthcare emphasized in The 2012 World Health Report, 'no health without research': The endpoint needs to go beyond publication outputs, has forwarded the global evidence-based practice (EBP) movement (Zachariah et al., 2011). Notably, Lindeman (1975) identified research utilization and quality improvement as nursing priorities over forty years ago. Yet, current literature suggests research findings may take seventeen years to reach practice integration (Morris et al., 2011). Notably another dilemma added to the challenge is approximately 80% of current nursing practice does not reflect evidence-based nursing decisions (Conner, Dwyer, and Oliveria, 2016). Peer reviewed literature report direct care nurses self-identify lack of resources, time, and critical appraisal skills to navigate current literature (Yoder et al., 2014). Proficient skills of direct care nurses to acquire and appraise existing studies can be the catalyst translating scientific knowledge to the bedside; however, an understanding of the baseline knowledge and readiness of front-line providers is limited. Organizations worldwide are challenged to overcome these self-reported barriers to implementing and adopting research findings into clinical nursing practice. The purpose of this research study was to determine the self-perceived online research and critical appraisal skills and the EBP readiness and knowledge of front-line nurses from three care facilities in the southwest United States.
Methods: A cross-sectional exploratory descriptive design was used in this study. The Stevens EBP Readiness Inventory and EBP Knowledge Assessment questionnaires were used to assess direct care nurses’ self-reported evidenced-based readiness and baseline EBP knowledge. Research skill was measured using four questions adapted from the Research Readiness Self-Assessment tool. Informed consent was obtained from (N=49) Registered Nurses volunteering to participate. The survey questionnaires were administered online to nurses volunteering to participate from 22 nursing units during a 3-week period in May 2017.
Results: Demographic, descriptive, and frequency distributions were examined.Front-line nurses expressed the highest level of self-confidence in four questions pertaining to the area of use and implementation of clinical practice guidelines. The study data were analyzed using SPSS version 25. The highest area of perceived evidence-based practice readiness was ability to “deliver care using evidence-based clinical practice guidelines” with a mean 4.5, SD, 1.55; “use of agency-adopted clinical practice guidelines”, mean, 4.29, SD, 1.60; “choose evidence-based approaches over routine as a base for own clinical decision making”, mean 4.2, SD, 1.60; and “participate in evidence-based quality improvement processes to evaluate outcomes of practice changes”, mean, 4.02, SD, 1.49. In comparison, the lowest areas of self-confidence for evidence-based practice centered on a range of topics reflected in three questions reflecting the ability to assess the “major facets to be assessed when using clinical practice guidelines”, mean, 2.77, SD, 1.18; “ability to identify statistics commonly used in evidence summaries”, mean, 2.96, SD, 1.18; and “ability to conduct expert search strategies using pre-constructed strategies in major databases”, mean, 2.67, SD, 1.21. The remaining 14 questions assessing evidence-based practice readiness ranged from a low mean score of 3.02 – 3.69, reflecting scores falling approximately half-way between having “very little” to having a “great deal” of evidence-based readiness.
Conclusion: While front-line nurses reported high levels of self-confidence for using EBP to implement and deliver care using clinical practice guidelines, they also expressed lower knowledge and self-efficacy with use of more advanced EBP skills. Strengthening nurse online search skills was identified as the most important learning deficit in this sample of Registered Nurses. Limitations of this study included a voluntary and relatively small sample size and cross-sectional design. Findings from this study helped identify objective data to guide focused organizational education efforts to improve direct care nurses’ use of EBP and research concepts necessary to integrate research into clinical practice.
-

Medication Safety Zone to Promote Uninterrupted Medication Administration
Sandy Martir and Trisha Saul
-
Improving Engagement in an Emergency Department: A Quality Improvement Project
Roxanne McGray, Mary Waldo, and Catherine Van Son
Purpose: This quality improvement, doctorate of nursing practice (DNP) project assesses the need for and evaluates the impact of an engagement intervention focused on improving nurse, physician, and emergency department technician (EDT) engagement within an emergency department.
Background: Engagement is defined as an energetic state of involvement with personally fulfilling activities that enhance one’s sense of professional efficacy and is characterized by vigor, dedication, and absorption. While a significant amount of research exists that correlates the relationship between low nurse engagement levels with high turnover rates, there is little known about the effectiveness of interventions aimed at improving nurse engagement. Therefore, a project evaluating the impact of an engagement intervention on increasing engagement levels for all staff was piloted in an emergency department.
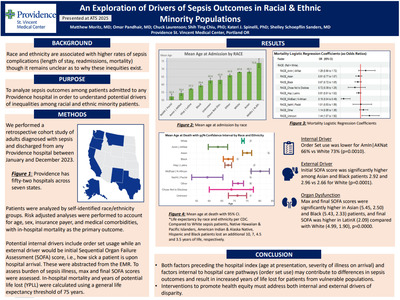
Methods: In September 2017 staff (physicians, nurses and EDTs) who work in the emergency department (N=69) completed a pre-intervention survey to assess baseline engagement levels, using the Utrecht Work Engagement Scale (UWES). The preintervention survey included open-ended questions developed by the project team to solicit qualitative information regarding engagement, as well as demographic questions. The preintervention data revealed overall low engagement levels of participants (m = 2.10, sd = 1.63, n=40). The dedication subscale had the lowest mean (m = 1.30, sd = 1.49), while the absorption subscale had the highest mean (m = 2.53, sd = 1.78); the vigor subscale fell between these two means (m = 2.33, sd = 1.59). The open-ended pre-intervention survey results, along with recommendations from the literature and guided by the six areas of worklife framework, were used to guide the design of the unit-based engagement intervention. Some of the interventions will include enhanced staff recognition, activities to improve the sense of community within the department, increased accountability of staff members, augmented shared governance structures, and improved follow-through by the leadership team when staff suggestions are presented. The post-intervention survey will be administered in March 2018 following the intervention phase of the project. Pre- and postintervention survey results and the intervention will be presented.
Outcomes: The level of staff engagement is the primary outcome of this quality improvement project. Pre- and post-intervention survey data will be compared to understand the effectiveness of the intervention designed to increase engagement in the emergency department. The outcomes of this project will help to inform future interventions focused on supporting and maintaining high levels of staff engagement.
Conclusion: Staff engagement is integral to the vitality of the healthcare workforce. A onesize- fits-all approach is not enough to keep staff engaged, excited to come to work, and able to provide the best care for their patients. Listening to staff suggestions and creating an individualized approach for each unit is essential to keep the workforce engaged.
-

Current and Emerging Treatments for Psoriatic Arthritis
Philip Mease
From the publisher:
Written by leading experts in the field and designed for dermatologists and residents, this book includes evidence-based medicine that underscores the clinical data, as well as practical tips on how to use both biologic and systemic agents in the field of dermatology. In the past decade, there have been several groundbreaking advances in medical dermatology. Novel biologic and systemic agents have been developed to treat inflammatory disorders, including psoriasis and atopic dermatitis, as well as skin malignancies such as melanoma.
Biologic and Systemic Agents in Dermatology encompasses these developments by describing the mechanism of action of these various agents and the clinical efficacy and safety to treating these respective disorders. The utilization of biologic and systemic agents in other dermatologic conditions, pharmacoeconomics, pharmacovigilance, and clinical trials outcomes are discussed as well as topics including tumor necrosis, conventional systemic agents for psoriatic disease, and oral agents for atopic dermatitis.
-

Axial Spondyloarthritis
Philip Mease and Muhammad Asim Khan
From the publisher:
Focusing on the key essentials you need to know, Axial Spondyloarthritis provides a quick, expert overview of axSpA from a clinical perspective. This concise resource by Drs. Philip Mease and Muhammad Khan presents practical recommendations and guidelines for the diagnosis, management, and treatment of spondyloarthritis impacting the axial skeleton alongside an overview of epidemiology, special populations, and patient education.
Key Features:
- Discusses key information on genetic factors and disease biomarkers.
- Presents an overview of clinical features, classification criteria, and imaging to aid in diagnosis.
- Covers management and treatment guidelines, including non-pharmacologic management and the use of biologics.
- Consolidates essential information on this timely topic into a single, convenient resource.
-
Impact and Predictors of Paravalvular Regurgitation Following Implantation of the Fully Repostionable and Retrievable Lotus Transcatheter Aortic Valve: Results From the Reprise III Randomized Controlled Trial
Daniel O'Hair, Vivek Rajagopal, Axel Linke, Dean Kereiakes, Ron Waksman, Vinod H. Thourani, Nicolas Dumonteil, Robert W. Hodson, Jeffrey Southard, John Harrison, Samir Kapadia, Dominic Allocco, Ian Meredith, Michael Reardon, and Ted Feldman
Background
Paravalvular leak (PVL) following TAVR has been associated with worse long-term outcomes including an increased risk of mortality. REPRISE III was a large randomized trial comparing 2 contemporary TAVR devices: Lotus and CoreValve (CV). Lotus incorporates an adaptive seal designed to minimize PVL. In this analysis, we evaluated the predictors of PVL and its impact on clinical outcomes.
Methods
Patients with high/extreme surgical risk and severe, symptomatic aortic stenosis underwent randomization to Lotus or CV. Multivariate modeling to assess predictors of PVL and outcomes stratified by PVL at 30 days were evaluated.
Results
We randomized 912 patients (2 Lotus:1 CV), age 83±7 years, 51% female, and Society of Thoracic Surgeons predicted risk of mortality 6.8%±4.0%. Lotus was superior to CV for the secondary endpoint of ≥moderate PVL at 1 year (Lotus 0.9%, CV 6.9%; p
Conclusion
Rates of PVL with the Lotus valve were lower than with CV. Calcium was a strong predictor of PVL. Overall, outcomes were similar between groups at 1 year though longer-term follow-up is needed.
-

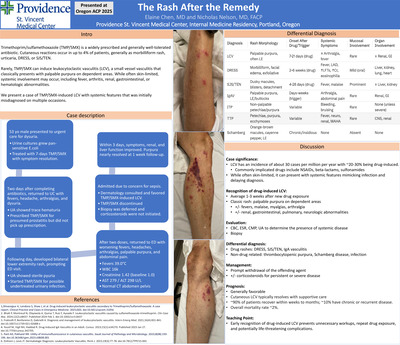
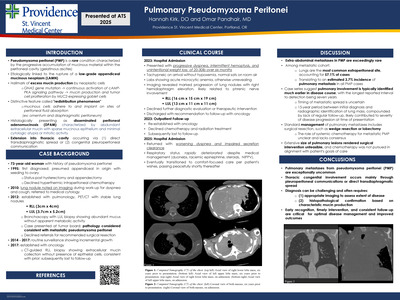
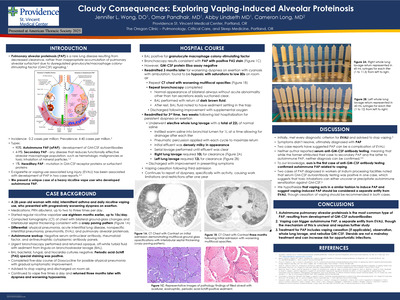
Updated efficacy of first or second-line pembrolizumab plus in metastatic triple negative breast cancer and correlations with baseline lymphocyte and naïve CD4+ T-cell count
David Page, Joanna Pucilowska, Laura Bennetts, I Kim, Katherine Sanchez, Maritza Martel, Alison Conlin, Nikki Moxon, Staci Mellinger, Anupama Acheson, K Kemmer, Z Mitri, J Vuky, J Ahn, C Abaya, T Manigault, R Basho, Walter Urba, and HL McArthur
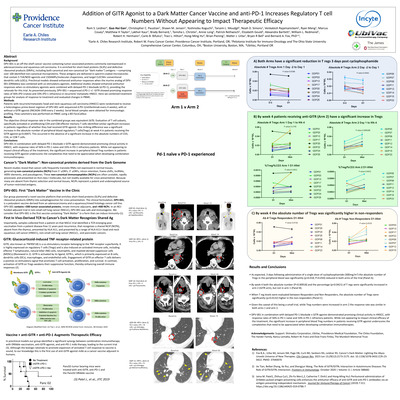
Background: In mTNBC, anti-PD-1/L1 monotherapy is most effective when administered early in the course of disease, with recent trials demonstrating overall response rates (ORR) of 23-26% in the first-line setting and 5-6% in later lines. This may reflect iatrogenic lymphopenia from preceding cytotoxic chemotherapy. Furthermore, curative-intent chemotherapy is associated with prolonged suppression of naïve CD4+ cells, a T-cell subset that may play a critical role in the generation of de novo anti-tumor immune responses. We present the final clinical results of a pilot study evaluating the safety and efficacy of combining pembrolizumab plus standard-of-care capecitabine in the first/second-line mTNBC setting. We also explore potential associations between clinical benefit and lymphopenia, preceding chemotherapy, and absolute naïve CD4+ counts.
Methods: In a pilot study, we evaluated the tolerability and preliminary efficacy of concurrent pembro (200mg IV q21 day) plus investigator-selected 1st/2nd line paclitaxel (80mg/m2 IV weekly) or oral cape (2,000mg BID, weekly 1 on/1 off). The primary endpoint was tolerability, defined as the proportion of subjects receiving >6 weeks concurrent therapy without dose discontinuation with toxicities reported per CTCAE v4.0. The secondary endpoint was 12-week objective response rate (ORR) by RECIST1.1. Exploratory endpoints included peripheral blood cell enumeration by real-time flow cytometry and routine clinical laboratory. Naïve CD4+ cells were defined as CD45+ CD3+ TCRab+ CD4+ CD45RA+ CCR7+. Here, we report the results of the pilot phase of the cape cohort (NCT02734290).
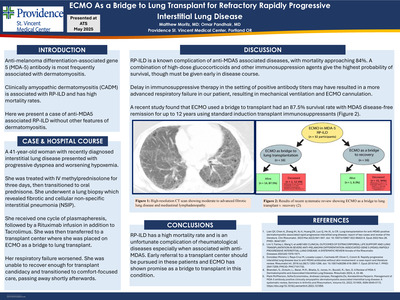
Results: Twelve of 14 subjects were treated in the first-line setting. All subjects (14/14, 100%) tolerated cape+pembro for >6 weeks, with toxicities consistent with monotherapy cape experience (diarrhea: grade I-II 50%, grade III 7%; hand-foot: grade I-II 71%) that improved with dose-reduction as needed. At 12 weeks, the ORR was 6/14 (42.9%), and the clinical benefit rate (ORR + stable disease) was 8/14 (57.1%). Depressed absolute lymphocyte count at baseline (ALC<1.0/uL: 33% CBR; ALC≥1.0/uL: 75% CBR) and recent exposure to cytotoxic chemotherapy (6 months: 75% CBR) were associated with reduced clinical benefit. By flow cytometry, subjects experiencing clinical benefit had higher baseline absolute naïve CD4+ counts (average 283 cells/uL v. 93 cells/uL, p=.069).
Conclusions: This study met the primary endpoint of safety for cape plus pembro in mTNBC, with encouraging clinical activity. These data are supportive of further studies evaluating combination chemotherapy plus anti-PD-1/L1 mTNBC. We observed greater clinical benefit in subjects with non-suppressed ALC, less exposure to recent chemo, and higher baseline naïve CD4+ counts, suggesting that iatrogenic immunosuppression can impair response to immune checkpoint therapy in mTNBC. These findings should be confirmed in ongoing randomized trials of immune checkpoint +/- chemotherapy in mTNBC, and should be considered in the design of future clinical trials.
-
Oral anticoagulant use in patients with atrial fibrillation managed by primary care and cardiology providers with or without use of a structured note for PINNACLE Registry reporting
J Petersen, Tyler J Gluckman, S Ingale, L Zhao, J Westcott, D Wells, J Buckler, and C Dale
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.







{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}