-

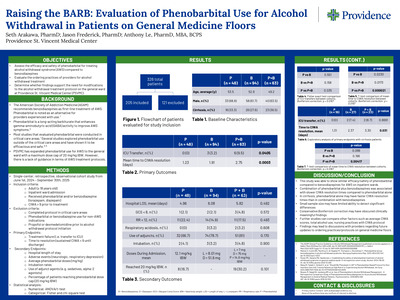
Raising the BARB: Evaluation of Phenobarbital Use for Alcohol Withdrawal in Patients on General Medicine Floors
Seth Arakawa, Jason Frederick, and Anthony Le
Abstract: Alcohol withdrawal syndrome (AWS) can present as a spectrum of symptoms such as a mild headache, gastrointestinal issues, and diaphoresis. However, if not treated properly, it can progress to severe hallucinations, seizures, or delirium tremens. Current guidelines from the American Society of Addiction Medicine (ASAM) recommend benzodiazepines as first line agents for alcohol withdrawal with phenobarbital recommended as an adjunct agent or replacement to benzodiazepines by providers who are familiar with its use. Although most evidence supporting phenobarbital in AWS comes from critical care settings, emerging data suggest it may also be safe and effective in general ward patients. Providence St. Vincent Medical Center (PSVMC) recently expanded phenobarbital use for AWS to the general ward floors with a dose cap of 20 mg/ kg ideal body weight (IBW), but guidance is lacking for alcohol withdrawal management. The purpose of this study is to evaluate the efficacy, safety, and ordering practices of phenobarbital in comparison to Benzodiazepines for alcohol withdrawal on general medicine floors and whether modifications to the alcohol withdrawal treatment protocol at PSVMC are needed. This will be a single-center, retrospective, observational cohort study evaluating patients admitted outside of the ICU and emergency department settings at PSVMC. Patients will be included if they are greater than 18 years of age, non-ICU patients diagnosed with alcohol withdrawal syndrome and received either phenobarbital or a benzodiazepine for alcohol withdrawal. The primary endpoints for this study will be treatment failure, defined as ICU transfer, and time to resolution, defined as CIWA score < 9 sustained until discharge. Secondary endpoints will include hospital length of stay, medication-related adverse effects (e.g. respiratory depression, neurologic effects), average doses of phenobarbital and benzodiazepines, intubation rates, use of adjunct agents for alcohol withdrawal symptoms, and percent of patients who hit the phenobarbital protocol dose cap of 20 mg/kg IBW. Manual chart review and EPIC Slicer Dicer will be used to identify patients and retrieve data from the electronic health record. Descriptive statistics will be used to describe baseline characteristics of study population, efficacy, and safety for both the benzodiazepines and phenobarbital groups. A chi-square test will be used to evaluate categorical data while a t-test will be used for numerical outcomes. Results and conclusions will be shared when the project is completed. (IRB approved). Learning Objectives: Evaluate the efficacy, safety, and ordering practices of phenobarbital in comparison to benzodiazepines for alcohol withdrawal on the general medicine floors. Presentation Category: Inpatient clinical services
-

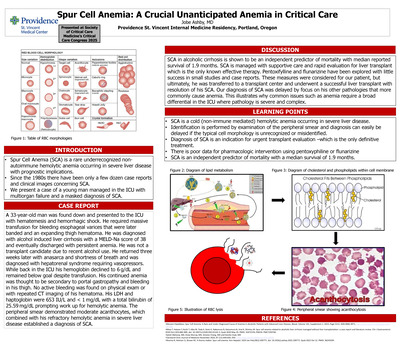
Spur Cell Anemia: A Crucial Unanticipated Anemia in Critical Care
Jobe Ashby
INTRODUCTION: Spur Cell Anemia (SCA) is a rare underrecognized non-autoimmune hemolytic anemia occurring in severe liver disease with prognostic implications. Since the 1980s there have been only a few dozen case reports and clinical images concerning SCA. We present a case of a young man managed in the ICU with multiorgan failure and a masked diagnosis of SCA. DESCRIPTION: A 33-year-old man was found down and presented to the ICU with hematemesis and hemorrhagic shock. He required massive transfusion for bleeding esophageal varices that were later banded and an expanding thigh hematoma. He was diagnosed with alcohol induced liver cirrhosis with a MELD-Na score of 38 and eventually discharged with persistent anemia. He was not a transplant candidate due to recent alcohol use. He returned three weeks later with anasarca and shortness of breath and was diagnosed with hepatorenal syndrome requiring vasopressors. While back in the ICU his hemoglobin declined to 6 g/dL and remained below goal despite transfusion. His continued anemia was thought to be secondary to portal gastropathy and bleeding in his thigh. No active bleeding was found on physical exam or with repeated CT imaging of his hematoma. His LDH and haptoglobin were 653 IU/L and < 1 mg/dL with a total bilirubin of 25.59 mg/dL prompting work up for hemolytic anemia. The peripheral smear demonstrated moderate acanthocytes, which combined with his refractory hemolytic anemia in severe liver disease established a diagnosis of SCA. DISCUSSION: SCA in alcoholic cirrhosis is shown to be an independent predictor of mortality with median reported survival of 1.9 months. SCA is managed with supportive care and rapid evaluation for liver transplant which is the only known effective therapy. Pentoxifylline and flunarizine have been explored with little success in small studies and case reports. These measures were considered for our patient, but ultimately, he was transferred to a transplant center and underwent a successful liver transplant with resolution of his SCA. Our diagnosis of SCA was delayed by focus on his other pathologies that more commonly cause anemia. This illustrates why common issues such as anemia require a broad differential in the ICU where pathology is severe and complex
-

Ofatumumab Associated Legionella Pneumonia in a Young Multiple Sclerosis Patient
Jobe Ashby and Omar Panhair
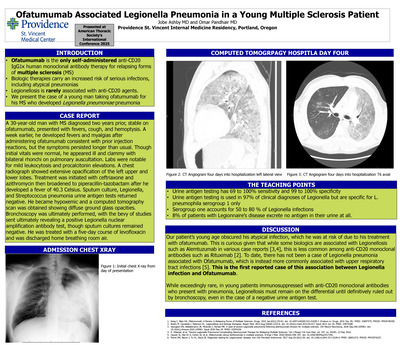
Ofatumumab is the only anti-CD20 IgG1κ human monoclonal antibody therapy for relapsing forms of multiple sclerosis (MS) that patients can self-administer subcutaneously. Anti-CD20 agents are biologic therapies that carry an increased risk of serious infections, but rarely Legionellosis. We present the case of a young man taking ofatumumab for his MS who developed Legionella pneumoniae pneumonia. A 30-year-old man with MS diagnosed two years prior, stable on ofatumumab, presented with fevers, cough, and hemoptysis. A week earlier, he developed fevers and myalgias after administering ofatumumab, but these symptoms persisted longer than usual. Though initial vital signs were normal, he appeared ill and clammy and had bilateral rhonchi on pulmonary auscultation. There was leukocytosis and an elevated procalcitonin level. A chest radiograph showed extensive opacification of the left upper and lower lobes. Treatment with ceftriaxone and azithromycin was initiated. Overnight, he developed a high fever to 40.3 Celsius and treatment was broadened to piperacillin-tazobactam. Sputum culture and urine antigen tests for Legionella and Streptococcus pneumonia were negative. Days later he became hypoxemic, and a computed tomography scan was obtained showing diffuse ground glass opacities. Bronchoscopy was ultimately performed, ultimately revealing a positive Legionella nuclear amplification antibody test, though sputum cultures remained negative. He was treated with levofloxacin for a five-day course with improvement and discharged breathing room air. Our patient’s young age belied his atypical infection, which he was at risk of due to his ofatumumab. While some biologics are associated with Legionellosis such as alemtuzumab, this is less common among anti-CD20 therapies like rituximab. While ofatumumab has been associated with upper respiratory tract infections, this is the first report of an association with Legionella. The final diagnosis in our case was delayed because the Legionella urine antigen testing was negative. Urine antigen testing is commonly used to rule out Legionella as a cause of atypical pneumonia; Urine antigen testing is used in 97% of clinical diagnoses. However, this test is not definitive, despite 69 to 100% sensitivity and 99 to 100% specificity, because it is specific for L. pneumophila serogroup 1 only. Serogroup 1 accounts for 50 to 80 % of Legionella infections and 8% of patients with Legionnaire’s disease excrete no antigen in their urine. This first report demonstrates that in patients immunosuppressed with anti-CD20 therapies presenting with pneumonia, Legionellosis must be considered until definitively ruled out by bronchoscopy, even when urine antigen testing is negative.
-

Idiopathic Systemic Capillary Leak Syndrome with Shock and Compartment Syndrome Due to Influenza A
Jobe Ashby, MD; Katelyn Bobrowski, DO; and Ryan Best, MD
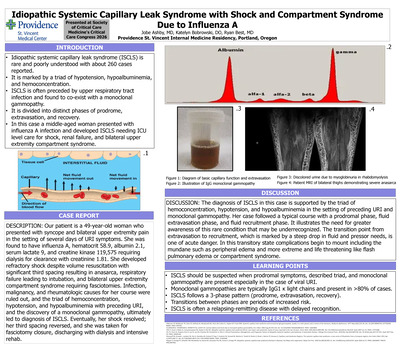
INTRODUCTION: Idiopathic systemic capillary leak syndrome (ISCLS) is a rare, poorly understood condition that leads to extreme pathology with severe but predictable complications. First described in 1960, ISCLS has been identified in about 260 case reports and is marked by a triad of hypotension, hypoalbuminemia, and hemoconcentration often preceded by upper respiratory tract infection. It is divided into distinct phases of prodrome, extravasation, and recovery. We present a case of a middle-aged woman who presented with influenza A infection and developed ISCLS needing ICU level care for shock and bilateral upper extremity compartment syndrome. DESCRIPTION: Our patient is a 49-year-old woman who presented with syncope and bilateral upper extremity pain in the setting of several days of URI symptoms. She was found to have influenza A, hematocrit 58.9, albumin 2.1, serum lactate 9, and creatine kinase 119,575 requiring dialysis for clearance with creatinine 1.81. She developed refractory shock despite volume resuscitation with significant third spacing resulting in anasarca, respiratory failure leading to intubation, and bilateral upper extremity compartment syndrome requiring fasciotomies. Infection, malignancy, and rheumatologic causes for her course were ruled out, and the triad of hemoconcentration, hypotension, and hypoalbuminemia with preceding URI, and the discovery of a monoclonal gammopathy, ultimately led to diagnosis of ISCLS. Eventually, her shock resolved; her third spacing reversed, and she was taken for fasciotomy closure, discharging with dialysis and intensive rehab. DISCUSSION: The diagnosis of ISCLS in this case is supported by the triad of hemoconcentration, hypotension, and hypoalbuminemia in the setting of preceding URI and monoclonal gammopathy. Her case followed a typical course with a prodromal phase, fluid extravasation phase, and fluid recruitment phase. It illustrates the need for greater awareness of this rare condition that may be underrecognized. The transition point from extravasation to recruitment, which is marked by a steep drop in fluid and pressor needs, is one of acute danger. In this transitory state complications begin to mount including the mundane such as peripheral edema and more extreme and life threatening like flash pulmonary edema or compartment syndrome.
-

Phenazopyridine-induced sulfhemoglobinemia: A diagnostic and management dilemma
Natalie Bolton, MD; Linh Tang Taylor, MD; Kristy Poonyagarlyagorn, MD; and Cameron Long, MD
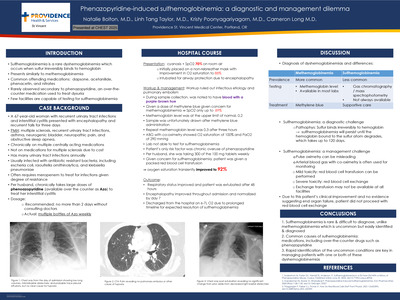
Introduction: Sulfhemoglobinemia is a rare dyshemoglobinemia which occurs when sulfur irreversibly binds to hemoglobin. Presents similarly to methemoglobinemia. Common offending medications: dapsone, acetanilide, phenacetin, and nitrates. Rarely observed secondary to phenazopyridine, an over-the counter medication used to treat dysuria. Few facilities are capable of testing for sulfhemoglobinemia Case Background: A 67-year-old woman with recurrent urinary tract infections and interstitial cystitis presented with encephalopathy and recurrent falls for three days. PMH: multiple sclerosis, recurrent urinary tract infections, asthma, neurogenic bladder, neuropathic pain, and obstructive sleep apnea. Chronically on multiple centrally acting medications. Not on medications for multiple sclerosis due to cost. Has many urinary tract infections annually Usually infected with antibiotic resistant bacteria, including escheria coli, raoultella ornithinolytica, and klebsiella pneumoniae. Often requires meropenem to treat for infections given degree of resistance. Per husband, chronically takes large doses of phenoazopyridine (available over the counter as Azo) to treat her interstitial cystitis Dosage: Recommended: no more than 2 days without consulting doctors Actual: multiple bottles of Azo weekly Conclusion: 1. Sulfhemoglobinemia is rare & difficult to diagnose, unlike ethemoglobinemia which is uncommon but easily identified & diagnosed 2. Common causes of sulhemoglobinemia: medications, including over-the counter drugs such as phenazopyridine 3. Rapid identification of the uncommon conditions are key in managing patients with one or both of these dyshemoglobinemias
-
 Infection by Natalie Bolton and Jeffrey Youker")
A Rare and Fatal Complication of Herpes Simplex Virus (HSV) Infection
Natalie Bolton and Jeffrey Youker
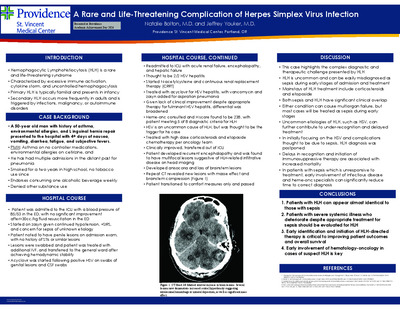
Introduction: Hemophagocytic Lymphohistiocytosis (HLH) is a rare syndrome characterized by overactive immune activation, cytokine storm, and uncontrolled hemophagocytosis. Primary HLH is familial and most often seen in infants, whereas secondary HLH occurs more frequently in adults and is triggered by infections, malignancies, or autoimmune disorders. Clinically, secondary HLH often mimics sepsis but fails to respond to standard therapies, contributing to delayed diagnosis and treatment. Without timely intervention, HLH can result in extensive tissue damage, multiorgan failure, and death. In rare cases, central nervous system (CNS) involvement may occur, manifesting as histiocytic infiltration that can be misinterpreted as malignancy or infection. Case Presentation: A 51 year-old man presented with four days of nausea, vomiting, diarrhea, and fevers. Initial evaluation revealed persistent hypotension, severe transaminitis, neutropenia, thrombocytopenia, and penile lesions, prompting ICU admission. Hemodynamic stability was achieved with fluid administration and empiric antibiotics, after which the patient was transferred to the general ward and started on acyclovir following positive HSV results from genital lesion swabs and CSF samples. Subsequently, the patient developed acute renal failure, encephalopathy, and hepatic failure, suspected to be secondary to HSV hepatitis, necessitating ICU readmission. Due to the severity of organ dysfunction, N-acetyl-cysteine and continuous renal replacement therapy (CRRT) were initiated. Although HLH was initially considered unlikely due to its rare association with HSV, further evaluation confirmed the diagnosis. The patient was treated with high-dose steroids and etoposide chemotherapy, resulting in clinical improvement and transfer out of critical care. However, the patient later experienced recurrent encephalopathy. Brain MRI revealed multifocal lesions suggestive of HLH related infiltrative disease. Neurologic deterioration progressed to anisocoria and loss of brainstem reflexes, and repeat CT imaging revealed new lesions with mass effect and brain stem compression. Despite aggressive management, the patient succumbed to the disease. Discussion: This case underscores a complex diagnostic and therapeutic challenge involving a rare etiology of HLH. The clinical overlap between HLH and sepsis, both capable of causing multiorgan failure, contributes to under-recognition and delayed treatment. Initial management focused on treating HSV infection and its complications, which inadvertently postponed HLH diagnosis. Delayed recognition and initiation of immunosuppressive therapy, including corticosteroids and etoposide, are associated with increased mortality. Conclusions: This case highlights the importance of maintaining a high index of suspicion for HLH in patients with severe systemic illness, particularly when clinical deterioration persists despite appropriate treatment for presumed sepsis. Early identification and prompt initiation of HLH-directed therapy are critical to improving outcomes.
-

The Rash After the Remedy
Elaine Chen, MD
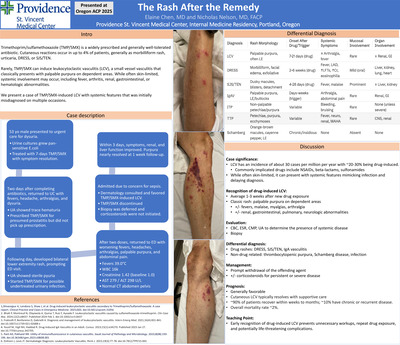
Introduction: Trimethoprim/sulfamethoxazole (TMP/SMX) is a widely prescribed and generally well-tolerated antibiotic. Cutaneous reactions occur in up to 4% of patients, including morbilliform rash, urticaria, DRESS, Stevens-Johnson syndrome, and toxic epidermal necrolysis. More rarely, TMP/SMX can trigger leukocytoclastic vasculitis (LCV), a small-vessel vasculitis characterized by neutrophilic infiltration, fibrinoid necrosis, and leukocytoclasia. LCV typically manifests as palpable purpura on dependent areas. While often skin-limited, systemic involvement may occur. We present a case of TMP/SMX-induced LCV with multi-organ features. Case description: A 53-year-old healthy male presented to urgent care with dysuria. Urine culture grew pan-sensitive E. coli, and he completed a 7-day course of TMP/ SMX with symptom resolution. Two days later, he returned with fevers, headaches, arthralgias, and dysuria. Urinalysis showed trace hematuria, and he was re-prescribed TMP/SMX for presumed prostatitis. Before restarting, his fevers improved but he developed a bilateral lower-extremity rash, prompting ED evaluation. TMP/SMX was re-prescribed a third time for possible undertreated infection. After two doses, he returned with worsening fevers, headaches, arthralgias, progressive palpable purpura, and abdominal pain. He was febrile to 39.0°C with creatinine 1.42 mg/dL (baseline 1.0), WBC 16K, Hgb 12 g/dL, platelets 127K, AST 279 U/L, ALT 298 U/L, and was admitted for concern of sepsis. Dermatology was consulted and favored TMP/SMX induced LCV. Biopsy was deferred, and corticosteroids were not initiated. Following drug discontinuation, his symptoms and renal function improved within 3 days, and purpura nearly resolved at 1 week. Discussion: LCV is rare, with an incidence of ~30 per million annually, and 10-20% of cases being drug-induced. Other causes of LCV include infections, autoimmune disorders, malignancies, and idiopathic. Symptoms typically arise within 1-3 weeks of exposure and present with palpable purpura, sometimes accompanied by fever, arthritis, renal, gastrointestinal, or hematologic involvement. The diagnosis here was supported by the classic rash, temporal association with TMP/SMX, worsening on re-exposure, and rapid improvement after withdrawal. Other TMP/SMX reactions were considered, as it can cause hepatitis, and a physiologic creatinine elevation of ~17-31% via inhibition of tubular secretion. This patient’s creatinine exceeded that range and coincided with palpable purpura, supporting LCV rather than DRESS or TEN/SJS. Drug-induced IgA vasculitis was also possible, as it can mimic LCV with multi-organ involvement. In this case, drug-induced LCV was favored, as IgA vasculitis is rarer. Management is drug withdrawal, with resolution usually within 2-3 weeks. Corticosteroids are reserved for severe or refractory disease. The prognosis is favorable with prompt withdrawal of the drug. TMP/SMX-induced LCV is a rare but important adverse reaction. Clinicians should suspect it in patients with new palpable purpura after medication exposure. Early recognition and drug withdrawal are crucial to prevent repeat exposure, unnecessary testing, and serious complications.
-

Snuggles, not struggles: evaluation of a post-operative pain management protocol in a level III community NICU
MaLeane Chin, Danielle Megano, Aiyana Ooki-Knutson, and Deasy Erin Wilson
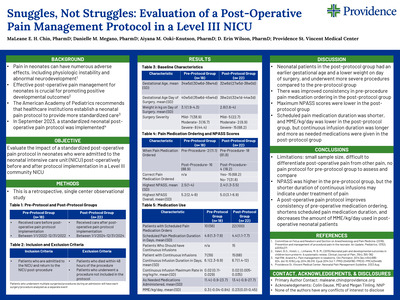
Abstract: Neonates are an extremely sensitive population often subject to painful interventions. This pain can have numerous adverse effects including physiologic instability, altered brain development, and abnormal stress responses, which can persist into childhood. Effective post-operative pain management for neonates is crucial for promoting positive developmental outcomes. No specific post-operative pain protocol for neonatal patients has shown to be most effective, so the American Academy of Pediatrics recommends that healthcare institutions establish a neonatal pain protocol to provide more standardized care. This project is a retrospective, single center observational study determined to be exempt by the institutional review board. Infants cared for in a Level III community neonatal intensive care unit (NICU) between January 1, 2022 and December 31, 2022 receiving post-operative care prior to the implementation of a standardized post-operative pain protocol, and between January 1, 2024 and December 31, 2024 receiving post-operative care after the implementation of a standardized post-operative pain protocol will be identified. Infants with pain following procedures not included in the policy and patients who died within 48 hours of the procedure will be excluded. Data collected will include gestational age at birth, corrected gestational age on date of surgery, weight, date and type of operation, operating surgeon, adherence to protocol, NPASS scores, total amount of morphine milligram equivalents, duration of continuous analgesic infusions and scheduled pain medications, number of as needed analgesics administered, and post-operative complications. Based on this information, the impact and clinical outcomes of a standardized postoperative pain protocol in a level III community NICU can be evaluated. Results and conclusions will be presented. Learning Objectives: Evaluate the impact of a standardized post-operative pain protocol in neonates who were admitted to the neonatal intensive care unit (NICU) post-operatively before and after protocol implementation in a Level III community NICU Presentation Category: Pediatrics
-

Efficiency Rx: EMR Training for Resident Wellness
Calder Dorn, DO; Tom Chau, MD, MBA, FACP; and Shelley Sanders, MD, FACP
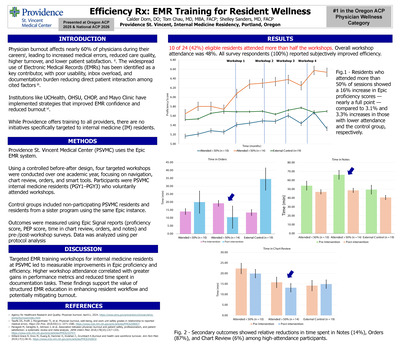
Introduction: Physician burnout affects nearly 60% of physicians during their careers, leading to increased medical errors, reduced care quality, higher turnover, and lower patient satisfaction. ii. The widespread use of Electronic Medical Records (EMRs) has been identified as a key contributor, with poor usability, inbox overload, and documentation burden reducing direct patient interaction among cited factors iii. Institutions like UCHealth, OHSU, CHOP, and Mayo Clinic have implemented strategies that improved EMR confidence and reduced burnout vi. While Providence offers training to all providers, there are no initiatives specifically targeted to internal medicine (IM) residents. Methods: Providence St. Vincent Medical Center (PSVMC) uses the Epic EMR system. Using a controlled before-after design, four targeted workshops were conducted over one academic year, focusing on navigation, chart review, orders, and smart tools. Participants were PSVMC internal medicine residents (PGY1–PGY3) who voluntarily attended workshops. Control groups included non-participating PSVMC residents and residents from a sister program using the same Epic instance. Outcomes were measured using Epic Signal reports (proficiency score, PEP score, time in chart review, orders, and notes) and pre-/post -workshop surveys. Results: Overall workshop attendance among residents was 48%. Residents who attended more than 50% of sessions showed a 16% increase in Epic proficiency scores—nearly a full point—compared to 3.1% and 3.3% increases in those with lower attendance and the control group, respectively. Secondary outcomes showed relative reductions in time spent in Notes (14%), Orders (87%), and Chart Review (6%) among high-attendance participants. All survey respondents (100%) reported subjectively improved efficiency from the workshops. Conclusion: \Targeted EMR training workshops for internal medicine residents at PSVMC led to measurable improvements in Epic proficiency and efficiency. Higher workshop attendance correlated with greater gains in performance metrics and reduced time spent in documentation tasks. These findings support the value of structured EMR education in enhancing resident workflow and potentially mitigating burnout.
-

Pulmonary Pseudomyxoma Peritonei
Hannah Kirk, DO and Omar Pandhair
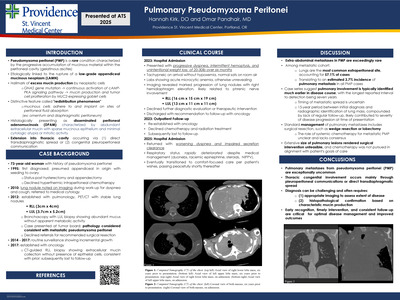
Introduction: Pseudomyxoma peritonei (PMP) is an intra -abdominal cancer occurring in one to four out of one million patients. It begins as a mucinous adenocarcinoma of the appendix that implants on other peritoneal surfaces, spreading into gelatinous ascites. Treatment consists of hyperthermic intraperitoneal chemotherapy (HIPEC) and cytoreductive surgery (CRS). Extra -abdominal metastases are rare. We present the case of a patient who underwent treatment for PMP and was found to have lung nodules over a decade later. Case Presentation: A 73 -year -old woman with pseudomyxoma peritonei presented to the emergency department with progressive dyspnea and unintentional weight loss. Twenty -eight years earlier she was found to have appendiceal pseudomyxoma peritonei with extension to her right ovary and underwent CRS, though she didn't receive HIPEC. Fifteen years later, she was noted to have lung nodules and underwent bronchoscopy with biopsy that revealed mucinous cystic lesions. Body -wide imaging was negative for recurrence or other metastases. She was monitored with serial imaging that showed stable sized nodules approximately 5 x 3.5 cm in the right lower lobe and 5 x 4 cm in the left upper lobe. She presented seven years later with twenty -pound weight loss, progressive dyspnea on exertion, and intermittent hemoptysis. She was borderline tachycardic without hypoxemia and newly anemic with a three -point hemoglobin drop to 8.9 g/dL. Computed tomography of the chest showed a right - sided mass 15.3 x 14.9 x 19 cm in size and a left -upper mass 12.9 x 11.3 x 11 cm in size with compression of adjacent bronchi and vasculature. Discussion: Extra -abdominal metastases of PMP are exceedingly rare. Within the metastatic cohort, the lungs accounted for 57.1% of cases, suggesting 3.7% of PMP cases developed pulmonary metastases. While it is unclear when our patient first developed pulmonary metastases, a case series suggests these are usually identified much earlier, with the longest time to discovery of lung metastasis being seven years. This is likely why our patient's masses grew to such a significant size, as none of the metastases identified in case series was even half the size of hers. Unfortunately, treatment of pulmonary metastases is usually accomplished with wedge resection or lobectomy, and our patient's masses had grown so large that this was unfeasible. While it is unclear whether systemic chemotherapy has a role in the treatment of metastatic PMP, the patient discussed a trial with oncology and elected to forego any further workup or treatment.
-

Implementation and Impact of the Transition Series for Senior Residents in Internal Medicine Residency
Abby Lindseth, MD and Jeffrey Youker
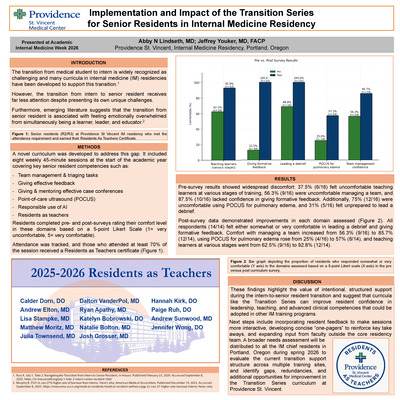
The transition from medical student to intern is widely recognized as a challenging period, and numerous curricula have been developed to support this transition. However, the transition from intern to senior resident receives far less attention despite presenting its own unique challenges. Anecdotal feedback from internal medicine residents and emerging literature suggests that the transition to senior resident is associated with feeling emotionally overwhelmed from simultaneously being a learner, leader and educator.1,2 To address this gap, the Transition Series was developed as a novel curriculum to support internal medicine residents as they advance into their senior roles. Building on the existing Intern Only series, the Transition Series emphasized leadership development, strategies for teaching, and advanced clinical skills not typically covered during intern year. By providing dedicated time for developing these skills, the curriculum aimed to enhance senior resident preparedness, confidence, and well-being in their new roles. The curriculum consisted of eight weekly 45-minute sessions at the start of the academic year, covering key senior resident competencies: team management, giving effective feedback, tools for giving and mentoring morning reports, point-of-care ultrasound (POCUS), residents as teachers, leading a debrief, and the responsible use of AI in medicine and medical education. Residents completed pre- and post-surveys rating their comfort in these domains (1 = very uncomfortable, 5 = very comfortable). Attendance was tracked, and those who attended at least 70% of the sessions received a Residents as Teacher certificate. Pre-survey results showed widespread discomfort: 37% (6/16) felt uncomfortable teaching learners at various stages, 56% (9/16) were uncomfortable managing a team, and 87.5% (10/16) lacked confidence in giving formative feedback. Additionally, 75% (12/16) were uncomfortable using POCUS for pulmonary edema, and 31% (5/16) felt unprepared to lead a debrief. Post-survey data demonstrated improvements in each domain assessed. All respondents (14/14) felt either somewhat or very comfortable in leading a debrief and giving formative feedback. Comfort with managing a team increased from 56.3% (9/16) to 85.7% (12/14), using POCUS for pulmonary edema rose from 25% (4/16) to 55.6% (5/9), and confidence in team management went from 43.8% (7/16) to 77.8% (7/9). These findings highlight the value of intentional, structured support during the intern-to senior resident transition and suggest that curricula like the Transition Series can significantly improve resident confidence in leadership, teaching, and advanced clinical competencies. Beyond the quantitative improvements, the series fostered a sense of community and validation among residents navigating their new responsibilities. A personal lesson learned through this project is the power of using lived experience to drive meaningful change and the importance of creating space for emerging educators to shape the systems they are a part of. Having just completed residency, I was uniquely positioned to prioritize topics that felt most relevant in real time. This perspective allowed me to design a curriculum that directly addressed the gaps I had experienced, and to advocate for a more learner-centered approach to resident development. Moving forward, resident feedback will be incorporated into the sessions to make them more interactive and include concise “one-pagers” to reinforce take-home points and support diverse learning styles. I also hope to broaden the scope of input by inviting perspectives from outside the residency core faculty, including subspecialists and recent graduates who have just experienced the transition. To further refine this curriculum and enhance the project’s reach, a focused needs assessment will be distributed to multiple internal medicine residency programs to better understand the challenges of this transition and refine the curriculum to meet evolving learner needs.
-

An Atypical Presentation of Metastatic Gastric Adenocarcinoma Due to Pulmonary Lymphangitic Carcinomatosis
Matthew Moritz and Omar Pandhair
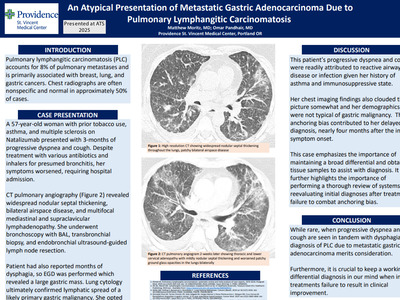
Pulmonary lymphangitic carcinomatosis (PLC) accounts for approximately 8% of pulmonary metastases and is primarily associated with breast, lung, and gastric cancers. Chest radiographs are often nonspecific and normal in approximately 50% of cases. We present a case of PLC as an initial presentation of metastatic gastric adenocarcinoma. A 57-year-old White woman with prior tobacco use, asthma, and multiple sclerosis on Natalizumab presented with three months of progressive dyspnea and cough. She was evaluated multiple times and treated with various antibiotics and inhalers for presumed bronchitis. Despite this, her symptoms worsened, prompting hospital evaluation. She was tachycardic and markedly hypoxemic on arrival. A high-resolution computed tomography (CT) scan revealed widespread nodular septal thickening, bilateral airspace disease, and multifocal mediastinal and supraclavicular lymphadenopathy most concerning for lymphoma or atypical infection. She underwent bronchoscopy with bronchoalveolar lavage, transbronchial biopsy, and endobronchial ultrasound guided lymph node resection. She also reported progressive dysphagia with solid foods and significant weight loss over the prior months, so esophagogastroduo denoscopy was performed with pathology showing a poorly differentiated adenocarcinoma. Lung cytology confirmed lymphatic spread of a likely primary gastric malignancy. She opted to discharge on hospice. Given our patient’s asthma and immunosuppressive therapy, her progressive dyspnea and cough were easily readily attributed to reactive airway disease or infection. Her chest imaging findings also clouded the picture somewhat and her demographics were not typical of gastric malignancy as it is half as common in women and has very low prevalence in the non-Hispanic White population. Natalizumab therapy was also not associated with increased risk of malignancy in a recent cohort study. This anchoring bias contributed to her delayed diagnosis, as her weight loss and dysphagia were not uncovered until she was hospitalized, four months after the initial symptom onset. In a similar case, a man presenting with respiratory symptoms whose imaging showed only bilateral ground-glass opacities was felt to have non-malignant disease until trans-bronchial biopsy revealed metastatic gastric adenocarcinoma. Both cases emphasize the importance of maintaining a broad differential and obtaining tissue samples to assist with diagnosis. Our case highlights the importance of performing a thorough review of systems and reevaluating initial diagnoses after initial treatment failure to combat anchoring bias. When progressive dyspnea and cough are seen in tandem with dysphagia, the otherwise very rare diagnosis of PLC due to metastatic gastric adenocarcinoma merits consideration.
-

ECMO as a Bridge to Lung Transplant for Refractory Rapidly Progressive Interstitial Lung Disease
Matthew Moritz and Omar Pandhair
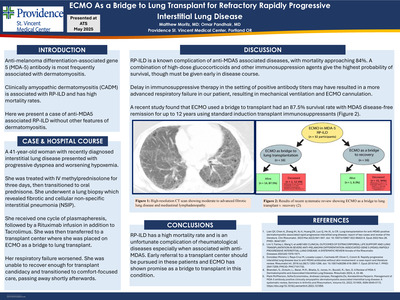
Anti-melanoma differentiation-associated gene 5 (MDA-5) antibody is most frequently associated with dermatomyositis with various degrees of clinical manifestations including rapidly progressive interstitial lung disease (RP-ILD), inflammatory arthritis, vasculopathy, and other cutaneous findings. Clinically amyopathic dermatomyositis (CADM) is frequently associated with RP-ILD and has high mortality rates. Here we present a case of anti-MDA5 associated RPILD but without other features of dermatomyositis that did not respond to standard immunosuppressive therapy. A 41-year-old woman with recently diagnosed interstitial lung disease and polyarthritis previously on methotrexate presented with progressive dyspnea and worsening hypoxemic respiratory failure. She was previously admitted for respiratory failure two months prior where high resolution CT revealed moderate to advanced fibrotic lung disease and mediastinal lymphadenopathy and was discharged on a prolonged prednisone taper. Previous studies revealed a positive MDA5 antibody. She was treated initially with intravenous methylprednisolone 1,000 mg for three days then transitioned to oral prednisone. Lung biopsy revealed fibrotic and cellular non-specific interstitial pneumonia (NSIP). She received one cycle of plasma pheresis, followed by a Rituximab infusion in addition to Tacrolimus. She was then transferred to a transplant center where she was placed on veno-arterial venous extracorporeal membrane oxygenation (ECMO) as a bridge to lung transplant. Unfortunately, her respiratory failure worsened, requiring ECMO reconfiguration. She was unable to recover enough for transplant candidacy and transitioned to comfort-focused care, passing away shortly afterwards. RP-ILD is a known complication of anti-MDA5 associated diseases, with mortality approaching 84%. A combination of high-dose glucocorticoids and other immunosuppression agents give the highest probability of survival, though they must be administered early in the disease course. Our patient had a delay in additional immunosuppressive therapy, despite positive antibody titers two months prior, which may have resulted in a more advanced respiratory failure and hypoxemia on presentation, ultimately requiring mechanical ventilation and subsequent ECMO cannulation. A systematic review published in Annals of Rheumatology found that ECMO used a bridge to transplant had an 87.5% survival rate with MDA5 disease-free remission for up to 12 years using standard induction transplant immunosuppressants, which a more recent case report in CHEST exemplified. Our case emphasizes the importance of early antibody screening and prompt initiation of appropriate immunosuppressive therapy to avoid transformation to RP-ILD. Early referral to a transplant center should be pursued in these patients as ECMO has shown promise as a bridge to transplant in this condition.
-

An Exploration of Drivers of Sepsis Outcomes in Racial and Ethnic Minority Populations
Matthew Moritz, Omar Pandhair, and Shelley Schoepflin Sanders
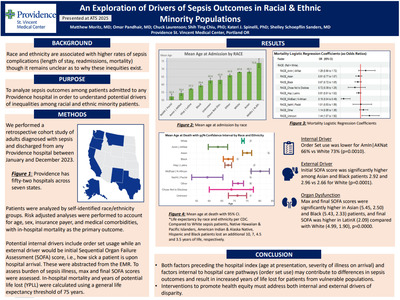
RATIONALE: Race and ethnicity affect sepsis outcomes in unclear ways. Existing data is conflicting, with some studies suggesting minority patients do worse, while others did not show a difference in outcomes between these groups. We sought to investigate whether inequalities exist in sepsis outcomes for different racial and ethnic groups in our large hospital system and to characterize how they may manifest. METHODS: We performed a retrospective cohort study of adults diagnosed with sepsis and discharged from any of Providence’s 52 hospitals between January 1 and December 31, 2023. We grouped patients into ten different race/ethnicity groups including White, Black, Hispanic/Latinx, Black, Asian, Middle Eastern/North African, American Indian/Alaska Native, and other/ unknown/chose not to disclose. Patient age, gender, insurance payer, and medical comorbidity groups were determined. In-hospital mortality, hospital length of stay (LOS), 30-day readmission rate, lactic acid level, sepsis order set usage, and initial, final, and maximum sequential organ failure assessment (SOFA) scores were abstracted from the electronic medical record. RESULTS: We identified 44,443 sepsis patients, of whom the mean age was 65.3 years and 52.7% were male. 65.2% were White, 17.0% were Hispanic/Latinx, 5.2% were Asian, 4.1% were Black, and 1.3% were Native American. White (67.9 years) and Asian (68.1 years) patients were of similar average age, while Black (59.4 years), Hispanic (57.2 years), and Native American (54.4 years) patients were younger. Hispanic/ Latinx patients had a 2.46% lower mortality rate (p < 0.0001) than White patients. Black patients had a LOS of 0.63 days longer (p < 0.0001) than White patients on average, while Hispanic patients had a 0.51-day shorter LOS (p< 0.0001). Readmission rates were similar across groups. Black and Asian patients had higher initial, maximum, and final SOFA scores than Whites (p < 0.0001). Asian patients also had a higher lactic acid level by 0.13 mmol/L (p = 0.0001) than White patients. CONCLUSIONS: We noted a significant difference in the average age of each race/ethnicity group, meaning that despite similar mortality rates, Black and Native American patients on average present and die younger of sepsis than White patients. Similarly, age may account for much of the mortality benefit associated with the Hispanic/Latinx group. Further study investigating years of potential life lost may help better elucidate these disparities. Disparities in the severity of presenting illness of Black and Asian patients may be due to delayed recognition in the prehospital setting.
-

Pulmonary Prelude: ILD as the Only Manifestation of Rheumatoid Arthritis
Matthew Moritz, MD
Abstract: Rheumatoid arthritis (RA), a systemic autoimmune disorder, classically presents with joint pain and prolonged morning stiffness. Extra-articular pulmonary manifestations are frequently observed but can be the primary initial presentation. We present a case of a women with chronic RA in remission who presented with shortness of breath and was found to have new RA-associated interstitial lung disease (RA-ILD). A 74-year-old female with a history of rheumatoid arthritis in remission, chronic obstructive pulmonary disease, and recent admission for septic shock presented with progressive dyspnea and hypoxia. Initial vitals noted an oxygen saturation in the low 80s. CT pulmonary angiography excluded pulmonary embolism but demonstrated significant interval progression of basilar predominant pulmonary fibrosis with subpleural reticular opacities compared to imaging seven months prior. Pulmonology was consulted and recommended high-dose prednisone (1 mg/kg). Serologic evaluation revealed elevated anti-cyclic citrullinated peptide(> 250 U/ml) and rheumatoid factor(> 500 IU/ml), with a negative hypersensitivity pneumonitis panel. Rheumatology agreed with mycophenolate monotherapy given lack of synovial involvement. Despite therapy, her respiratory status declined, necessitating heated high-flow nasal cannula support. Repeat chest imaging showed worsening ground-glass opacities, prompting escalation to high-dose intravenous methylprednisolone, which led to gradual clinical improvement. She transitioned to an oral prednisone taper, weaned to 6 L nasal cannula, and discharged with close pulmonology and rheumatology follow-up. RA-ILD chest CT findings are variable but most commonly demonstrate usual interstitial pneumonia (UIP) or nonspecific interstitial pneumonia (NSIP) patterns, although organizing pneumonia and rheumatoid nodules are also well described. While RA-ILD typically develops within five years of RA onset, our patient exhibited pulmonary manifestations decades after diagnosis, highlighting the marked heterogeneity in disease presentation. Furthermore, the absence of articular involvement further distinguishes this case, as most patients with RA-ILD exhibit at least some degree of joint disease. The presence of markedly elevated rheumatoid factor and anti-cyclic citrullinated peptide (anti-CCP) antibodies supported the diagnosis in this case and aligned with known associations between serologic activity and extra-articular disease expression. Current treatment strategies for RA-ILD emphasize systemic steroids and DMARDs, and like our patient, most receive high-dose steroids for management of acute flare, though augmentation with mycophenolate was selected given the predominance of pulmonary involvement. Since there are no dedicated randomized controlled trials in this area, treatment is based on observational data and expert opinion and should include a multidisciplinary approach to optimize patient outcomes.
-

Behavior Change in a Young Woman: The Secret Lies in the Ovarian Tumor
Matthew Moritz, MD; Linh Tang Taylor, MD; Olivia L Snir; and Stephanie Griffith, MD
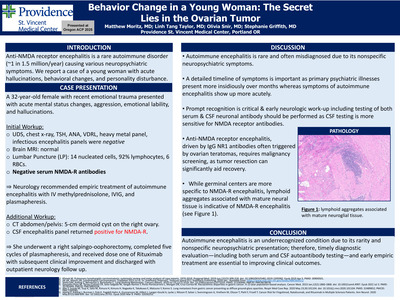
Introduction: Autoimmune encephalitis is a rare immune-mediated disorder characterized by neuropsychiatric symptoms. Anti-NMDA receptor (NMDA-R) encephalitis, the most common subtype, affects approximately 1 in 1.5 million people annually. We present a case of a young female with new-onset hallucinations, behavioral changes, and personality disturbance. Case Presentation: A 32-year-old female with remote methamphetamine use and recent trauma presented with acute mental status changes, aggression, emotional lability, and hallucinations. Vitals were normal; on exam she appeared confused, agitated, and displayed unusual behavior, including hallucinations. Initial evaluation revealed mild leukocytosis, but otherwise normal urine drug screen, chest radiograph, TSH, ANA, VDRL, heavy metal panel, infectious and autoimmune encephalitis panels, and brain MRI. Lumbar puncture (LP) revealed fourteen nucleated cells, ninety-two percent lymphocytes, and six red blood cells. Psychiatry was consulted but felt this was unlikely to represent a primary psychiatric disorder. Neurology recommended repeat LP and initiation of empiric methylprednisolone, IVIG, and plasmapheresis for presumed autoimmune encephalitis. CT abdomen/pelvis revealed a five-centimeter dermoid cyst on the right ovary. She underwent right salpingoopherectomy with pathology showing a cystic teratoma with mature neuronal tissue. The CSF encephalitis panel returned positive for NMDA-R. She completed five sessions of plasmapheresis and one dose of rituximab induction. Her agitation and behavioral disturbances were slow to resolve, requiring high-dose antipsychotics and benzodiazepines, but she was ultimately discharged with close outpatient neurology follow -up and a plan for a second rituximab dose. Discussion: Due to its rarity and nonspecific symptoms, autoimmune encephalitis is often overlooked in clinical practice. Furthermore, our patient’s age and recent traumatic experience prompted a primary psychiatric diagnosis to be pursued. This case underscores the importance of assessing symptom onset, as primary psychiatric disorders such as schizophrenia or bipolar disorder typically present with a more gradual, insidious onset— unlike the acute presentation seen in our case. When suspected, a basic workup should include a brain MRI, lumbar puncture, and neuronal autoantibody testing, though brain MRI findings may be normal. Both serum and CSF should be tested for neuronal autoantibodies, as CSF offers greater sensitivity—particularly for NMDA receptor antibodies, as demonstrated in our case where only CSF testing yielded a positive result. In anti-NMDA receptor encephalitis, IgG antibodies against NR1 are often triggered by neural tissue in ovarian teratomas via molecular mimicry. Once autoimmune encephalitis is diagnosed, evaluation for an underlying malignancy should follow, as treatment of a paraneoplastic process is integral to disease management. In our case, an ovarian teratoma—commonly associated with anti-NMDA receptor encephalitis—was identified and resected, contributing to clinical improvement
-

A Case of Pembrolizumab Associated SJS/TEN Spectrum Reaction
Lauryn Orsillo, DO; Alex Zhu, MD; and Linh Tang Taylor, MD
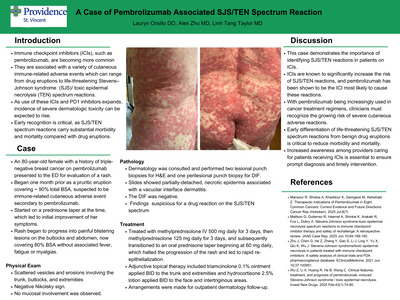
Introduction: Immune checkpoint inhibitors (ICIs), such as pembrolizumab, are becoming increasingly more common.1 They are associated with a variety of cutaneous immune-related adverse events which can range from drug eruptions to life-threatening Stevens–Johnson syndrome (SJS)/ toxic epidermal necrolysis (TEN) spectrum reactions.2 As use of these ICIs and PD1 inhibitors expands, the incidence of severe dermatologic toxicity can be expected to rise. Early recognition is critical, as SJS/TEN spectrum reactions carry substantial morbidity and mortality compared with drug eruptions. Case report: An 80-year-old female with a history of triple-negative breast cancer on pembrolizumab presented to the ED for evaluation of a worsening rash. She reported that the rash began approximately one month earlier as a pruritic eruption covering an estimated 90% total body surface area. Her oncologist suspected an immune-related cutaneous adverse event secondary to pembrolizumab, with her most recent dose administered one month prior to rash onset. She was started on a prednisone taper, which led to initial improvement of her symptoms. A few days prior to presentation, while still receiving the prednisone taper, the rash progressed and evolved into painful blistering lesions on the buttocks and abdomen, now covering 80% total body surface area. She denied associated fever, fatigue or myalgias. Physical examination revealed scattered vesicles and erosions involving the trunk, buttocks, and extremities, with a negative Nikolsky sign. No mucosal involvement was observed. Dermatology was consulted and performed two lesional punch biopsies for H&E and one perilesional punch biopsy for DIF. The slides were interpreted by a dermatopathologist and showed a partially-detached, necrotic epidermis associated with a vacuolar interface dermatitis. The DIF was negative. These findings were suspicious for a drug reaction in the SJS/TEN spectrum. The patient was treated with methylprednisolone IV 500 mg daily for three days, followed by methylprednisolone 125 mg daily for three days, and subsequently transitioned to an oral prednisone taper beginning at 60 mg daily, which halted the progression of the rash and led to rapid re-epithelialization. Adjunctive topical therapy included triamcinolone 0.1% ointment applied twice daily to the trunk and extremities and hydrocortisone 2.5% lotion applied twice daily to the face and intertriginous areas. Arrangements were made for outpatient dermatology follow-up. Discussion: This case demonstrates the importance of identifying SJS/TEN reactions in patients on ICIs. ICIs are known to significantly increase the risk of SJS/TEN reactions, and pembrolizumab has been shown to be the ICI most likely to cause these reactions. 2, 3 With pembrolizumab being increasingly used in cancer treatment regimens, clinicians must recognize the growing risk of severe cutaneous adverse reactions.1 Early differentiation of life-threatening SJS/TEN spectrum reactions from benign drug eruptions is critical to reduce morbidity and mortality. Increased awareness among providers caring for patients receiving ICIs is essential to ensure prompt diagnosis and timely intervention.
-

Evaluating Outcomes of Long-Acting Injectable Antiretrovirals for HIV Treatment and Pre-exposure Prophylaxis in a Pharmacist-Managed Clinic Setting
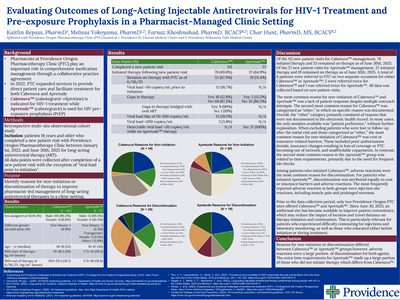
Kaitlin Repass, PharmD; Melissa Yokoyama, PharmD; Farnaz Khoshnahad, PharmD, BCACP; and Char Hunt, PharmD, MS, BCACP
-

When Common Isn’t Typical: A Diagnostic Twist in Hyperparathyroidism
Connor Shortt, DO* and Laura Loertscher, MD*
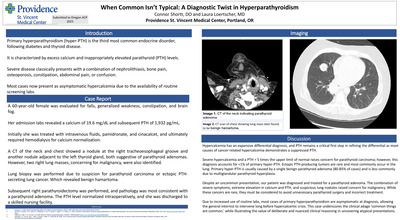
Introduction: Primary hyperparathyroidism is the third most common endocrine disorder, following diabetes and thyroid disease. It is characterized by excess calcium and inappropriately elevated parathyroid (PTH) levels. Severe disease classically presents with a combination of nephrolithiasis, bone pain, osteoporosis, constipation, abdominal pain, anxiety, depression, or confusion. However, due to the availability of routine labs, most cases now present as asymptomatic hypercalcemia. Case Description: A 60-year-old female was evaluated for falls, generalized weakness, constipation, and brain fog. Her admission labs revealed a calcium of 19.6 mg/dL and subsequent PTH of 1,932 pg/mL. She was treated with intravenous fluids, pamidronate, and cinacalcet, and ultimately required hemodialysis for calcium normalization. A CT of the neck and chest showed a nodule at the right tracheoesophageal groove and another nodule adjacent to the left thyroid gland, both suggestive of parathyroid adenomas. However, two right lung masses, concerning for malignancy, were also identified. In the setting of extreme hypercalcemia, a CT-guided lung biopsy was performed due to suspicion for parathyroid carcinoma or ectopic PTH-secreting lung cancer. Lung pathology revealed benign hamartoma. Subsequent right parathyroidectomy was performed, and pathology was most consistent with a parathyroid adenoma. The PTH level normalized intraoperatively, and she was discharged to a skilled nursing facility. Discussion: Hypercalcemia has an expansive differential diagnosis, and the magnitude of elevation influences the pretest probability for a cancer-related etiology. Severe hypercalcemia, defined as >14 mg/dL, raises concern for malignancy. PTH remains a critical first step in refining the differential as most causes of cancer-related hypercalcemia demonstrate a suppressed PTH. Severe hypercalcemia and a PTH > 5 times the upper limit of normal can raise concern for parathyroid carcinoma; however, this diagnosis accounts for < 1% of primary hyperparathyroid cases. Ectopic PTH-producing tumors are rare and most commonly occur in the lung. Primary hyperparathyroidism is usually caused by a single benign parathyroid adenoma (80-85% of cases) and is less commonly due to multiglandular parathyroid hyperplasia. Despite an uncommon presentation, our patient was ultimately diagnosed and treated for parathyroid adenoma. The combination of severe symptoms, extreme elevation in calcium and PTH, and suspicious lung nodules raised appropriate concern for malignancy. While these cancers are rare, they must be considered to avoid unnecessary parathyroid surgery and incorrect treatment. Due to increased use of routine labs, most cases of primary hyperparathyroidism are asymptomatic at diagnosis, allowing the general internist to intervene long before hypercalcemic crisis. This case underscores the clinical adage ‘common things are common,’ while illustrating the value of deliberate and nuanced clinical reasoning in uncovering atypical presentations.
-

Puzzling Papules: Uncovering the Etiology of a Rash in a Returning Traveler
Lisa Stampke, MD and Shahana Baig-Lewis, MD
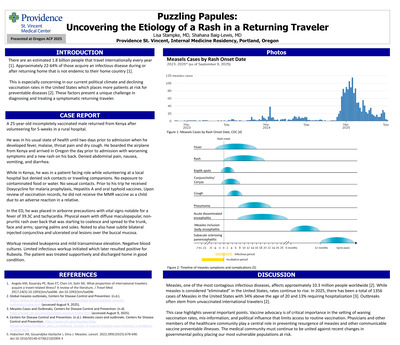
Introduction: There are an estimated 1.8 billion people that travel internationally every year [1]. Approximately 22-64% of those acquire an infectious disease during or after returning home that is not endemic to their home country [1]. This is especially concerning in our current political climate and declining vaccination rates in the United States which places more patients at risk for preventable diseases [2]. These factors present a unique challenge in diagnosing and treating a symptomatic returning traveler. Case Description: A 25-year-old incompletely vaccinated male returned from Kenya after volunteering for 5-weeks in a rural hospital. He was in his usual state of health until two days prior to admission when he developed fever, malaise, throat pain and dry cough. He boarded the airplane from Kenya and arrived in Oregon the day prior to admission with worsening symptoms and a new rash on his back. Denied abdominal pain, nausea, vomiting, diarrhea. While in Kenya, he was in a patient facing role while volunteering at a local hospital but denied sick contacts or traveling companions. No exposure to contaminated food or water. No sexual contacts. Prior to his trip he received Doxycycline for malaria prophylaxis, Hepatitis A and oral typhoid vaccines. Upon review of vaccination records, he did not receive the MMR vaccine as a child due to an adverse reaction in a relative. In the ED, he was placed in airborne precautions with vital signs notable for a fever of 39.3C and tachycardia. Physical exam with diffuse maculopapular, non-pruritic rash over back that was starting to coalesce and spread to the trunk, face and arms; sparing palms and soles. Noted to also have subtle bilateral injected conjunctiva and ulcerated oral lesions over the buccal mucosa. Workup revealed leukopenia and mild transaminase elevation. Negative blood cultures. Limited infectious workup initiated which later resulted positive for Rubeola. The patient was treated supportively and discharged home in good condition. Discussion: Measles, one of the most contagious infectious diseases, affects approximately 10.3 million people worldwide [2]. While measles is considered “eliminated” in the United States, rates continue to rise. In 2025, there has been a total of 1356 cases of Measles in the United States with 34% above the age of 20 and 13% requiring hospitalization [3]. Outbreaks often stem from unvaccinated international travelers [2]. This case highlights the importance of collecting a thorough vaccination history in this population to streamline infectious workup and reduce healthcare costs. Furthermore, this case underscores the critical need for continued vaccination advocacy in primary care to prevent resurgence of measles and other similar communicable and vaccine preventable illnesses.
-
Hypercalcemic Crisis After Open Mitral Valve Replacement
Andrew Sunwood, DO
59. Hypercalcemic Crisis After Open Mitral Valve Replacement Andrew Sunwood, DO Background: Hypercalcemic crisis is a rare manifestation of primary hyperparathyroidism characterized by a sudden increase in serum calcium levels to >14 mg/dL with symptoms of hypercalcemia including adverse gastrointestinal symptoms, abdominal pain, and even predisposition to cardiac arrhythmias. There is only one other documented case of hypercalcemic crisis occurring after open heart surgery. Case information: 69-year-old female with a history of primary osteoporosis on alendronate and valvular heart failure presented for mitral valve replacement. Preoperative lab work did not show evidence of electrolyte abnormalities. She under- went open bioprosthetic mitral valve replacement with tricuspid valve annuloplasty. She was taken to the cardiac intensive care unit for routine post-operative management and placed on dobutamine and furosemide infusions. Amiodarone was also started for post-operative atrial fibrillation/flutter. Post-operative day 3 (POD3), calcium levels were noted to rise to 10.5 mg/dL (normal 8.7-10.2 mg/dL). POD4, furosemide infusion was discontinued and calcium levels continued to rise to 11.2 mg/dL. The patient reported symptoms including increased sleepiness, brain fog, mild nausea, and decreased appetite. Further workup showed elevated intact parathyroid hormone 1310 pg/mL (normal 18-88 pg/mL), 25-hydroxyvitamin D 15.1 ng/mL (normal 20-50 ng/mL), and a negative parathyroid hormone-related peptide. Electrocardiogram showed sinus rhythm with a 1st degree AV block and QTc of 453 ms. A thyroid ultrasound demonstrated a 3 x 1.5 cm lesion on the left thyroid lobe, suspected parathyroid adenoma. Management included cinacalcet, normal saline infusion with IV furosemide for volume management, and zoledronic acid. Calcitonin was considered but was not on the hospital formulary. Serum calcium levels peaked on POD7 at 15.7 mg/dL with an ionized calcium of 2.15 mmol/L (normal 1.12-1.40 mmol/L). There was no evidence of arrhythmia apart from atrial fibrillation. She underwent parathyroidectomy revealing a left inferior parathyroid adenoma with immediate intraoperative normalization of parathyroid hormone levels post-resection. Serum calcium levels remained within normal limits for the remainder of her hospitalization, and she was discharged with vitamin D and calcium citrate. Discussion: Hypercalcemic crisis is a rare manifestation of hyperparathyroidism resulting in albumin-corrected calcium levels >14 mg/dL. This case illustrates hypercalcemic crisis in a patient likely with a longstanding parathyroid adenoma but without prior evidence of hypercalcemia. The sternotomy is the suspected trigger for the hypercalcemic crisis, whether from trauma and localized inflammation or related to cardiopulmonary bypass, with only one other documented case after coronary artery bypass grafting in a previously normocalcemic patient found to have a parathyroid adenoma. Management of hypercalcemic crisis includes stabilization through normal saline infusions and reduction of serum calcium levels with +cinacalcet, bisphosphonates, and calcitonin, if possible; and definitive treatment with parathyroidectomy. Post-valvular surgery patients especially require close moni- toring for signs of cardiac arrhythmias given the heightened risk post-operation.
-

Hydroxocobalamin in Septic Shock Management – Should It Be Introduced Sooner?
Linh Tang Taylor, MD; Cameron Miles Long, MD; and Omar Pandhair
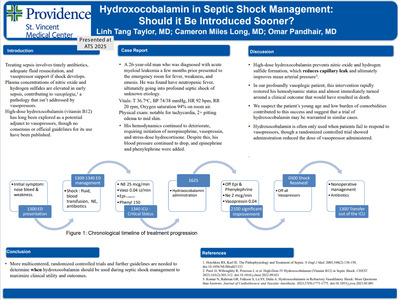
Introduction: Treating sepsis involves timely antibiotics, adequate fluid resuscitation, and vasopressor support if shock develops. Plasma concentrations of nitric oxide and hydrogen sulfides are elevated in early sepsis, contributing to vasoplegia,1 a pathology that isn’t addressed by vasopressors. High-dose hydroxocobalamin (vitamin B12) does, and therefore, has long been explored as a potential adjunct to vasopressors, though no consensus or official guidelines for its use have been published. Case Report: A 26-year-old man who was diagnosed with acute myeloid leukemia a few months prior presented to the emergency room for fever, weakness, and emesis. He was found to be profoundly hypotensive and was treated with aggressive fluid resuscitation and broad-spectrum antibiotics. His hemodynamics continued to deteriorate, requiring initiation of norepinephrine, vasopressin, and stress-dose hydrocortisone. Despite this, his mean arterial pressure continued to drop, and epinephrine and phenylephrine were added, with fleeting benefits. Ultimately, 5 g of hydroxocobalamin was administered intravenously. Within a few hours, vasopressor doses were able to be reduced significantly, and he was stable enough for abdominal imaging, which showed a perforated sigmoid colon abscess. Surgical intervention was deferred due to the extremely high risk of morbidity and death due to profound pancytopenia and the severity of septic shock. Within 15 hours, his shock improved with down titration of all vasopressors and normalization of lactate levels. He was transferred out of the ICU 21 hours after hydroxocobalamin administration and discharged home a week later Discussion: High-dose hydroxocobalamin prevents nitric oxide and hydrogen sulfide formation, which reduces capillary leak and ultimately improves mean arterial pressure3 . In our profoundly vasoplegic patient, this intervention rapidly restored his hemodynamic status and almost immediately turned around a clinical outcome that most likely would have resulted in death. We suspect the patient’s young age and low burden of comorbidities contributed to this success and suggest that a trial of hydroxocobalamin may be warranted in similar cases. Hydroxocobalamin is often only used when patients fail to respond to vasopressors, though a randomized controlled trial showed administration reduced the dose of vasopressor administered2 . More multicentered, randomized controlled trials and further guidelines are needed to determine when hydroxocobalamin should be used during septic shock management to maximize clinical utility and outcomes.
-

The Power of Two Questions: A Simplified Approach to Delirium Detection
Dalton VanderPol, MD; Laura Perry; and Shelley Schoepflin Sanders
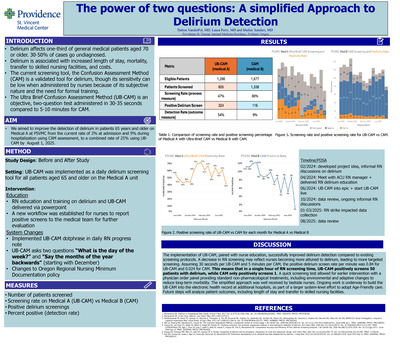
Background: Delirium affects one-third of general medical patients aged 70 or older. Patients with older age, preexisting dementia, or cognitive impairment are at increased risk of developing delirium. Delirium is associated with increased length of stay, mortality, transfer to skilled nursing facilities, and costs. Although the Confusion Assessment Method (CAM) is a validated tool for delirium, its sensitivity can be low when administered by nurses because of its subjective nature and the need for formal training. The Ultra Brief Confusion Assessment Method (UB-CAM) is an objective, two-question test administered in 30-35 seconds compared to 5-10 minutes for CAM. The objective was to increase the combined delirium detection rate from 12% to 25% by July 1, 2025. Methods: The UB-CAM was implemented as a daily delirium screening tool for all patients aged 65 and older on the Medical A unit. Nurses on Medical A received training on delirium recognition and the proper use of the UB-CAM. A new workflow was established for nurses to report positive screens to the medical team for further evaluation. The primary outcome was measured by the percentage of patients on Medical A who had a positive delirium screen, which was assessed at admission and daily by RNs using the UB-CAM. Results: 605 adults aged 65 and over were screened out of 1,286 eligible for a screening rate of 47%. The UB-CAM combined positive rate on Medical A from June 2024 to July 1, 2025, was 54% (324/605). On a comparable unit (Medical B) during the same time, 1338 adults age 65 and over were screened with the CAM out of 1,677 eligible for a screening rate of 80%. Of those screened, 9% (116/1338) screened positive. Conclusion: The implementation of UB-CAM, paired with nurse education, successfully improved delirium detection compared to existing screening protocols. A decrease in RN screening may reflect nurses becoming more attuned to delirium, leading to more targeted screening. Assuming 30 seconds per UB-CAM and 5 minutes per CAM, the positive delirium screen rate per minute was 0.84 for UB-CAM and 0.024 for CAM. This means that in a single hour of RN screening time, UB-CAM positively screens 50 patients with delirium, while CAM only positively screens 1. A quick screening test allowed for earlier intervention with a physician order panel providing standard non-pharmacological treatments, including environmental and adaptive changes to reduce long-term morbidity. The simplified approach was well received by bedside nurses. Ongoing work is underway to build the UB-CAM into the electronic health record at four additional units at two hospitals, as part of a larger system-level effort to adopt Age-Friendly care. Future steps will analyze patient outcomes, including length of stay and transfer to skilled nursing facilities.
-

A Fatal ‘Sepsis’: Intravascular Large B-Cell Lymphoma in Disguise
Jennifer L. Wong, DO1; Jared A. Shipley, MD2; and Christine Johnson, MD3
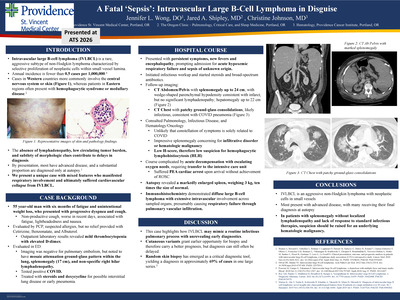
Introduction: Intravascular large B-cell lymphoma (IVLBCL) is a rare, aggressive subtype of non-Hodgkin lymphoma characterized by selective proliferation of neoplastic cells within small vessel lumina. Cases in Western countries more commonly involve the central nervous system or skin, whereas patients in Eastern regions often present with hemophagocytic syndrome or medullary disease. The absence of lymphadenopathy, low circulating tumor burden, and subtlety of morphologic clues contribute to delays in diagnosis. By presentation, most have advanced disease, and a substantial proportion are diagnosed only at autopsy. We report a unique case with mixed features who manifested respiratory involvement and ultimately suffered cardiovascular collapse. Case Presentation: A 55-year-old man with six months of fatigue and unintentional weight loss presented with progressive dyspnea and cough. Laboratory results revealed mild thrombocytopenia with elevated D-dimer, but imaging was negative for pulmonary embolism. There were ground-glass opacities concerning for early pneumonia and splenomegaly up to 17 cm. He tested positive for COVID, received fluids, and was discharged from the Emergency Department. His symptoms worsened with associated fevers and altered mentation, prompting hospital admission two weeks later. He was treated for sepsis of unclear source with empiric antibiotics and steroids without improvement. Follow up imaging showed further enlargement of the spleen to 24 cm, now with wedge-shaped parenchymal hypodensity consistent with infarct, but no significant lymphadenopathy. He acutely decompensated with escalating oxygen needs and was transferred to the intensive care unit, where he suffered a PEA cardiac arrest. He died despite prolonged resuscitative efforts. Autopsy revealed a markedly enlarged spleen, weighing 3 kg, ten times the size of normal. Immunohistochemistry demonstrated diffuse large B-cell lymphoma with extensive intravascular involvement across sampled organs, presumably causing respiratory failure through pulmonary vascular infiltration. Discussion: This case highlights how IVLBCL may mimic a routine infectious pulmonary process with unrevealing early diagnostics. Rapid clinical decline and lack of an optimal biopsy target make timely diagnosis and therapy difficult. Cutaneous variants grant an earlier opportunity for biopsy and therefore carry a better prognosis, but diagnosis can still often be delayed. Therefore, in patients with splenomegaly without localized lymphadenopathy and lack of response to standard infectious therapies, suspicion should be raised for an underlying hematologic malignancy.
-

When Jaundice Isn’t Just the Liver’s Fault: A Chilly Case of Cold Autoimmune Hemolytic Anemia
Jennifer Wong, DO and Shahana Baig-Lewis, MD, MPH
Introduction: Cold agglutinin disease (CAD), a subtype of autoimmune hemolytic anemia (AIHA), is characterized by IgM autoantibodies that target red blood cell antigens at low temperatures, leading to agglutination in cooler peripheral tissues and hemolysis. Predominately directed against the “I” or “i” antigens, cold agglutinins are commonly associated with Mycoplasma pneumoniae and infectious mononucleosis. Distinguishing warm AIHA from CAD can be challenging. Definitive diagnosis relies on antibody testing, with warm AIHA primarily involving IgG and CAD involving IgM. We report a case of CAD initially misattributed to drug-induced liver injury in the setting of a viral upper respiratory infection. Case Presentation: A 39-year-old woman with no significant past medical history presented with acute weakness and fevers. Symptoms were initially attributed to a viral illness and self-treated with Acetaminophen and Ibuprofen, achieving only partial relief. She visited her primary care provider the day prior to admission with new onset dark urine and jaundice. Concern for acute hepatitis prompted referral to the emergency department (ED). Initial evaluation revealed marked hyperbilirubinemia, elevated transaminases, and an echogenic liver on ultrasound, suggestive of fatty infiltration or chronic hepatocellular disease. She was admitted with presumed acetaminophen-induced acute hepatitis. Concurrently, a 4.6 g/dL drop in hemoglobin and positive antibody screen (Direct antiglobulin testing (DAT) positive for both IgG and C3), led to presumptive diagnosis of warm AIHA. Further workup revealed Epstein-Barr virus infection, confirming CAD. She was managed with supportive measures, counseled on avoidance of cold exposure, and discharged with close hematology follow-up. Discussion: CAD accounts for 20–25% of AIHA cases and may present insidiously or acutely in association with infections. Primary management includes avoidance of cold exposure, warming of intravenous fluids and transfusions, and treatment of underlying triggers. In severe cases, plasmapheresis may provide temporary benefit, and Rituximab-containing regimens are considered for primary CAD. This case highlights how initial anchoring to a presumed diagnosis of acute hepatitis delayed recognition of hemolysis. Cognitive biases—including premature closure, authority bias, framing bias, and availability bias—contributed to the initial misdiagnosis. Detailed history, attention to evolving data, and re-evaluation of the working diagnosis were essential in identifying CAD and implementing appropriate management.
Printing is not supported at the primary Gallery Thumbnail page. Please first navigate to a specific Image before printing.



{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}
{kind=link}